Download as pptx, pdf, or txt
You might also like
- NBME 11 BLOCK 1-4 (With Answers)Document204 pagesNBME 11 BLOCK 1-4 (With Answers)kh60% (5)
- The Doctor Will See You Now PDF 130kDocument8 pagesThe Doctor Will See You Now PDF 130kperry261No ratings yet
- Lifestyle DiseasesDocument44 pagesLifestyle Diseaseskyro draxNo ratings yet
- Liver Function TestsDocument4 pagesLiver Function TestsAnbaraj ArunNo ratings yet
- An Update On Menopause ManagementDocument10 pagesAn Update On Menopause ManagementJuan FranciscoNo ratings yet
- AHNS 2019 Final ProgramDocument140 pagesAHNS 2019 Final ProgramAbhishek Kumar RamadhinNo ratings yet
- Fever of Unknown Origin - Clinical Overview of Classic - and - Current ConceptsDocument20 pagesFever of Unknown Origin - Clinical Overview of Classic - and - Current ConceptsPedro Luz da RosaNo ratings yet
- ABG Practice Question AnswersDocument7 pagesABG Practice Question AnswersVidit JoshiNo ratings yet
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 16: HematologyFrom EverandComplementary and Alternative Medical Lab Testing Part 16: HematologyNo ratings yet
- Cirrhosis Jol 2009Document54 pagesCirrhosis Jol 2009SaaraAlleyahAlAnazi100% (1)
- Initial Investigation and Managenement Benign Ovariam MassesDocument12 pagesInitial Investigation and Managenement Benign Ovariam MassesleslyNo ratings yet
- Alcoholic Liver DiseaseDocument5 pagesAlcoholic Liver DiseaseSucii Sekar NingrumNo ratings yet
- VaginitisDocument54 pagesVaginitisgloria100% (1)
- Liver Tests SlidesDocument65 pagesLiver Tests SlidesDokter MuhammadNo ratings yet
- 8 BilirubinDocument25 pages8 BilirubinTagreed DerarNo ratings yet
- Pathology of Alcoholic Liver DiseaseDocument7 pagesPathology of Alcoholic Liver DiseasehghNo ratings yet
- Alcoholic Liver DiseaseDocument22 pagesAlcoholic Liver DiseaseVikramjeet SinghNo ratings yet
- Non Hodgkin LymphomaDocument53 pagesNon Hodgkin LymphomaMeilina Elin WardhaniNo ratings yet
- Perimenopausal Bleeding and Bleeding After MenopauseDocument5 pagesPerimenopausal Bleeding and Bleeding After MenopauseAnonymous KwWTUPjXNo ratings yet
- Elevated Liver Enzymes PDFDocument63 pagesElevated Liver Enzymes PDFPrakarsa Adi Daya NusantaraNo ratings yet
- Alcoholic Liver Disease HarrisonDocument3 pagesAlcoholic Liver Disease HarrisonJesly Charlies0% (1)
- The Side Effects of Common Psychiatric DrugsDocument40 pagesThe Side Effects of Common Psychiatric DrugsSFLD0% (1)
- Hidradenitis Suppurativa: A Diagnostic AtlasFrom EverandHidradenitis Suppurativa: A Diagnostic AtlasGiuseppe MicaliNo ratings yet
- Liver Function Testing PDFDocument2 pagesLiver Function Testing PDFRajesh KumarNo ratings yet
- Substance-Related DisorderDocument2 pagesSubstance-Related DisorderRichelle Delos ReyesNo ratings yet
- Hypotension: Causes, Incidence, and Risk FactorsDocument4 pagesHypotension: Causes, Incidence, and Risk Factorsclubsanatate100% (1)
- EssayDocument8 pagesEssayapi-308498731No ratings yet
- Graves' Disease & PregnancyDocument19 pagesGraves' Disease & Pregnancyrajan kumar100% (1)
- UTI LectureDocument62 pagesUTI LectureHaidar ShiddiqNo ratings yet
- Adrenal Gland OSCEDocument14 pagesAdrenal Gland OSCEOmar AttaNo ratings yet
- Adverse Effects of FluoroquinolonesDocument10 pagesAdverse Effects of FluoroquinolonesAvelox FloxNo ratings yet
- Interpret Liver TestsDocument4 pagesInterpret Liver TestsKaram Ali ShahNo ratings yet
- LymphomaDocument5 pagesLymphomaBlossom Wawa IINo ratings yet
- Hyper & Hypothyroidism LectureDocument1 pageHyper & Hypothyroidism LectureJhevilin RMNo ratings yet
- 11 Tramadol OverdoseDocument5 pages11 Tramadol OverdoseMohamed ElkhodaryNo ratings yet
- UTI and Asymptomatic Bacteriuria TEACHING SLIDESDocument43 pagesUTI and Asymptomatic Bacteriuria TEACHING SLIDESJana DbaibouNo ratings yet
- Inflammatory Bowel DiseaseDocument59 pagesInflammatory Bowel DiseaseLala Rahma Qodriyan SofiakmiNo ratings yet
- Post-Vaccination Side Effects Following The Second Dose of COVID-19 Vaccine Among Health Care WorkersDocument7 pagesPost-Vaccination Side Effects Following The Second Dose of COVID-19 Vaccine Among Health Care WorkersIJPHS100% (1)
