Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Case Study AppendicitisDocument58 pagesCase Study AppendicitisArianne Joy Balon100% (2)
- Detailed Design - To Be ApprovedDocument28 pagesDetailed Design - To Be ApprovedGeorgiana Cătălina MihalceaNo ratings yet
- Schwartz's Principles of Surgery - Appendix PDFDocument22 pagesSchwartz's Principles of Surgery - Appendix PDFPhạm Tuân100% (1)
- Emergency of ObstetryDocument14 pagesEmergency of ObstetryPratikaLawrenceSasubeNo ratings yet
- Penyakit Dan Gangguan SyarafDocument6 pagesPenyakit Dan Gangguan SyarafPratikaLawrenceSasubeNo ratings yet
- Hepatitis Virus: Department Ilmu Kesehatan Anak FK UKIDocument46 pagesHepatitis Virus: Department Ilmu Kesehatan Anak FK UKIPratikaLawrenceSasubeNo ratings yet
- Sindrom Cushing: Donnie Lumban Gaol Departemen Ilmu Penyakit Dalam FkukiDocument38 pagesSindrom Cushing: Donnie Lumban Gaol Departemen Ilmu Penyakit Dalam FkukiPratikaLawrenceSasubeNo ratings yet
- Gastrointestinal Tract Presentation-1Document85 pagesGastrointestinal Tract Presentation-1PratikaLawrenceSasubeNo ratings yet
- PathologyDocument8 pagesPathologyJemimah Tomarong DespabeladeroNo ratings yet
- Acute Appendicitis in Adults ManagementDocument16 pagesAcute Appendicitis in Adults ManagementPriscila Tobar AlcántarNo ratings yet
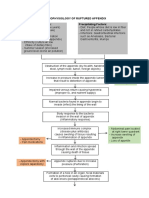
- Pathophysiology of Ruptured AppendixDocument2 pagesPathophysiology of Ruptured AppendixAya PaquitNo ratings yet
- Guidelines and Prescribed Format of Project ReportDocument14 pagesGuidelines and Prescribed Format of Project ReportJordan JanardanNo ratings yet
- Bicol Medical Center Department of Surgery: AppendicitisDocument60 pagesBicol Medical Center Department of Surgery: AppendicitisHenry Bona100% (1)
- Anatomy of AppendixDocument6 pagesAnatomy of AppendixNikhil Siddhartha AtchalaNo ratings yet
- Medical Surgical NursingDocument11 pagesMedical Surgical NursingJa DimasNo ratings yet
- AppendicitisDocument17 pagesAppendicitisAhmed Halaby100% (1)
- Harrison's Practice Abdominal Pain DefinitionDocument27 pagesHarrison's Practice Abdominal Pain Definitionearicasilla100% (2)
- Textbook Acute Care General Surgery Workup and Management 1St Edition Dale A Dangleben Ebook All Chapter PDFDocument53 pagesTextbook Acute Care General Surgery Workup and Management 1St Edition Dale A Dangleben Ebook All Chapter PDFsaundra.hawn119100% (21)
- A Case Study of RupturedDocument12 pagesA Case Study of RupturedkisNo ratings yet
- Guidelines For BTP Report PDFDocument14 pagesGuidelines For BTP Report PDFAyush GuptaNo ratings yet
- Appendicitis Case PresentationDocument52 pagesAppendicitis Case PresentationNico Avellana100% (2)
- Enzyme NutritionDocument7 pagesEnzyme NutritionViliaminaNo ratings yet
- Jurnal InvaginasiDocument3 pagesJurnal InvaginasiAbdurrohman IzzuddinNo ratings yet
- Guide On The Use of The Design & Build / Turnkey Conditions of ContractDocument3 pagesGuide On The Use of The Design & Build / Turnkey Conditions of ContractupdazNo ratings yet
- PS 3103Document9 pagesPS 3103JayeshNo ratings yet
- Case Study For Peri-Appendiceal AbcessDocument79 pagesCase Study For Peri-Appendiceal Abcessmarife100% (5)
- EGB101 - S1 - 2024 - Assessment 1a - Scoping Study TemplateDocument6 pagesEGB101 - S1 - 2024 - Assessment 1a - Scoping Study Templateabdullah.gujjarr.171No ratings yet
- Appendectomy - Better Health ChannelDocument6 pagesAppendectomy - Better Health ChannelBilal AhmadNo ratings yet
- მსხვილი ნაწლავი 1Document36 pagesმსხვილი ნაწლავი 1Malak A MahadeenNo ratings yet
- Seminar Report FormatDocument6 pagesSeminar Report FormatSunil KotthakotaNo ratings yet
- (英文) HART实用命令详解 PDFDocument11 pages(英文) HART实用命令详解 PDFvirgil guimanNo ratings yet
- Management of Acute Appendicitis in AdultsDocument28 pagesManagement of Acute Appendicitis in Adultscandra1991100% (1)
- Appendix 1 List of Buffer Memory AddressesDocument26 pagesAppendix 1 List of Buffer Memory AddressesFeby Aries DarmawanNo ratings yet
- سعقلثاي 8.5Document309 pagesسعقلثاي 8.5Simina Întuneric100% (1)
- AppendectomyDocument40 pagesAppendectomyenny100% (12)