
Pharmacogenetics 2008 For Med Students
Pharmacogenetics 2008 For Med Students
You might also like
- CR Certificate (1465731)Document6 pagesCR Certificate (1465731)rampartnersbusinessllcNo ratings yet
- Czarina Drug Study JuneDocument20 pagesCzarina Drug Study JuneNicoh AvilaNo ratings yet
- Their Eyes Were Watching GodDocument13 pagesTheir Eyes Were Watching Godapi-316773627100% (1)
- PharmacogeneticsDocument30 pagesPharmacogeneticsShailendra Sk100% (3)
- 2principles of Geriatric Pharmacotherapy - Lee - 10-19-10Document53 pages2principles of Geriatric Pharmacotherapy - Lee - 10-19-10Mbel'z Mbel'z Embil'zNo ratings yet
- Adverse Drug ReactionDocument108 pagesAdverse Drug ReactionBinod Sah100% (2)
- 5685 - UHN2012Pharmacogenomic PharmacogeneticDocument44 pages5685 - UHN2012Pharmacogenomic PharmacogeneticAdinda TobingNo ratings yet
- Lecture INST-100046 2022 09 12 04 48 38Document31 pagesLecture INST-100046 2022 09 12 04 48 38Nithya mandalaNo ratings yet
- Dosage Form For Personalized Medicine: HistoryDocument11 pagesDosage Form For Personalized Medicine: HistoryNayeema KhowserNo ratings yet
- Pharmacogenomics 121004112431 Phpapp02Document53 pagesPharmacogenomics 121004112431 Phpapp0288AKK100% (1)
- Farm A Kogen EtikDocument60 pagesFarm A Kogen Etikrahmad wahyudiNo ratings yet
- MCM16-283 Drug Induced DiseasesDocument128 pagesMCM16-283 Drug Induced DiseasesAshraf Khan ShaonNo ratings yet
- Importance of Pharmacogenomics in The Personalized MedicineDocument6 pagesImportance of Pharmacogenomics in The Personalized MedicineJames AustinNo ratings yet
- ADRs - Classification, Mechanism, Predisposing Factors & Causality AssessmentDocument7 pagesADRs - Classification, Mechanism, Predisposing Factors & Causality AssessmentAman UpadhyayNo ratings yet
- Pharmaco GeneticsDocument52 pagesPharmaco GeneticsManikanta GupthaNo ratings yet
- Pharmacogenetics Drug Drug Interactions1Document16 pagesPharmacogenetics Drug Drug Interactions1Marfu'ah Mar'ahNo ratings yet
- Trastuzumab MonographDocument11 pagesTrastuzumab MonographAmeliaNo ratings yet
- Pharmacogenomics:: Increasing The Safety and Effectiveness of Drug TherapyDocument12 pagesPharmacogenomics:: Increasing The Safety and Effectiveness of Drug TherapyFlorentina GasttiNo ratings yet
- Genetics Related Adr With Example FocusingDocument10 pagesGenetics Related Adr With Example Focusingaadrika negiNo ratings yet
- PharmecogenomicsDocument21 pagesPharmecogenomicsRatan Ratan100% (1)
- Theselectionof Antiepilepticdrugs Forthetreatmentof Epilepsyinchildren AndadultsDocument10 pagesTheselectionof Antiepilepticdrugs Forthetreatmentof Epilepsyinchildren AndadultsFaizan MazharNo ratings yet
- Pharmacogenomics: New Challenges For Thai Anesthesiologists: J Med Assoc Thai 2017 100 (Suppl. 7) : S250-S258Document9 pagesPharmacogenomics: New Challenges For Thai Anesthesiologists: J Med Assoc Thai 2017 100 (Suppl. 7) : S250-S258Ronald André Buleje HinostrozaNo ratings yet
- Clin Pharmacy ADRDocument36 pagesClin Pharmacy ADRAnonymous DgPsK0oQNo ratings yet
- Clin Pharmacy ADRDocument24 pagesClin Pharmacy ADRAnonymous DgPsK0oQNo ratings yet
