
Isolated Dental Anomalies Class I Angle: Supernumerary Teeth Anodontia
Isolated Dental Anomalies Class I Angle: Supernumerary Teeth Anodontia
You might also like
- 2anatomy of The Inguinal RegionDocument47 pages2anatomy of The Inguinal Regionthowell3No ratings yet
- Zhan Zhuang: How To Cultivate Energy With Standing Meditation PDFDocument22 pagesZhan Zhuang: How To Cultivate Energy With Standing Meditation PDFTomas1122100% (3)
- OriginalDocument10 pagesOriginalAmir IqbalNo ratings yet
- Classification of Anomaly2Document213 pagesClassification of Anomaly2samar yousif mohamed100% (1)
- Developmental TeethDocument53 pagesDevelopmental Teethlyli Star AngeloNo ratings yet
- Sakeena Assad PresentationDocument93 pagesSakeena Assad Presentationjenny girlNo ratings yet
- Lecture 4(1)Document5 pagesLecture 4(1)photo copyhemnNo ratings yet
- Genetic Disorders and SyndromesDocument77 pagesGenetic Disorders and Syndromesفاطمة الجش.No ratings yet
- Developmental Disorders of TeethDocument64 pagesDevelopmental Disorders of TeethPatterson MachariaNo ratings yet
- Variation in Tooth Morphology Anatomy PDFDocument9 pagesVariation in Tooth Morphology Anatomy PDFadriiianaiiioanaNo ratings yet
- 14 Tooth AbnormalitiesDocument152 pages14 Tooth Abnormalitiesحمزہ محبNo ratings yet
- Lec 1 Developmental Disturbances of TeetDocument17 pagesLec 1 Developmental Disturbances of TeetRana SayedNo ratings yet
- ( (Developmental Disturbances) ) : What Does Developmental Disturbance Mean??Document4 pages( (Developmental Disturbances) ) : What Does Developmental Disturbance Mean??Asma'a AlmawasNo ratings yet
- Oral Path PDFDocument367 pagesOral Path PDFAashka Desai100% (2)
- Classification of MalocclusionDocument29 pagesClassification of MalocclusionИскен АдылбековNo ratings yet
- Developmental Anomalies of The Teeth PDFDocument75 pagesDevelopmental Anomalies of The Teeth PDFIbrahim HashimiNo ratings yet
- ORAL PATHOLOGY Practical SpecimensDocument24 pagesORAL PATHOLOGY Practical SpecimensPravin PrajapatiNo ratings yet
- Developmental Disturbances of TeethDocument7 pagesDevelopmental Disturbances of TeethSherin ThomasNo ratings yet
- Tutorial in English Blok 5Document12 pagesTutorial in English Blok 5Ifata RDNo ratings yet
- 3435-Article Text-10228-1-10-20211027Document6 pages3435-Article Text-10228-1-10-20211027Irin Susan VargheseNo ratings yet
- Aetiology of MalocclusionDocument5 pagesAetiology of MalocclusionSRO oONo ratings yet
- Prof. Dr. Hasham Khan: Head Deptt. of Paediatric DentistryDocument143 pagesProf. Dr. Hasham Khan: Head Deptt. of Paediatric DentistryAbdul MohaiminNo ratings yet
- Supernumerary and Congenitally Absent Teeth A Literature ReviewDocument6 pagesSupernumerary and Congenitally Absent Teeth A Literature Reviewea6z9033No ratings yet
- Developmental Anomalies of TeethDocument97 pagesDevelopmental Anomalies of Teethtopuzoglualeyna5No ratings yet
- Anatomic Anomalies - LectureDocument10 pagesAnatomic Anomalies - LectureKhalid BhatNo ratings yet
- Prolonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkDocument5 pagesProlonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkRahulLife'sNo ratings yet
- Management of Delayed Eruption of Perma-Nent Maxillary Incisor Associated With The Presence of Supernumerary Teeth: A Case ReportDocument5 pagesManagement of Delayed Eruption of Perma-Nent Maxillary Incisor Associated With The Presence of Supernumerary Teeth: A Case ReportFelianda ThaliaNo ratings yet
