Download as ppt, pdf, or txt
You might also like
- (The European Society of Cardiology Series) Marco Tubaro (Editor), Pascal Vranckx (Editor), Susanna Price (Editor), Christiaan Vrints (Editor), Eric Bonnefoy (Editor) - The ESC Textbook of Intensive ADocument1,088 pages(The European Society of Cardiology Series) Marco Tubaro (Editor), Pascal Vranckx (Editor), Susanna Price (Editor), Christiaan Vrints (Editor), Eric Bonnefoy (Editor) - The ESC Textbook of Intensive AEdu Martins100% (1)
- Carol Rivers'board Review FlashcardsDocument440 pagesCarol Rivers'board Review FlashcardsJennelle CadoganNo ratings yet
- Electro Cardiogram & DysrythmiasDocument40 pagesElectro Cardiogram & DysrythmiasshobharamkrishnaNo ratings yet
- Physiology Behind Contraceptive MethodsDocument26 pagesPhysiology Behind Contraceptive Methodsnirilib100% (2)
- Conduction System of The HeartDocument24 pagesConduction System of The HeartnirilibNo ratings yet
- Conduction System of The HeartDocument24 pagesConduction System of The HeartnirilibNo ratings yet
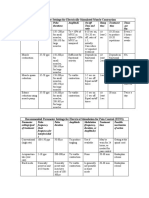
- Parameter Settings For Electrically Stimulated Muscle ContractionDocument3 pagesParameter Settings For Electrically Stimulated Muscle Contractionpallen100% (5)
- ECG ECG Basics Presentation 201309101527422446 PDFDocument45 pagesECG ECG Basics Presentation 201309101527422446 PDFRamesh RajNo ratings yet
- ECG AbnormalDocument60 pagesECG Abnormalvidishmalaviya300No ratings yet
- 35ekg 1Document103 pages35ekg 1Veerapong Vattanavanit100% (2)
- Cardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyDocument87 pagesCardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyummimalikihamidNo ratings yet
- Conduction System of Heart-FinalDocument69 pagesConduction System of Heart-FinalAshish ChavanNo ratings yet
- Nursing School EKGDocument43 pagesNursing School EKGRob Dickerson100% (1)
- Kuliah EKG Blok Kegawatdaruratan September 2018Document122 pagesKuliah EKG Blok Kegawatdaruratan September 2018khanzaisdiharanaNo ratings yet
- Electrocardiogram: By: Keverne Jhay P. Colas, RN, MANDocument72 pagesElectrocardiogram: By: Keverne Jhay P. Colas, RN, MANGaras AnnaBerniceNo ratings yet
- Arrhythmia NewDocument73 pagesArrhythmia Newlohith saiNo ratings yet
- Normal ECGDocument63 pagesNormal ECGMohd Johari Mohd ShafuwanNo ratings yet
- Arrhythmias: Sing Khien Tiong Gpst1Document34 pagesArrhythmias: Sing Khien Tiong Gpst1preethi preethaNo ratings yet
- Cardiovascular AlterationsDocument46 pagesCardiovascular Alterationsaneesnair86No ratings yet
- 321 Lecture ECGDocument38 pages321 Lecture ECGCea Mikee Mitch BartolomeNo ratings yet
- N12 Cardiac DysrhythmiasDocument68 pagesN12 Cardiac Dysrhythmiaskathbondoc03No ratings yet
- Arrhythmias 101Document59 pagesArrhythmias 101Abdiwahab ShahnizzleNo ratings yet
- Advanced ECG AnalysisDocument90 pagesAdvanced ECG AnalysisnursewinstonNo ratings yet
- Chapter - 036 Arrhythmias ClassDocument129 pagesChapter - 036 Arrhythmias ClassWisdomIsMiseryNo ratings yet
- ECG InterpretationDocument73 pagesECG Interpretationsultan khabeebNo ratings yet
- ECG Red BookDocument54 pagesECG Red BookHilbertHeungNo ratings yet
- Ecg Pathology 02Document95 pagesEcg Pathology 02Andi MP Manurung100% (1)
- Cardiac Arrest: April B. Perez, RN, Man, PHD, FpchaDocument50 pagesCardiac Arrest: April B. Perez, RN, Man, PHD, Fpchayuuki konnoNo ratings yet