- Critical Limits of Laboratory Results For Urgent Clinician NotificationDocument8 pagesCritical Limits of Laboratory Results For Urgent Clinician NotificationCarl DonaireNo ratings yet
- JIFCC Lab Tests Interpretation 2018Document8 pagesJIFCC Lab Tests Interpretation 2018Abdul Sattar100% (1)
- Farmakogenetik EditDocument60 pagesFarmakogenetik Editfitriadevie451No ratings yet
- Geriatric Pharmacology: Lisa Rosenberg, MD Touro University Nevada April 6, 2011Document45 pagesGeriatric Pharmacology: Lisa Rosenberg, MD Touro University Nevada April 6, 2011Recky Patala100% (1)
- ADRsDocument56 pagesADRsFarina FaraziNo ratings yet
- Drug Interaction-SibyDocument93 pagesDrug Interaction-SibyAswin DamodaranNo ratings yet
- Monitoring Efek Samping Obat 12Document36 pagesMonitoring Efek Samping Obat 12Novitra Dewi100% (1)
- Referensi Nilai KritisDocument9 pagesReferensi Nilai KritisFaiz AchmadNo ratings yet
- Daunorubicin: Drug NameDocument7 pagesDaunorubicin: Drug NameEdgar Ledesma-MartínezNo ratings yet
- Xarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Document26 pagesXarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Dimas RfNo ratings yet
- Anti-Cancer DrugsDocument78 pagesAnti-Cancer DrugsLaghari Jamil100% (1)
- Warfarin - Drug InformationDocument23 pagesWarfarin - Drug InformationTestesteNo ratings yet
- PHARMACOTHERAPY IN GERIATRIC PATIENTS - PPT RF11fcbc - TMP (Dr. Suharti S, SPFK)Document29 pagesPHARMACOTHERAPY IN GERIATRIC PATIENTS - PPT RF11fcbc - TMP (Dr. Suharti S, SPFK)Farid NurdiansyahNo ratings yet
- Introduction To PharmacogenomicsDocument35 pagesIntroduction To Pharmacogenomicssazaki224No ratings yet
- LP CardioDocument8 pagesLP CardioEliza ToteNo ratings yet
- Adverse Drug Reporting (Adrs)Document11 pagesAdverse Drug Reporting (Adrs)Razia JafferyNo ratings yet
- Pharmacogenetics 141110022651 Conversion Gate01Document45 pagesPharmacogenetics 141110022651 Conversion Gate01Jeevan Khanal0% (1)
- Use of Aeds in 2011 and Beyond: Optimizing Clinical ManagementDocument32 pagesUse of Aeds in 2011 and Beyond: Optimizing Clinical ManagementchandanNo ratings yet
- Geriatric Pharmacology DO 22Document41 pagesGeriatric Pharmacology DO 22enghannnNo ratings yet
- Oxford Handbook of Clinical PharmacyDocument10 pagesOxford Handbook of Clinical Pharmacygmsanto7No ratings yet
- Meso 2022Document82 pagesMeso 2022cindi diaNo ratings yet
- Dr. Jarir at Thobari, PHD - Basic Pharmacovigilance PDFDocument35 pagesDr. Jarir at Thobari, PHD - Basic Pharmacovigilance PDFFerina AngeliaNo ratings yet
- Adverse Drug ReactionsDocument14 pagesAdverse Drug Reactionsgaikwaduv98No ratings yet
- Ajovy - Fremanezumab - Drug Information - UpToDateDocument6 pagesAjovy - Fremanezumab - Drug Information - UpToDateDiana PhamNo ratings yet
- LectureDocument29 pagesLectureRiyazuddin MohammedNo ratings yet
- Aspectos Prácticos Nuevos Anticoagulantes Am Jour Hem 2011Document5 pagesAspectos Prácticos Nuevos Anticoagulantes Am Jour Hem 2011jose_esteban_pena_duranNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument32 pagesSee Full Prescribing Information For Complete Boxed WarningGag PafNo ratings yet
- Jamal 2014Document11 pagesJamal 2014Nguyễn Đức LongNo ratings yet