- Abnormalities of Tooth Number: Two TypesDocument28 pagesAbnormalities of Tooth Number: Two TypesKyaw Myo HtetNo ratings yet
- Prostho Rehabilitation - HypodontiaDocument24 pagesProstho Rehabilitation - HypodontiaAmniAzmiNo ratings yet
- Supernumerary Lateral IncisorDocument2 pagesSupernumerary Lateral IncisorNatasa StojkovicNo ratings yet
- Developmental Anomalies of DentitionDocument54 pagesDevelopmental Anomalies of DentitionSowmiya N.MNo ratings yet
- PBL Oral BiologyDocument12 pagesPBL Oral BiologyhusunasanNo ratings yet
- Mal OcclusionDocument3 pagesMal OcclusionrichardananNo ratings yet
- CL 1 Part 2 PDFDocument11 pagesCL 1 Part 2 PDFdhurgham kaabiNo ratings yet
- Sequelae of TraumaDocument27 pagesSequelae of TraumaDr.O.R.GANESAMURTHINo ratings yet
- Oral Patho Lec Midterm ReviewerDocument165 pagesOral Patho Lec Midterm Revieweralvarez.sofiadennieceNo ratings yet
- Pedo2013 14Document189 pagesPedo2013 14Vladimir Argirovic100% (4)
- Rabbit and Rodent DentistryDocument6 pagesRabbit and Rodent DentistrySebastián Ordóñez RamírezNo ratings yet
- Prosthetic Implications of Dental Anomalies and ProblemsDocument18 pagesProsthetic Implications of Dental Anomalies and ProblemsDharshiniNo ratings yet
- Oral Surgery: Indication & Contra-Indication of ExtractionDocument9 pagesOral Surgery: Indication & Contra-Indication of Extractionتركيه تركيهNo ratings yet
- Session 10 TeethDocument100 pagesSession 10 TeethZNo ratings yet
- Odonto ExoticosDocument14 pagesOdonto ExoticosPedro FontaniveNo ratings yet
- Orthodontic Management in Cleft PatientsDocument4 pagesOrthodontic Management in Cleft Patientsdent.dreamer7No ratings yet
- Presentation2 Impaction (Online)Document91 pagesPresentation2 Impaction (Online)lola abualillNo ratings yet
- Indication and Contraindication of ExodontiaDocument9 pagesIndication and Contraindication of ExodontiaSagad AlaaNo ratings yet
- 15-Traumatic Injuries of The TeethDocument79 pages15-Traumatic Injuries of The Teethحمزہ محبNo ratings yet
- Pediatric Pathology: Glo Arby Arguelles, DMDDocument27 pagesPediatric Pathology: Glo Arby Arguelles, DMDRayne GelleNo ratings yet
- Management of Developing DentitionDocument51 pagesManagement of Developing Dentitionahmed alshaariNo ratings yet
- Anamolies of Formation and Eruption For Class 22Document76 pagesAnamolies of Formation and Eruption For Class 22Nihaz 72No ratings yet
- Developmental Disturbances of Tooth PDFDocument97 pagesDevelopmental Disturbances of Tooth PDFEmad AlriashyNo ratings yet
- Preventive & Interceptive OrthodonticsDocument50 pagesPreventive & Interceptive OrthodonticsDeebah ChoudharyNo ratings yet
- Traumatic Injuries of TeethDocument6 pagesTraumatic Injuries of TeethMiguel lisayNo ratings yet
- Oral PathologyDocument184 pagesOral Pathologyyalahopa100% (1)
- Abnormalities of Teeth Eruption, Structure, Form, Number, and SizeDocument48 pagesAbnormalities of Teeth Eruption, Structure, Form, Number, and SizeNoor AlsanouriNo ratings yet
- Animal DentistryDocument10 pagesAnimal DentistryFei Fei LoNo ratings yet
- Supernumerary Teeth - Fourth Molars: Bilateral Maxillary Distomolars An Extremely Rare Case ReportDocument4 pagesSupernumerary Teeth - Fourth Molars: Bilateral Maxillary Distomolars An Extremely Rare Case ReportMichael XuNo ratings yet
- Supernumerary MesiodensDocument17 pagesSupernumerary MesiodenssabeerNo ratings yet
- APznzabu1Ci9p9yRpxFqJSukJAe2 6rzeDQRKy GGsZNB1jUFPKmnLhAb3H17ZdDocument24 pagesAPznzabu1Ci9p9yRpxFqJSukJAe2 6rzeDQRKy GGsZNB1jUFPKmnLhAb3H17Zdclassybrands0No ratings yet