- Hyperthyroidism and Thyroid Storm: Tintinalli Chapter 215 12/15/05Document44 pagesHyperthyroidism and Thyroid Storm: Tintinalli Chapter 215 12/15/05Charith KumaraNo ratings yet
- An Interesting Case of Treatment Resistant AsthmaDocument39 pagesAn Interesting Case of Treatment Resistant AsthmaushapadminivadivelswamyNo ratings yet
- Important Complications of Chronic Kidney Disease PDFDocument4 pagesImportant Complications of Chronic Kidney Disease PDFDrBishnu Prasad MahalaNo ratings yet
- Physician & Dialysis - Economics Matters: Umesh KhannaDocument3 pagesPhysician & Dialysis - Economics Matters: Umesh Khannaunfriendly.gy2268No ratings yet
- Breast Pain - History TakingDocument6 pagesBreast Pain - History TakingValencia FooNo ratings yet
- Thyroid Disease AlgorithmsDocument29 pagesThyroid Disease AlgorithmsGoh Chong Aik100% (2)
- Ospolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)Document7 pagesOspolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)ddandan_2No ratings yet
- Drug-Induced QT Interval ProlongationDocument13 pagesDrug-Induced QT Interval ProlongationgeoaislaNo ratings yet
- Journal Herpes Simplex EncephalitisDocument2 pagesJournal Herpes Simplex EncephalitissavinaumarNo ratings yet
- Dental Health and Overall Health4Document3 pagesDental Health and Overall Health4Adinda Vashia OktegiandaNo ratings yet
- The Role of Diet in Multiple Sclerosis - A ReviewDocument16 pagesThe Role of Diet in Multiple Sclerosis - A ReviewHabib G. Moutran BarrosoNo ratings yet
- Practical Gastroenterology and Hepatology Board Review ToolkitFrom EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultNo ratings yet
- Effects of Human Exposure To Hormone-Disrupting Chemicals Examined in Landmark UN ReportDocument3 pagesEffects of Human Exposure To Hormone-Disrupting Chemicals Examined in Landmark UN ReportMaja KazazicNo ratings yet
- Neurological Pharmacology PresentationDocument49 pagesNeurological Pharmacology PresentationAmit MartinNo ratings yet
- Nutritional Healing For Multiple SclerosisDocument6 pagesNutritional Healing For Multiple SclerosisBrian Hunter Levins Jr.No ratings yet
- Antiphospholipid SyndromeDocument16 pagesAntiphospholipid Syndrometal26No ratings yet
- FCO - Cancer Cachexia SyndromeDocument8 pagesFCO - Cancer Cachexia SyndromeThanos ZafeiriouNo ratings yet
- HIV-associated Nephropathy (HIVAN) - UpToDate PDFDocument22 pagesHIV-associated Nephropathy (HIVAN) - UpToDate PDFMuh Deriyatmiko BastamanNo ratings yet
- Schizophrenia: Onset of Symptoms Typically Occurs in Young Adulthood, With Around 0.4-0.6% of TheDocument3 pagesSchizophrenia: Onset of Symptoms Typically Occurs in Young Adulthood, With Around 0.4-0.6% of ThepapatukNo ratings yet
- Human and Health Rights in Relation To Sustainable2Document17 pagesHuman and Health Rights in Relation To Sustainable2ptkabworldNo ratings yet
- The Inflammatory ProcessDocument7 pagesThe Inflammatory ProcessDaniul ConuiNo ratings yet
- Acute PericarditisDocument14 pagesAcute PericarditisMila Ccasani100% (1)
- Cancer Prevention - The Causes and Prevention of Cancer Volume 1 (Cancer Prevention-Cancer Causes) (PDFDrive) PDFDocument338 pagesCancer Prevention - The Causes and Prevention of Cancer Volume 1 (Cancer Prevention-Cancer Causes) (PDFDrive) PDFtheresaNo ratings yet
- Carcinoid Syndrome, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandCarcinoid Syndrome, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- Career Appraisal GuidanceDocument31 pagesCareer Appraisal Guidancerummaan17No ratings yet
- Flows and Loads 43 PDFDocument6 pagesFlows and Loads 43 PDFrummaan17No ratings yet
- Request For Quotation Supply of Consultant ServicesDocument13 pagesRequest For Quotation Supply of Consultant Servicesrummaan17No ratings yet
- 3.3 Pressures On The Structural SurfacesDocument3 pages3.3 Pressures On The Structural Surfacesrummaan17No ratings yet
- Pre-Departure Medical ExaminationDocument7 pagesPre-Departure Medical Examinationrummaan17No ratings yet
- Pre-Departure Medical ExaminationDocument7 pagesPre-Departure Medical Examinationrummaan17No ratings yet
