Download as pptx, pdf, or txt
You might also like
- Weightlifting USAW Level 1 Sports PerformanceDocument50 pagesWeightlifting USAW Level 1 Sports PerformanceChris Kasinski100% (2)
- Anatomy NotesDocument3 pagesAnatomy NotesKaren Kaye Canlas100% (3)
- Rehabilitation Protocol For Clavicle OrifDocument3 pagesRehabilitation Protocol For Clavicle OrifJaneNo ratings yet
- Sport Traumatology-III Knee Complex-10Document26 pagesSport Traumatology-III Knee Complex-10kamran aliNo ratings yet
- ACL Reconstruction 2020Document39 pagesACL Reconstruction 2020محمد عقلNo ratings yet
- The Shoulder: Understanding The Science Behind Both Movement and Dysfunction by Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, AMSDocument9 pagesThe Shoulder: Understanding The Science Behind Both Movement and Dysfunction by Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, AMSChrisGellertNo ratings yet
- Trunk Stability by Calvin Morriss, PHD.: What Exactly Is Trunk Stability For A Rugby Player?Document9 pagesTrunk Stability by Calvin Morriss, PHD.: What Exactly Is Trunk Stability For A Rugby Player?Justice Man100% (1)
- Shoulder Injuries ReportDocument9 pagesShoulder Injuries Reportley343100% (1)
- Scapular Stabilization ExercisesDocument2 pagesScapular Stabilization ExercisesnimitrisNo ratings yet
- Acute Anterior Shoulder Dislocation Physical Therapy ProtocolDocument4 pagesAcute Anterior Shoulder Dislocation Physical Therapy Protocolgermano87No ratings yet
- Final Phase Exercise RehabilitationDocument11 pagesFinal Phase Exercise RehabilitationLeighton SmithNo ratings yet
- Spi Gelman LDocument3 pagesSpi Gelman LkotraeNo ratings yet
- Normal Mechanics and Pathophysiology of The ShoulderDocument48 pagesNormal Mechanics and Pathophysiology of The ShoulderAdelin IlincaNo ratings yet
- Rotator Cuff InjuriesDocument26 pagesRotator Cuff Injuriesanname_girlNo ratings yet
- Overuse Injuries of UpperDocument55 pagesOveruse Injuries of UpperNicu Tanase-RaduNo ratings yet
- Rotator Cuff InjuryDocument29 pagesRotator Cuff InjuryArko duttaNo ratings yet
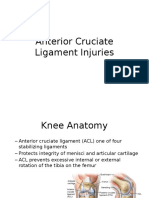
- Anterior Cruciate Ligament InjuriesDocument16 pagesAnterior Cruciate Ligament InjuriesAlmas PrawotoNo ratings yet
- Acl PCL PresentationDocument17 pagesAcl PCL PresentationSafwan Idham RamlanNo ratings yet
- ACL InjuryDocument42 pagesACL InjuryRishabh VermaNo ratings yet
- High - and Low-Bar Squatting Techniques During Weight-Training.1996Document14 pagesHigh - and Low-Bar Squatting Techniques During Weight-Training.1996Broc Il SerbatoioNo ratings yet
- 15hip TotalHipArthroplastyDocument4 pages15hip TotalHipArthroplastyudaysravsNo ratings yet
- Patellar Tendon Rupture and RehabilitationDocument4 pagesPatellar Tendon Rupture and RehabilitationdedsnetNo ratings yet
- Olympic WeightliftingDocument51 pagesOlympic WeightliftingdawidNo ratings yet
- The Countermovement ShrugDocument4 pagesThe Countermovement ShrugAnonymous OikQYkNo ratings yet
- Analysis of SwimmingDocument11 pagesAnalysis of SwimmingawilliamsNo ratings yet
- Chapter 11 - Injuries - The Hip, Thigh, and PelvisDocument13 pagesChapter 11 - Injuries - The Hip, Thigh, and PelvisSurgicalgownNo ratings yet
- Physiotherapy in AmputationsDocument6 pagesPhysiotherapy in Amputationskrissh20No ratings yet