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- DRUG STUDY 2023 WARD POTASSIUM CHLORIDE AutosavedDocument2 pagesDRUG STUDY 2023 WARD POTASSIUM CHLORIDE AutosavedMary Grace AgataNo ratings yet
- Toc PDFDocument12 pagesToc PDFSOURAV DAS100% (1)
- MICROPARA Lab Exercise 2 DISINFECTION AND STERILIZATIONDocument6 pagesMICROPARA Lab Exercise 2 DISINFECTION AND STERILIZATIONMa. Isabel A. EnriquezNo ratings yet
- Antibiotic Sensitivity Pattern and Plasmid Profile of Bacteria Isolated From Diabetic Ulcers in Mbano Metropolis, Imo State, Southeastern NigeriaDocument9 pagesAntibiotic Sensitivity Pattern and Plasmid Profile of Bacteria Isolated From Diabetic Ulcers in Mbano Metropolis, Imo State, Southeastern NigeriaUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Unit 7. Sympathomimetics and SympatholyticsDocument44 pagesUnit 7. Sympathomimetics and SympatholyticsApril Mergelle Lapuz100% (2)
- Bo5550077 PDFDocument4 pagesBo5550077 PDFBlagoje0% (1)
- Reading Part A Text BookletDocument4 pagesReading Part A Text BookletWisdomofGod OfficialNo ratings yet
- Pulmonology Short CasesDocument10 pagesPulmonology Short CasesRZ Ng100% (1)
- List of Culture Media Used in Microbiology With Their Uses - MicrobiologyDocument14 pagesList of Culture Media Used in Microbiology With Their Uses - MicrobiologyRatan YadavNo ratings yet
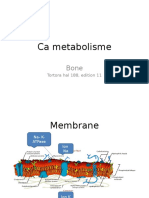
- Ca Metabolisme: Tortora Hal 188, Edition 11Document21 pagesCa Metabolisme: Tortora Hal 188, Edition 11Julian HuningkorNo ratings yet
- Mind Therepy PDFDocument6 pagesMind Therepy PDFShaurya SinghNo ratings yet
- Case Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1Document11 pagesCase Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1J.r. MercadoNo ratings yet
- Anterior Repositioning Appliance For Relief of TMD in Conjunction With Definitive Orthodontic TreatmentDocument10 pagesAnterior Repositioning Appliance For Relief of TMD in Conjunction With Definitive Orthodontic TreatmentumadeviNo ratings yet
- TechSpec - Infusomat PDocument1 pageTechSpec - Infusomat PANISA DESYNo ratings yet
- Home Health Care and Diabetes ManagementDocument5 pagesHome Health Care and Diabetes ManagementIndia Home Health CareNo ratings yet
- Links Library Find Out If You WonDocument10 pagesLinks Library Find Out If You WonusmleNo ratings yet
- Apnea of Prematurity: UnderstandingDocument2 pagesApnea of Prematurity: UnderstandingEmil JaniakNo ratings yet
- Meningitis (Physical Exam)Document6 pagesMeningitis (Physical Exam)MohammadAwitNo ratings yet
- History of Drug Discovery 1Document7 pagesHistory of Drug Discovery 1Brent FontanillaNo ratings yet
- Side Effect Reporting FormDocument2 pagesSide Effect Reporting FormBBB.AAANo ratings yet
- Biopad BiosprayDocument24 pagesBiopad BiosprayLuci ContiuNo ratings yet
- Concept Paper InsulinDocument3 pagesConcept Paper InsulinCrystine Jaye SenadreNo ratings yet
- 01 Homepage - Apr.1Document4 pages01 Homepage - Apr.1atpfacebookNo ratings yet
- MS CA and EN Ans KeyDocument15 pagesMS CA and EN Ans KeyAydh Dim-Mac RsclNo ratings yet
- Drug StudyDocument5 pagesDrug StudyOlivia Solomon100% (1)
- Formulat 19Document1 pageFormulat 19Kanwal SheikhNo ratings yet
- Guiding Documents For Zonal & Sub-Zonal & Port Offices 17.06.2011Document483 pagesGuiding Documents For Zonal & Sub-Zonal & Port Offices 17.06.2011rk7bpsNo ratings yet