- PharmacogenomicsDocument56 pagesPharmacogenomicsapi-650133203No ratings yet
- MolnupiravirDocument7 pagesMolnupiravirConcepStore PyNo ratings yet
- 9 Personalized MedicineDocument34 pages9 Personalized Medicinehamza najmNo ratings yet
- FILE - 20220726 - 203059 - Gout LUONG MDDocument52 pagesFILE - 20220726 - 203059 - Gout LUONG MDQuang NguyenNo ratings yet
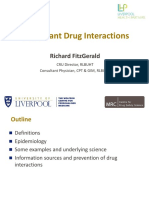
- 14.50 - Richard Fitzgerald - Important Drug InteractionsDocument30 pages14.50 - Richard Fitzgerald - Important Drug Interactionsasif charsiNo ratings yet
- Lecture 8 - PharmacogeneticsDocument38 pagesLecture 8 - PharmacogeneticsNicko WijayaNo ratings yet
- Adverse Effects of ArvsDocument10 pagesAdverse Effects of ArvsAllan Takudzwa MpeperekiNo ratings yet
- Albenza, (Albendazole) Dosing, Indications, Interactions, Adverse Effects, and MoreDocument4 pagesAlbenza, (Albendazole) Dosing, Indications, Interactions, Adverse Effects, and MoreSourav GhoshNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Herbal Supplements: Efficacy, Toxicity, Interactions with Western Drugs, and Effects on Clinical Laboratory TestsFrom EverandHerbal Supplements: Efficacy, Toxicity, Interactions with Western Drugs, and Effects on Clinical Laboratory TestsNo ratings yet
- Erf1899 and 1898 Isipingo HILLSDocument1 pageErf1899 and 1898 Isipingo HILLSTushar PareekNo ratings yet
- Biotechnology ReportDocument137 pagesBiotechnology ReportTushar PareekNo ratings yet
- Pharmacogenomics: The New Step Towards Improving HealthcareDocument14 pagesPharmacogenomics: The New Step Towards Improving HealthcareTushar PareekNo ratings yet
- GAP AnalysisDocument4 pagesGAP AnalysisTushar PareekNo ratings yet
- Emergency ProceduresDocument19 pagesEmergency ProceduresMilos Kalember100% (1)
- Isl and CapstoneDocument6 pagesIsl and Capstoneapi-348627392No ratings yet
- Technical Instruction ABB RED670Document10 pagesTechnical Instruction ABB RED670Iqball ArdiyanNo ratings yet
- How Long A Trip Is It From Here To Our Cairo Office?Document5 pagesHow Long A Trip Is It From Here To Our Cairo Office?Luyện TrầnNo ratings yet
- Social and Prof Issues Module2Document31 pagesSocial and Prof Issues Module2Angelo NebresNo ratings yet
- Introduction To LinguisticsDocument4 pagesIntroduction To LinguisticsRomnick Fernando CoboNo ratings yet
- Blood and Body Fluid SpillageDocument4 pagesBlood and Body Fluid SpillageSony AntonyNo ratings yet
- Truss - 2 Detail: Scale 1: 50 MTRSDocument1 pageTruss - 2 Detail: Scale 1: 50 MTRSGerald MasangayNo ratings yet
- FACTURADocument1 pageFACTURAAnny CañasNo ratings yet
- Safe ManualDocument2 pagesSafe Manualsrujan patelNo ratings yet
- Unit 1 - Foundations of BiochemistryDocument28 pagesUnit 1 - Foundations of BiochemistryJoselitz Reyes TumulakNo ratings yet
- Cost Volume Profit AnalysisDocument12 pagesCost Volume Profit Analysisganeshiyer1467% (3)
- Buckling and Ultimate Strength Assessment For Offshore Structures APRIL 2004Document5 pagesBuckling and Ultimate Strength Assessment For Offshore Structures APRIL 2004Flávio RodriguesNo ratings yet
- Music Link Investigation 1 & 2 Chhairatanak Huy PDFDocument27 pagesMusic Link Investigation 1 & 2 Chhairatanak Huy PDFChay HuyNo ratings yet