- Hip Journal SquattingDocument33 pagesHip Journal SquattingVicky KdNo ratings yet
- Pathomechanics of Acromioclavicular JointDocument28 pagesPathomechanics of Acromioclavicular JointMuhib ArfinNo ratings yet
- Rotator Cuff Repair Rehab ProtocolDocument6 pagesRotator Cuff Repair Rehab Protocolalz388508No ratings yet
- Hamstring Exercise ProgressionDocument15 pagesHamstring Exercise ProgressionFrancisco De VelascoNo ratings yet
- 2013 Glenohumeral Motion Deficits, Friend or FoeDocument17 pages2013 Glenohumeral Motion Deficits, Friend or FoeIsrael Matías Chandia RamírezNo ratings yet
- HIP JOINT Special Tests-WPS OfficeDocument51 pagesHIP JOINT Special Tests-WPS OfficeManisha Mishra100% (2)
- The Shoulder and Shoulder GirdleDocument43 pagesThe Shoulder and Shoulder GirdleMuhammad UsmanNo ratings yet
- Rehabilitation After Anterior Cruciate Ligament ReconstructionDocument62 pagesRehabilitation After Anterior Cruciate Ligament ReconstructionVladGrosuNo ratings yet
- LL AmputationDocument119 pagesLL AmputationMpt SportsNo ratings yet
- Structural Balance of ShouldersDocument51 pagesStructural Balance of ShouldersMark McKean100% (1)
- Sports Injuries in UE - Shoulder - Part 3.Document87 pagesSports Injuries in UE - Shoulder - Part 3.salmankhan09215No ratings yet
- Lui KinesDocument29 pagesLui KinesJewel May LuiNo ratings yet
- Hip DislocDocument67 pagesHip DislocAli TawbeNo ratings yet
- Closed Reduction of Posterior Hip DislocationDocument4 pagesClosed Reduction of Posterior Hip DislocationHannah JuanitaNo ratings yet
- Jarrett 2013Document20 pagesJarrett 2013aliNo ratings yet
- Scoliosis 2003Document53 pagesScoliosis 2003Rei Perdio100% (2)
- Knee Injuries Part 1Document38 pagesKnee Injuries Part 1meenoNo ratings yet
- Shoulder Pain OverviewDocument37 pagesShoulder Pain Overvieweddie bechillNo ratings yet
- Anterior Cruciate LigamentDocument26 pagesAnterior Cruciate LigamentAmandeep Singh100% (2)
- نسخة light blue creative modern medical clinic presentationDocument33 pagesنسخة light blue creative modern medical clinic presentationFaresNo ratings yet
- Hip Labral Repair PresentationDocument15 pagesHip Labral Repair Presentationapi-612728940No ratings yet
- Swimming Warm Up StretchesDocument9 pagesSwimming Warm Up StretchesMark CastreyNo ratings yet
- 8 - 13 March, 2010Document72 pages8 - 13 March, 2010sandipandassarmaNo ratings yet
- 3 Weightlifting Ireland Why We Use Olympic Lifts LiftDocument40 pages3 Weightlifting Ireland Why We Use Olympic Lifts LiftMark O ConnellNo ratings yet
- BloopDocument20 pagesBloopsundar persaudNo ratings yet
- Bicipital TendinitisDocument19 pagesBicipital TendinitisRonak PatelNo ratings yet
- Traction: Cervical & LumbarDocument21 pagesTraction: Cervical & LumbarSEGERD01No ratings yet
- Traction: Cervical & LumbarDocument21 pagesTraction: Cervical & LumbarBoud ElhassanNo ratings yet
- C. Resistance Training Exercise TechniqueDocument24 pagesC. Resistance Training Exercise TechniqueNicole Ba�aresNo ratings yet
- A Teaching Progression For Squatting Exercises.7Document9 pagesA Teaching Progression For Squatting Exercises.7Rhiannon CristinaNo ratings yet
- Summary of Dr. Aaron Horschig, Dr. Kevin Sonthana & Travis Neff's The Squat BibleFrom EverandSummary of Dr. Aaron Horschig, Dr. Kevin Sonthana & Travis Neff's The Squat BibleNo ratings yet