- Basics of EKG Interpretation: Michael Rochon-Duck July 6, 2015 Slideset Adapted From: Jennifer Ballard-Hernandez, DNPDocument127 pagesBasics of EKG Interpretation: Michael Rochon-Duck July 6, 2015 Slideset Adapted From: Jennifer Ballard-Hernandez, DNPYS NateNo ratings yet
- Brady ArrhythmiasDocument36 pagesBrady ArrhythmiasSajin AlexanderNo ratings yet
- 2 ECG HockstadDocument65 pages2 ECG HockstadAUH ICUNo ratings yet
- Electrocardiography (Ecg) : Presented By: Fahad I. HussienDocument102 pagesElectrocardiography (Ecg) : Presented By: Fahad I. HussienMustafa A. DawoodNo ratings yet
- Ecg 21Document30 pagesEcg 21Afzal HussainNo ratings yet
- Jose Gianni C. Espada Clinical ClerkDocument133 pagesJose Gianni C. Espada Clinical ClerkJohn Christopher LucesNo ratings yet
- Arrhythmias: Terminology, Definitions, and MechanismsDocument16 pagesArrhythmias: Terminology, Definitions, and MechanismshazelelNo ratings yet
- ECG ArrythemiaDocument79 pagesECG ArrythemiaMahadevNo ratings yet
- Cardiovascular System Study SheetDocument8 pagesCardiovascular System Study SheetTkNo ratings yet
- Ecg Interpretation New TemplateDocument88 pagesEcg Interpretation New TemplateJonathan NgNo ratings yet
- ArrhthmiasDocument44 pagesArrhthmiasmadeha goharNo ratings yet
- 3rd Lecture On Arrythmias by Dr. RoomiDocument16 pages3rd Lecture On Arrythmias by Dr. RoomiMudassar Roomi100% (2)
- ArythmiaDocument23 pagesArythmiafrisianamirashiNo ratings yet
- Arrythemia 1Document73 pagesArrythemia 1Mooma fatimaNo ratings yet
- EkgDocument94 pagesEkgCaprita LauraNo ratings yet
- Basic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalDocument79 pagesBasic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalVeerapong Vattanavanit0% (1)
- D_4_heart__2_Document22 pagesD_4_heart__2_Jyoti singhNo ratings yet
- ECG - Doc 09Document11 pagesECG - Doc 09Rincy RajanNo ratings yet
- Arrhythmias GeneralDocument131 pagesArrhythmias GeneralAnonymous IRl5fn6No ratings yet
- EKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDocument58 pagesEKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesrsadellaNo ratings yet
- Ecg BSTDocument204 pagesEcg BSTAnusha Verghese100% (1)
- Care of Patients With DysrhythmiasDocument37 pagesCare of Patients With Dysrhythmiasأم حمدNo ratings yet
- Cardiac Arrhythmia 171209212142 2Document74 pagesCardiac Arrhythmia 171209212142 2Gunel Sadiqova100% (1)
- Heartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaDocument31 pagesHeartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaNinaNo ratings yet
- Electrocardiogram: Hanan Fathy 2008Document94 pagesElectrocardiogram: Hanan Fathy 2008LiliLiliNo ratings yet
- Cardio AssessmentDocument104 pagesCardio Assessmentlowell.cerezo.ihsNo ratings yet
- Basics and Interpretation: Sif HansdottirDocument65 pagesBasics and Interpretation: Sif Hansdottirwenny1186100% (1)
- An Introduction To The 12 Lead EcgDocument85 pagesAn Introduction To The 12 Lead EcgAris Diyan YulistiawanNo ratings yet
- Cardiovascular Physiology 2Document52 pagesCardiovascular Physiology 2maxmus4No ratings yet
- ARITMIADocument47 pagesARITMIASarah JR Nur AzizahNo ratings yet
- Cardiac ArrhythmiasDocument11 pagesCardiac ArrhythmiasChino Paolo SamsonNo ratings yet
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocument74 pagesBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- ECG1Document67 pagesECG1Farhan RosliNo ratings yet
- ArrhythmiasDocument53 pagesArrhythmiasabotreka056No ratings yet