- Sheldon Krimsky - Kathleen Sloan - Race and The Genetic Revolution - Science, Myth, and Culture-Columbia University Press (2011)Document300 pagesSheldon Krimsky - Kathleen Sloan - Race and The Genetic Revolution - Science, Myth, and Culture-Columbia University Press (2011)Burnley JenifferNo ratings yet
- InvoiceDocument1 pageInvoiceAyam Goreng0% (1)
- Types of Strategies61Document69 pagesTypes of Strategies61TejashviNo ratings yet
- Conference Board of The Mathematical SciencesDocument43 pagesConference Board of The Mathematical Sciencesjhicks_mathNo ratings yet
- QA Lead Position Interview Questions and AnswersDocument10 pagesQA Lead Position Interview Questions and AnswersAkshay KhotNo ratings yet
- Read The Following Text About A Boy Called Cameron Oliver and His Award. Then, Answer The QuestionsDocument3 pagesRead The Following Text About A Boy Called Cameron Oliver and His Award. Then, Answer The QuestionsYênNo ratings yet
- A Review On The Law of Supply and Demand (Part 1)Document25 pagesA Review On The Law of Supply and Demand (Part 1)Janiña NatividadNo ratings yet
- Ust HtaDocument5 pagesUst HtaSteven SantosNo ratings yet
- Learning Activity Sheet Name of Student: - Learning Area-Grade Level: Mathematics-Grade 6 Date: - I. Introductory ConceptDocument9 pagesLearning Activity Sheet Name of Student: - Learning Area-Grade Level: Mathematics-Grade 6 Date: - I. Introductory ConceptANGELINA RAMBOYONGNo ratings yet
- Melon Growing Tips PDFDocument1 pageMelon Growing Tips PDFTaahirah Ben ZinatNo ratings yet
- Highlights of Netbeans Ide 7.0 Keyboard Shortcuts & Code TemplatesDocument2 pagesHighlights of Netbeans Ide 7.0 Keyboard Shortcuts & Code TemplatesJOSEPH DAVID CASTILLONo ratings yet
- Job 1 Workout CalendarDocument1 pageJob 1 Workout CalendarnatalipaskalNo ratings yet
- Marie Rochelle - Dangerous BetDocument4 pagesMarie Rochelle - Dangerous BetPaulette Jones50% (2)
- CS401 Bankers Algorithm Exercise FINALDocument6 pagesCS401 Bankers Algorithm Exercise FINALManoj SinwarNo ratings yet




























































































Download as ppt, pdf, or txt
You might also like
- CR Certificate (1465731)Document6 pagesCR Certificate (1465731)rampartnersbusinessllcNo ratings yet
- Czarina Drug Study JuneDocument20 pagesCzarina Drug Study JuneNicoh AvilaNo ratings yet
- Their Eyes Were Watching GodDocument13 pagesTheir Eyes Were Watching Godapi-316773627100% (1)
- PharmacogeneticsDocument30 pagesPharmacogeneticsShailendra Sk100% (3)
- 2principles of Geriatric Pharmacotherapy - Lee - 10-19-10Document53 pages2principles of Geriatric Pharmacotherapy - Lee - 10-19-10Mbel'z Mbel'z Embil'zNo ratings yet
- Adverse Drug ReactionDocument108 pagesAdverse Drug ReactionBinod Sah100% (2)
- 5685 - UHN2012Pharmacogenomic PharmacogeneticDocument44 pages5685 - UHN2012Pharmacogenomic PharmacogeneticAdinda TobingNo ratings yet
- Lecture INST-100046 2022 09 12 04 48 38Document31 pagesLecture INST-100046 2022 09 12 04 48 38Nithya mandalaNo ratings yet
- Dosage Form For Personalized Medicine: HistoryDocument11 pagesDosage Form For Personalized Medicine: HistoryNayeema KhowserNo ratings yet