- 2013 ASB Oludare HovorkaDocument2 pages2013 ASB Oludare HovorkaSimisola OludareNo ratings yet
























































































Download as ppt, pdf, or txt
You might also like
- 2anatomy of The Inguinal RegionDocument47 pages2anatomy of The Inguinal Regionthowell3No ratings yet
- Zhan Zhuang: How To Cultivate Energy With Standing Meditation PDFDocument22 pagesZhan Zhuang: How To Cultivate Energy With Standing Meditation PDFTomas1122100% (3)
- OriginalDocument10 pagesOriginalAmir IqbalNo ratings yet
- Classification of Anomaly2Document213 pagesClassification of Anomaly2samar yousif mohamed100% (1)
- Developmental TeethDocument53 pagesDevelopmental Teethlyli Star AngeloNo ratings yet
- Sakeena Assad PresentationDocument93 pagesSakeena Assad Presentationjenny girlNo ratings yet
- Lecture 4(1)Document5 pagesLecture 4(1)photo copyhemnNo ratings yet
- Genetic Disorders and SyndromesDocument77 pagesGenetic Disorders and Syndromesفاطمة الجش.No ratings yet
- Developmental Disorders of TeethDocument64 pagesDevelopmental Disorders of TeethPatterson MachariaNo ratings yet
- Variation in Tooth Morphology Anatomy PDFDocument9 pagesVariation in Tooth Morphology Anatomy PDFadriiianaiiioanaNo ratings yet
- 14 Tooth AbnormalitiesDocument152 pages14 Tooth Abnormalitiesحمزہ محبNo ratings yet
- Lec 1 Developmental Disturbances of TeetDocument17 pagesLec 1 Developmental Disturbances of TeetRana SayedNo ratings yet
- ( (Developmental Disturbances) ) : What Does Developmental Disturbance Mean??Document4 pages( (Developmental Disturbances) ) : What Does Developmental Disturbance Mean??Asma'a AlmawasNo ratings yet
- Oral Path PDFDocument367 pagesOral Path PDFAashka Desai100% (2)
- Classification of MalocclusionDocument29 pagesClassification of MalocclusionИскен АдылбековNo ratings yet
- Developmental Anomalies of The Teeth PDFDocument75 pagesDevelopmental Anomalies of The Teeth PDFIbrahim HashimiNo ratings yet
- ORAL PATHOLOGY Practical SpecimensDocument24 pagesORAL PATHOLOGY Practical SpecimensPravin PrajapatiNo ratings yet
- Developmental Disturbances of TeethDocument7 pagesDevelopmental Disturbances of TeethSherin ThomasNo ratings yet
- Tutorial in English Blok 5Document12 pagesTutorial in English Blok 5Ifata RDNo ratings yet
- 3435-Article Text-10228-1-10-20211027Document6 pages3435-Article Text-10228-1-10-20211027Irin Susan VargheseNo ratings yet
- Aetiology of MalocclusionDocument5 pagesAetiology of MalocclusionSRO oONo ratings yet
- Prof. Dr. Hasham Khan: Head Deptt. of Paediatric DentistryDocument143 pagesProf. Dr. Hasham Khan: Head Deptt. of Paediatric DentistryAbdul MohaiminNo ratings yet
- Supernumerary and Congenitally Absent Teeth A Literature ReviewDocument6 pagesSupernumerary and Congenitally Absent Teeth A Literature Reviewea6z9033No ratings yet
- Developmental Anomalies of TeethDocument97 pagesDevelopmental Anomalies of Teethtopuzoglualeyna5No ratings yet
- Anatomic Anomalies - LectureDocument10 pagesAnatomic Anomalies - LectureKhalid BhatNo ratings yet
- Prolonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkDocument5 pagesProlonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkRahulLife'sNo ratings yet
- Management of Delayed Eruption of Perma-Nent Maxillary Incisor Associated With The Presence of Supernumerary Teeth: A Case ReportDocument5 pagesManagement of Delayed Eruption of Perma-Nent Maxillary Incisor Associated With The Presence of Supernumerary Teeth: A Case ReportFelianda ThaliaNo ratings yet