- Fire Water Tank Foundation DesignDocument14 pagesFire Water Tank Foundation Designrummaan17No ratings yet
- Report - 1 PDFDocument1 pageReport - 1 PDFrummaan17No ratings yet
- Design NoteDocument1 pageDesign Noterummaan17No ratings yet
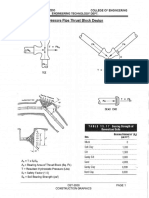
- Thrustblocks PDFDocument1 pageThrustblocks PDFrummaan17No ratings yet
- Software Verification: EXAMPLE 6-004Document7 pagesSoftware Verification: EXAMPLE 6-004rummaan17No ratings yet
- ThymomasDocument6 pagesThymomasAsmara SyedNo ratings yet
- Floppy InfantDocument48 pagesFloppy InfantAlexNo ratings yet
- Choriocarcinoma 11Document23 pagesChoriocarcinoma 11Fakhir HasanNo ratings yet
- Physical Examination and Health Assessment: Genitourinary SystemDocument134 pagesPhysical Examination and Health Assessment: Genitourinary Systemmesfin DemiseNo ratings yet
- Naprod Kaleidoscope Issue 2 - Naprod Life SciencesDocument5 pagesNaprod Kaleidoscope Issue 2 - Naprod Life SciencesNaprod Life Sciences Pvt. Ltd.No ratings yet
- Complication of POPDocument23 pagesComplication of POPKasey Chase0% (1)
- PNPK PNPKDocument3 pagesPNPK PNPKPutri JunitasariNo ratings yet
- Formulir Pencatatan Penandaan Lokasi Operasi Ruang/Unit/Bagian: Ruang Operasi Bulan: JUNI 2019 No Tanggal RM Diagnosa UtamaDocument6 pagesFormulir Pencatatan Penandaan Lokasi Operasi Ruang/Unit/Bagian: Ruang Operasi Bulan: JUNI 2019 No Tanggal RM Diagnosa UtamaMenikNo ratings yet
- Management of Discoloured TeethDocument77 pagesManagement of Discoloured TeethmirfanulhaqNo ratings yet
- CCDocument2 pagesCCretnopuspaningtyasNo ratings yet
- (NATO ASI Series 250) L. Ehrenberg (Auth.), Curtis C. Travis (Eds.) - Use of Biomarkers in Assessing Health and Environmental Impacts of Chemical Pollutants-Springer US (1993)Document283 pages(NATO ASI Series 250) L. Ehrenberg (Auth.), Curtis C. Travis (Eds.) - Use of Biomarkers in Assessing Health and Environmental Impacts of Chemical Pollutants-Springer US (1993)Sri Gama AprianiNo ratings yet
- Drug StudyDocument5 pagesDrug StudyJanine Erika Julom BrillantesNo ratings yet
- Imaging Breast Ca Nipple DischargeDocument1 pageImaging Breast Ca Nipple DischargesjulurisNo ratings yet
- Authors: Ibel Carri, María Marcela Barrio, Morten Nielsen: BackgroundDocument1 pageAuthors: Ibel Carri, María Marcela Barrio, Morten Nielsen: BackgroundrexNo ratings yet
- A Randomized Controlled Trial of Medication and Cognitive-Behavioral Therapy For HypochondriasisDocument9 pagesA Randomized Controlled Trial of Medication and Cognitive-Behavioral Therapy For HypochondriasisDewina Dyani Rosari IINo ratings yet
- Tuberculin Skin Test: Facilitator GuideDocument31 pagesTuberculin Skin Test: Facilitator GuideTiwi NaloleNo ratings yet
- Benign Breast DisordersDocument16 pagesBenign Breast DisordersJuan Carlos AuquiNo ratings yet
- A Productive and Friendly Epididymitis TreatmentDocument10 pagesA Productive and Friendly Epididymitis TreatmentwozhiainiNo ratings yet
- (Methods in Molecular Biology 1508) Thomas Lion (Eds.) - Human Fungal Pathogen Identification - Methods and Protocols (2017, Humana Press)Document439 pages(Methods in Molecular Biology 1508) Thomas Lion (Eds.) - Human Fungal Pathogen Identification - Methods and Protocols (2017, Humana Press)asfwegereNo ratings yet
- Teaching ProfessioDocument9 pagesTeaching ProfessioKharen EbasNo ratings yet
- 16 Tips On How To Treat HPV Naturally and Effectively at HomeDocument12 pages16 Tips On How To Treat HPV Naturally and Effectively at HomePaul LauNo ratings yet
- Test TakingDocument179 pagesTest TakingYucef Bahian-AbangNo ratings yet
- Getting Started With Homeopathy - Find A RemedyDocument52 pagesGetting Started With Homeopathy - Find A Remedymadhavkrishna garg100% (1)
- Kerosene - K1 & K2Document7 pagesKerosene - K1 & K2JodyNo ratings yet
- Veterans Hearing Loss Physician EvaluationDocument5 pagesVeterans Hearing Loss Physician Evaluationjim912No ratings yet
- Cissus Quadrangularis Plant Extract Enhances The Development of Cortical Bone and Trabeculae in The Fetal FemurDocument21 pagesCissus Quadrangularis Plant Extract Enhances The Development of Cortical Bone and Trabeculae in The Fetal FemurdellaNo ratings yet