- Pharmacogenomics 121004112431 Phpapp02Document53 pagesPharmacogenomics 121004112431 Phpapp0288AKK100% (1)
- Farm A Kogen EtikDocument60 pagesFarm A Kogen Etikrahmad wahyudiNo ratings yet
- MCM16-283 Drug Induced DiseasesDocument128 pagesMCM16-283 Drug Induced DiseasesAshraf Khan ShaonNo ratings yet
- Importance of Pharmacogenomics in The Personalized MedicineDocument6 pagesImportance of Pharmacogenomics in The Personalized MedicineJames AustinNo ratings yet
- ADRs - Classification, Mechanism, Predisposing Factors & Causality AssessmentDocument7 pagesADRs - Classification, Mechanism, Predisposing Factors & Causality AssessmentAman UpadhyayNo ratings yet
- Pharmaco GeneticsDocument52 pagesPharmaco GeneticsManikanta GupthaNo ratings yet
- Pharmacogenetics Drug Drug Interactions1Document16 pagesPharmacogenetics Drug Drug Interactions1Marfu'ah Mar'ahNo ratings yet
- Trastuzumab MonographDocument11 pagesTrastuzumab MonographAmeliaNo ratings yet
- Pharmacogenomics:: Increasing The Safety and Effectiveness of Drug TherapyDocument12 pagesPharmacogenomics:: Increasing The Safety and Effectiveness of Drug TherapyFlorentina GasttiNo ratings yet
- Genetics Related Adr With Example FocusingDocument10 pagesGenetics Related Adr With Example Focusingaadrika negiNo ratings yet
- PharmecogenomicsDocument21 pagesPharmecogenomicsRatan Ratan100% (1)
- Theselectionof Antiepilepticdrugs Forthetreatmentof Epilepsyinchildren AndadultsDocument10 pagesTheselectionof Antiepilepticdrugs Forthetreatmentof Epilepsyinchildren AndadultsFaizan MazharNo ratings yet
- Pharmacogenomics: New Challenges For Thai Anesthesiologists: J Med Assoc Thai 2017 100 (Suppl. 7) : S250-S258Document9 pagesPharmacogenomics: New Challenges For Thai Anesthesiologists: J Med Assoc Thai 2017 100 (Suppl. 7) : S250-S258Ronald André Buleje HinostrozaNo ratings yet
- Clin Pharmacy ADRDocument36 pagesClin Pharmacy ADRAnonymous DgPsK0oQNo ratings yet
- Clin Pharmacy ADRDocument24 pagesClin Pharmacy ADRAnonymous DgPsK0oQNo ratings yet
- Critical Limits of Laboratory Results For Urgent Clinician NotificationDocument8 pagesCritical Limits of Laboratory Results For Urgent Clinician NotificationCarl DonaireNo ratings yet
- JIFCC Lab Tests Interpretation 2018Document8 pagesJIFCC Lab Tests Interpretation 2018Abdul Sattar100% (1)
- Farmakogenetik EditDocument60 pagesFarmakogenetik Editfitriadevie451No ratings yet
- Geriatric Pharmacology: Lisa Rosenberg, MD Touro University Nevada April 6, 2011Document45 pagesGeriatric Pharmacology: Lisa Rosenberg, MD Touro University Nevada April 6, 2011Recky Patala100% (1)
- ADRsDocument56 pagesADRsFarina FaraziNo ratings yet
- Drug Interaction-SibyDocument93 pagesDrug Interaction-SibyAswin DamodaranNo ratings yet
- Monitoring Efek Samping Obat 12Document36 pagesMonitoring Efek Samping Obat 12Novitra Dewi100% (1)
- Referensi Nilai KritisDocument9 pagesReferensi Nilai KritisFaiz AchmadNo ratings yet
- Daunorubicin: Drug NameDocument7 pagesDaunorubicin: Drug NameEdgar Ledesma-MartínezNo ratings yet
- Xarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Document26 pagesXarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Dimas RfNo ratings yet