- Laboratory 1. Anatomical Position and TerminologiesDocument2 pagesLaboratory 1. Anatomical Position and TerminologiesAANo ratings yet
- Class 5 Science Classwork 091020Document3 pagesClass 5 Science Classwork 091020Rakesh AgarwalNo ratings yet
- Postmedj00400 0048Document3 pagesPostmedj00400 0048TRIANDINI TRIANDININo ratings yet
- Nerve InjuriesDocument3 pagesNerve InjuriesAmber MerrittNo ratings yet
- To Anatomical Studypterigomaxillary 2010 ComDocument22 pagesTo Anatomical Studypterigomaxillary 2010 ComTejas KhaireNo ratings yet
- The Hip: Therapeutic Exercise 2 Lino Linford BangayanDocument91 pagesThe Hip: Therapeutic Exercise 2 Lino Linford BangayanLino Linford Yu Bangayan100% (1)
- Midterm Exam Hc1 Skills SETADocument7 pagesMidterm Exam Hc1 Skills SETAKathrina AlfonsoNo ratings yet
- Facial ReconstructionDocument39 pagesFacial Reconstructionapi-3704106100% (4)
- Sialography ExaminationDocument14 pagesSialography ExaminationEkaRahmaNo ratings yet
- Higher Mental Functions OldDocument36 pagesHigher Mental Functions OldPriya Kuberan100% (1)
- (10920684 - Neurosurgical Focus) Tuberculum Sellae MeningiomasDocument6 pages(10920684 - Neurosurgical Focus) Tuberculum Sellae MeningiomasputriNo ratings yet
- Introduction To The Cardiovascular SystemDocument22 pagesIntroduction To The Cardiovascular Systemwaqas_xsNo ratings yet
- Robin Gallant39s Intensive Max Glute Hypertrophy PDocument8 pagesRobin Gallant39s Intensive Max Glute Hypertrophy PSavitaNo ratings yet
- Update On Upper BlepharoplastyDocument20 pagesUpdate On Upper BlepharoplastyRajinder Kumar BassanNo ratings yet
- Kriya For Conquering SleepDocument4 pagesKriya For Conquering SleepKirpal JotyNo ratings yet
- The Workings of The Brain Powers of The MindDocument17 pagesThe Workings of The Brain Powers of The MindLovely ramirezNo ratings yet
- Oral Radio Lec 4 FinalDocument11 pagesOral Radio Lec 4 FinalPrince AhmedNo ratings yet
- Make A Model of The Human Body: Science ProjectDocument5 pagesMake A Model of The Human Body: Science ProjectEris Putra SulaemanNo ratings yet
- The Language of AnatomyDocument7 pagesThe Language of AnatomyLinziJaeOnelNo ratings yet
- Cranial Nerve Part 2 (V, VII) : By: Fajri Mohammed (MD)Document51 pagesCranial Nerve Part 2 (V, VII) : By: Fajri Mohammed (MD)abo kooNo ratings yet
- Quarter 3: WORKSHEET NO. 1 Name: Score: Section: Date Submitted The Endocrine SystemDocument4 pagesQuarter 3: WORKSHEET NO. 1 Name: Score: Section: Date Submitted The Endocrine SystemPrincess RamoleteNo ratings yet
- Rehab BLDocument3 pagesRehab BLarissa razaliNo ratings yet
- Complete Kicking The Ultimate Guide To Kicks For Martial Arts Self-Defense & Combat SportsDocument140 pagesComplete Kicking The Ultimate Guide To Kicks For Martial Arts Self-Defense & Combat SportsXenthoyo Kenth Lee100% (8)
- Cuprins Atlas YokochiDocument2 pagesCuprins Atlas Yokochicherylin1No ratings yet
- Alingment in TKRDocument3 pagesAlingment in TKRdeepak100% (1)
- Anatomy of External EarDocument49 pagesAnatomy of External EarInderdeep AroraNo ratings yet
- Kemu A & P 1Document4 pagesKemu A & P 1malenya1No ratings yet
- Year Round Periodization For High School Football PDFDocument6 pagesYear Round Periodization For High School Football PDFmunichrangersNo ratings yet
- ATLS Head TraumaDocument30 pagesATLS Head TraumadilaNo ratings yet