- Abnormalities of Tooth Number: Two TypesDocument28 pagesAbnormalities of Tooth Number: Two TypesKyaw Myo HtetNo ratings yet
- Prostho Rehabilitation - HypodontiaDocument24 pagesProstho Rehabilitation - HypodontiaAmniAzmiNo ratings yet
- Supernumerary Lateral IncisorDocument2 pagesSupernumerary Lateral IncisorNatasa StojkovicNo ratings yet
- Developmental Anomalies of DentitionDocument54 pagesDevelopmental Anomalies of DentitionSowmiya N.MNo ratings yet
- PBL Oral BiologyDocument12 pagesPBL Oral BiologyhusunasanNo ratings yet
- Mal OcclusionDocument3 pagesMal OcclusionrichardananNo ratings yet
- CL 1 Part 2 PDFDocument11 pagesCL 1 Part 2 PDFdhurgham kaabiNo ratings yet
- Sequelae of TraumaDocument27 pagesSequelae of TraumaDr.O.R.GANESAMURTHINo ratings yet
- Oral Patho Lec Midterm ReviewerDocument165 pagesOral Patho Lec Midterm Revieweralvarez.sofiadennieceNo ratings yet
- Pedo2013 14Document189 pagesPedo2013 14Vladimir Argirovic100% (4)
- Rabbit and Rodent DentistryDocument6 pagesRabbit and Rodent DentistrySebastián Ordóñez RamírezNo ratings yet
- Prosthetic Implications of Dental Anomalies and ProblemsDocument18 pagesProsthetic Implications of Dental Anomalies and ProblemsDharshiniNo ratings yet
- Oral Surgery: Indication & Contra-Indication of ExtractionDocument9 pagesOral Surgery: Indication & Contra-Indication of Extractionتركيه تركيهNo ratings yet
- Session 10 TeethDocument100 pagesSession 10 TeethZNo ratings yet
- Odonto ExoticosDocument14 pagesOdonto ExoticosPedro FontaniveNo ratings yet
- Orthodontic Management in Cleft PatientsDocument4 pagesOrthodontic Management in Cleft Patientsdent.dreamer7No ratings yet
- Presentation2 Impaction (Online)Document91 pagesPresentation2 Impaction (Online)lola abualillNo ratings yet
- Indication and Contraindication of ExodontiaDocument9 pagesIndication and Contraindication of ExodontiaSagad AlaaNo ratings yet
- 15-Traumatic Injuries of The TeethDocument79 pages15-Traumatic Injuries of The Teethحمزہ محبNo ratings yet
- Pediatric Pathology: Glo Arby Arguelles, DMDDocument27 pagesPediatric Pathology: Glo Arby Arguelles, DMDRayne GelleNo ratings yet
- Management of Developing DentitionDocument51 pagesManagement of Developing Dentitionahmed alshaariNo ratings yet
- Anamolies of Formation and Eruption For Class 22Document76 pagesAnamolies of Formation and Eruption For Class 22Nihaz 72No ratings yet
- Developmental Disturbances of Tooth PDFDocument97 pagesDevelopmental Disturbances of Tooth PDFEmad AlriashyNo ratings yet
- Preventive & Interceptive OrthodonticsDocument50 pagesPreventive & Interceptive OrthodonticsDeebah ChoudharyNo ratings yet
- Traumatic Injuries of TeethDocument6 pagesTraumatic Injuries of TeethMiguel lisayNo ratings yet
- Oral PathologyDocument184 pagesOral Pathologyyalahopa100% (1)
- Abnormalities of Teeth Eruption, Structure, Form, Number, and SizeDocument48 pagesAbnormalities of Teeth Eruption, Structure, Form, Number, and SizeNoor AlsanouriNo ratings yet
- Animal DentistryDocument10 pagesAnimal DentistryFei Fei LoNo ratings yet
- Supernumerary Teeth - Fourth Molars: Bilateral Maxillary Distomolars An Extremely Rare Case ReportDocument4 pagesSupernumerary Teeth - Fourth Molars: Bilateral Maxillary Distomolars An Extremely Rare Case ReportMichael XuNo ratings yet
- Supernumerary MesiodensDocument17 pagesSupernumerary MesiodenssabeerNo ratings yet
- APznzabu1Ci9p9yRpxFqJSukJAe2 6rzeDQRKy GGsZNB1jUFPKmnLhAb3H17ZdDocument24 pagesAPznzabu1Ci9p9yRpxFqJSukJAe2 6rzeDQRKy GGsZNB1jUFPKmnLhAb3H17Zdclassybrands0No ratings yet