- Anti-Cancer DrugsDocument78 pagesAnti-Cancer DrugsLaghari Jamil100% (1)
- Warfarin - Drug InformationDocument23 pagesWarfarin - Drug InformationTestesteNo ratings yet
- PHARMACOTHERAPY IN GERIATRIC PATIENTS - PPT RF11fcbc - TMP (Dr. Suharti S, SPFK)Document29 pagesPHARMACOTHERAPY IN GERIATRIC PATIENTS - PPT RF11fcbc - TMP (Dr. Suharti S, SPFK)Farid NurdiansyahNo ratings yet
- Introduction To PharmacogenomicsDocument35 pagesIntroduction To Pharmacogenomicssazaki224No ratings yet
- LP CardioDocument8 pagesLP CardioEliza ToteNo ratings yet
- Adverse Drug Reporting (Adrs)Document11 pagesAdverse Drug Reporting (Adrs)Razia JafferyNo ratings yet
- Pharmacogenetics 141110022651 Conversion Gate01Document45 pagesPharmacogenetics 141110022651 Conversion Gate01Jeevan Khanal0% (1)
- Use of Aeds in 2011 and Beyond: Optimizing Clinical ManagementDocument32 pagesUse of Aeds in 2011 and Beyond: Optimizing Clinical ManagementchandanNo ratings yet
- Geriatric Pharmacology DO 22Document41 pagesGeriatric Pharmacology DO 22enghannnNo ratings yet
- Oxford Handbook of Clinical PharmacyDocument10 pagesOxford Handbook of Clinical Pharmacygmsanto7No ratings yet
- Meso 2022Document82 pagesMeso 2022cindi diaNo ratings yet
- Dr. Jarir at Thobari, PHD - Basic Pharmacovigilance PDFDocument35 pagesDr. Jarir at Thobari, PHD - Basic Pharmacovigilance PDFFerina AngeliaNo ratings yet
- Adverse Drug ReactionsDocument14 pagesAdverse Drug Reactionsgaikwaduv98No ratings yet
- Ajovy - Fremanezumab - Drug Information - UpToDateDocument6 pagesAjovy - Fremanezumab - Drug Information - UpToDateDiana PhamNo ratings yet
- LectureDocument29 pagesLectureRiyazuddin MohammedNo ratings yet
- Aspectos Prácticos Nuevos Anticoagulantes Am Jour Hem 2011Document5 pagesAspectos Prácticos Nuevos Anticoagulantes Am Jour Hem 2011jose_esteban_pena_duranNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument32 pagesSee Full Prescribing Information For Complete Boxed WarningGag PafNo ratings yet
- Jamal 2014Document11 pagesJamal 2014Nguyễn Đức LongNo ratings yet
- PharmacogenomicsDocument56 pagesPharmacogenomicsapi-650133203No ratings yet
- MolnupiravirDocument7 pagesMolnupiravirConcepStore PyNo ratings yet
- 9 Personalized MedicineDocument34 pages9 Personalized Medicinehamza najmNo ratings yet
- FILE - 20220726 - 203059 - Gout LUONG MDDocument52 pagesFILE - 20220726 - 203059 - Gout LUONG MDQuang NguyenNo ratings yet
- 14.50 - Richard Fitzgerald - Important Drug InteractionsDocument30 pages14.50 - Richard Fitzgerald - Important Drug Interactionsasif charsiNo ratings yet
- Lecture 8 - PharmacogeneticsDocument38 pagesLecture 8 - PharmacogeneticsNicko WijayaNo ratings yet
- Adverse Effects of ArvsDocument10 pagesAdverse Effects of ArvsAllan Takudzwa MpeperekiNo ratings yet
- Albenza, (Albendazole) Dosing, Indications, Interactions, Adverse Effects, and MoreDocument4 pagesAlbenza, (Albendazole) Dosing, Indications, Interactions, Adverse Effects, and MoreSourav GhoshNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Herbal Supplements: Efficacy, Toxicity, Interactions with Western Drugs, and Effects on Clinical Laboratory TestsFrom EverandHerbal Supplements: Efficacy, Toxicity, Interactions with Western Drugs, and Effects on Clinical Laboratory TestsNo ratings yet