- Arrhythmia: Dian Pratiwi Cardiology Department Chasan Boesoerie HospitalDocument73 pagesArrhythmia: Dian Pratiwi Cardiology Department Chasan Boesoerie HospitalummuabNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Physiology of Reproductive SystemDocument180 pagesPhysiology of Reproductive Systemnirilib0% (1)
- Renal PhysiologyDocument124 pagesRenal Physiologynirilib100% (2)
- Calcium and Phosphate HomeosatsisDocument35 pagesCalcium and Phosphate HomeosatsisnirilibNo ratings yet
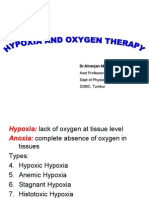
- Dr. Niranjan Murthy H L Associate Professor Dept of Physiology SSMC, TumkurDocument18 pagesDr. Niranjan Murthy H L Associate Professor Dept of Physiology SSMC, TumkurnirilibNo ratings yet
- Urine Concentration and Diluting MechanismsDocument26 pagesUrine Concentration and Diluting MechanismsnirilibNo ratings yet
- Descending Tracts: Dr. Niranjan Murthy H L Asst Prof of Physiology SSMC, TumkurDocument23 pagesDescending Tracts: Dr. Niranjan Murthy H L Asst Prof of Physiology SSMC, Tumkurnirilib100% (1)
- PlateletsDocument23 pagesPlateletsnirilibNo ratings yet
- Regulation of ElectrolytesDocument28 pagesRegulation of ElectrolytesnirilibNo ratings yet
- Physiology of MicturitionDocument9 pagesPhysiology of MicturitionnirilibNo ratings yet
- Circulatory Shock: Dr. Niranjan Murthy H L Asst Prof of Physiology SSMC, TumkurDocument18 pagesCirculatory Shock: Dr. Niranjan Murthy H L Asst Prof of Physiology SSMC, TumkurnirilibNo ratings yet
- Physiology Color VisionDocument18 pagesPhysiology Color VisionnirilibNo ratings yet
- CerebrumDocument45 pagesCerebrumnirilib0% (1)
- Nerve PhysiologyDocument31 pagesNerve Physiologynirilib100% (4)
- ERYTHROPOEISISDocument28 pagesERYTHROPOEISISnirilibNo ratings yet
- Plasma ProteinsDocument11 pagesPlasma ProteinsnirilibNo ratings yet
- Dr. Niranjan Murthy H L Asst. Prof. of Physiology SSMC, TumkurDocument39 pagesDr. Niranjan Murthy H L Asst. Prof. of Physiology SSMC, Tumkurnirilib100% (1)
- Respiratory Insufficiency & Other Clinical ConditionsDocument16 pagesRespiratory Insufficiency & Other Clinical ConditionsnirilibNo ratings yet
- Pulmonary Function TestsDocument35 pagesPulmonary Function Testsnirilib100% (4)
- Effect of Yoga and Supervised Integrated Exercise On Heart Rate Variability and Blood Pressure in HypertensivesDocument5 pagesEffect of Yoga and Supervised Integrated Exercise On Heart Rate Variability and Blood Pressure in HypertensivesnirilibNo ratings yet
- Hypoxia and Oxygen TherapyDocument19 pagesHypoxia and Oxygen Therapynirilib86% (7)
- Regulation of RespirationDocument46 pagesRegulation of Respirationnirilib89% (9)
- Respiration in Unusual EnvironmentsDocument26 pagesRespiration in Unusual Environmentsnirilib100% (1)
- Structure of Skeletal MuscleDocument13 pagesStructure of Skeletal MusclenirilibNo ratings yet
- Properties of Cardiac Muscle and Conducting SystemsDocument38 pagesProperties of Cardiac Muscle and Conducting Systemsnirilib100% (4)
- Properties of Skeletal MuscleDocument21 pagesProperties of Skeletal Musclenirilib72% (18)
- Dr. Niranjan Murthy H L: Asst. Prof., Dept. of Physiology Sree Siddhartha Medical College & Hospital, TumkurDocument17 pagesDr. Niranjan Murthy H L: Asst. Prof., Dept. of Physiology Sree Siddhartha Medical College & Hospital, Tumkurnirilib100% (1)
- Neuromuscular Junction: Dr. Niranjan Murthy H LDocument18 pagesNeuromuscular Junction: Dr. Niranjan Murthy H Lnirilib100% (3)
- Mobile Coronary Care UnitDocument16 pagesMobile Coronary Care UnitArcha100% (2)