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- DRUG STUDY 2023 WARD POTASSIUM CHLORIDE AutosavedDocument2 pagesDRUG STUDY 2023 WARD POTASSIUM CHLORIDE AutosavedMary Grace AgataNo ratings yet
- Toc PDFDocument12 pagesToc PDFSOURAV DAS100% (1)
- MICROPARA Lab Exercise 2 DISINFECTION AND STERILIZATIONDocument6 pagesMICROPARA Lab Exercise 2 DISINFECTION AND STERILIZATIONMa. Isabel A. EnriquezNo ratings yet
- Antibiotic Sensitivity Pattern and Plasmid Profile of Bacteria Isolated From Diabetic Ulcers in Mbano Metropolis, Imo State, Southeastern NigeriaDocument9 pagesAntibiotic Sensitivity Pattern and Plasmid Profile of Bacteria Isolated From Diabetic Ulcers in Mbano Metropolis, Imo State, Southeastern NigeriaUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Unit 7. Sympathomimetics and SympatholyticsDocument44 pagesUnit 7. Sympathomimetics and SympatholyticsApril Mergelle Lapuz100% (2)
- Bo5550077 PDFDocument4 pagesBo5550077 PDFBlagoje0% (1)
- Reading Part A Text BookletDocument4 pagesReading Part A Text BookletWisdomofGod OfficialNo ratings yet
- Pulmonology Short CasesDocument10 pagesPulmonology Short CasesRZ Ng100% (1)
- List of Culture Media Used in Microbiology With Their Uses - MicrobiologyDocument14 pagesList of Culture Media Used in Microbiology With Their Uses - MicrobiologyRatan YadavNo ratings yet
- Ca Metabolisme: Tortora Hal 188, Edition 11Document21 pagesCa Metabolisme: Tortora Hal 188, Edition 11Julian HuningkorNo ratings yet
- Mind Therepy PDFDocument6 pagesMind Therepy PDFShaurya SinghNo ratings yet
- Case Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1Document11 pagesCase Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1J.r. MercadoNo ratings yet
- Anterior Repositioning Appliance For Relief of TMD in Conjunction With Definitive Orthodontic TreatmentDocument10 pagesAnterior Repositioning Appliance For Relief of TMD in Conjunction With Definitive Orthodontic TreatmentumadeviNo ratings yet
- TechSpec - Infusomat PDocument1 pageTechSpec - Infusomat PANISA DESYNo ratings yet
- Home Health Care and Diabetes ManagementDocument5 pagesHome Health Care and Diabetes ManagementIndia Home Health CareNo ratings yet
- Links Library Find Out If You WonDocument10 pagesLinks Library Find Out If You WonusmleNo ratings yet
- Apnea of Prematurity: UnderstandingDocument2 pagesApnea of Prematurity: UnderstandingEmil JaniakNo ratings yet
- Meningitis (Physical Exam)Document6 pagesMeningitis (Physical Exam)MohammadAwitNo ratings yet
- History of Drug Discovery 1Document7 pagesHistory of Drug Discovery 1Brent FontanillaNo ratings yet
- Side Effect Reporting FormDocument2 pagesSide Effect Reporting FormBBB.AAANo ratings yet
- Biopad BiosprayDocument24 pagesBiopad BiosprayLuci ContiuNo ratings yet
- Concept Paper InsulinDocument3 pagesConcept Paper InsulinCrystine Jaye SenadreNo ratings yet
- 01 Homepage - Apr.1Document4 pages01 Homepage - Apr.1atpfacebookNo ratings yet
- MS CA and EN Ans KeyDocument15 pagesMS CA and EN Ans KeyAydh Dim-Mac RsclNo ratings yet
- Drug StudyDocument5 pagesDrug StudyOlivia Solomon100% (1)
- Formulat 19Document1 pageFormulat 19Kanwal SheikhNo ratings yet
- Guiding Documents For Zonal & Sub-Zonal & Port Offices 17.06.2011Document483 pagesGuiding Documents For Zonal & Sub-Zonal & Port Offices 17.06.2011rk7bpsNo ratings yet
- 2013 ASB Oludare HovorkaDocument2 pages2013 ASB Oludare HovorkaSimisola OludareNo ratings yet