- دليل الأمراض الشائعة للأطباء-1Document148 pagesدليل الأمراض الشائعة للأطباء-1Ibrahim RamizNo ratings yet
- Use of Vasopressors and InotropesDocument16 pagesUse of Vasopressors and InotropesIrving H Torres LopezNo ratings yet
- Group 8 Oxygenation AtionDocument46 pagesGroup 8 Oxygenation AtionPrince Masroor Ali AbroNo ratings yet
- Cardiovascular Pharmacology: DR Muhamad Ali Sheikh Abdul Kader MD (Usm) MRCP (Uk) Cardiologist, Penang HospitalDocument63 pagesCardiovascular Pharmacology: DR Muhamad Ali Sheikh Abdul Kader MD (Usm) MRCP (Uk) Cardiologist, Penang HospitalCvt RasulNo ratings yet
- Identifying Newborns With Critical Congenital Heart DiseaseDocument32 pagesIdentifying Newborns With Critical Congenital Heart DiseaseHardian RakhmawardanaNo ratings yet
- Long Covid 1Document5 pagesLong Covid 1lakshminivas PingaliNo ratings yet
- AnaPhy Muscle Disorder Case Study-BASCODocument5 pagesAnaPhy Muscle Disorder Case Study-BASCOChristine Jane BascoNo ratings yet
- Long-Term Spaceflight and The Cardiovascular SystemDocument8 pagesLong-Term Spaceflight and The Cardiovascular SystemSantoso 9JimmyNo ratings yet
- Ebstein Anomaly in The Adult PatientDocument11 pagesEbstein Anomaly in The Adult PatientRJMNo ratings yet
- Quiz 8 To 46Document7 pagesQuiz 8 To 46JhayneNo ratings yet
- Capstone PPDocument20 pagesCapstone PPapi-569838480No ratings yet
- Ecgs Made Easy 5th Edition Aehlert Test BankDocument15 pagesEcgs Made Easy 5th Edition Aehlert Test Bankemmaevanswqstmbjgxe100% (14)
- Short Learning Topics On Biomedical Equipments by Heer Thoshani 22998Document55 pagesShort Learning Topics On Biomedical Equipments by Heer Thoshani 22998Salim AloneNo ratings yet
- In Premature Ventricular Complex, An Impulse That Starts in A Ventricle and Is Conducted Through The Ventricles Before The Next Normal SinusDocument7 pagesIn Premature Ventricular Complex, An Impulse That Starts in A Ventricle and Is Conducted Through The Ventricles Before The Next Normal SinushelloaNo ratings yet
- Intuitive Patient Monitor For Comprehensive Bedside Care: iMEC15Document4 pagesIntuitive Patient Monitor For Comprehensive Bedside Care: iMEC15Camilo OrtegaNo ratings yet
- Bradycardia and TachycardiaDocument50 pagesBradycardia and Tachycardialiu_owen17No ratings yet
- 18 CPRIJBH2019DecDocument25 pages18 CPRIJBH2019DecLelyNo ratings yet
- Basics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyDocument206 pagesBasics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyRavi SharmaNo ratings yet
- COVID-19 - Vaccine - AstraZeneca - UK - Vaccine Analysis Print 24 Nov 2022Document132 pagesCOVID-19 - Vaccine - AstraZeneca - UK - Vaccine Analysis Print 24 Nov 2022Mary-Jane StevensNo ratings yet
- Cardiovascular Drug GuidelinesDocument182 pagesCardiovascular Drug GuidelinesSonishNo ratings yet
- ECG PPT CH 06 v3Document42 pagesECG PPT CH 06 v3cdiledu.itNo ratings yet
- Normal Ecg, Infarction & Arrhythmia SDocument98 pagesNormal Ecg, Infarction & Arrhythmia SAdinda GupitaNo ratings yet
- The Heart: Gen PhysioDocument73 pagesThe Heart: Gen PhysioDawnie AlvarezNo ratings yet
- SS DM MCH 2020 - 2021 Schedule Nov 6th Update PDFDocument32 pagesSS DM MCH 2020 - 2021 Schedule Nov 6th Update PDFlakshminivas PingaliNo ratings yet
- Elizabeth C. Sutliff: Y S U, Y, O K S U, K, ODocument3 pagesElizabeth C. Sutliff: Y S U, Y, O K S U, K, Oapi-564432337No ratings yet
- Physiology-Summary NotesDocument201 pagesPhysiology-Summary NotesReem NasserNo ratings yet