- Erf1899 and 1898 Isipingo HILLSDocument1 pageErf1899 and 1898 Isipingo HILLSTushar PareekNo ratings yet
- Biotechnology ReportDocument137 pagesBiotechnology ReportTushar PareekNo ratings yet
- Pharmacogenomics: The New Step Towards Improving HealthcareDocument14 pagesPharmacogenomics: The New Step Towards Improving HealthcareTushar PareekNo ratings yet
- GAP AnalysisDocument4 pagesGAP AnalysisTushar PareekNo ratings yet
- Emergency ProceduresDocument19 pagesEmergency ProceduresMilos Kalember100% (1)
- Isl and CapstoneDocument6 pagesIsl and Capstoneapi-348627392No ratings yet
- Technical Instruction ABB RED670Document10 pagesTechnical Instruction ABB RED670Iqball ArdiyanNo ratings yet
- How Long A Trip Is It From Here To Our Cairo Office?Document5 pagesHow Long A Trip Is It From Here To Our Cairo Office?Luyện TrầnNo ratings yet
- Social and Prof Issues Module2Document31 pagesSocial and Prof Issues Module2Angelo NebresNo ratings yet
- Introduction To LinguisticsDocument4 pagesIntroduction To LinguisticsRomnick Fernando CoboNo ratings yet
- Blood and Body Fluid SpillageDocument4 pagesBlood and Body Fluid SpillageSony AntonyNo ratings yet
- Truss - 2 Detail: Scale 1: 50 MTRSDocument1 pageTruss - 2 Detail: Scale 1: 50 MTRSGerald MasangayNo ratings yet
- FACTURADocument1 pageFACTURAAnny CañasNo ratings yet
- Safe ManualDocument2 pagesSafe Manualsrujan patelNo ratings yet
- Unit 1 - Foundations of BiochemistryDocument28 pagesUnit 1 - Foundations of BiochemistryJoselitz Reyes TumulakNo ratings yet
- Cost Volume Profit AnalysisDocument12 pagesCost Volume Profit Analysisganeshiyer1467% (3)
- Buckling and Ultimate Strength Assessment For Offshore Structures APRIL 2004Document5 pagesBuckling and Ultimate Strength Assessment For Offshore Structures APRIL 2004Flávio RodriguesNo ratings yet
- Music Link Investigation 1 & 2 Chhairatanak Huy PDFDocument27 pagesMusic Link Investigation 1 & 2 Chhairatanak Huy PDFChay HuyNo ratings yet
- Sheldon Krimsky - Kathleen Sloan - Race and The Genetic Revolution - Science, Myth, and Culture-Columbia University Press (2011)Document300 pagesSheldon Krimsky - Kathleen Sloan - Race and The Genetic Revolution - Science, Myth, and Culture-Columbia University Press (2011)Burnley JenifferNo ratings yet
- InvoiceDocument1 pageInvoiceAyam Goreng0% (1)
- Types of Strategies61Document69 pagesTypes of Strategies61TejashviNo ratings yet
- Conference Board of The Mathematical SciencesDocument43 pagesConference Board of The Mathematical Sciencesjhicks_mathNo ratings yet
- QA Lead Position Interview Questions and AnswersDocument10 pagesQA Lead Position Interview Questions and AnswersAkshay KhotNo ratings yet
- Read The Following Text About A Boy Called Cameron Oliver and His Award. Then, Answer The QuestionsDocument3 pagesRead The Following Text About A Boy Called Cameron Oliver and His Award. Then, Answer The QuestionsYênNo ratings yet
- A Review On The Law of Supply and Demand (Part 1)Document25 pagesA Review On The Law of Supply and Demand (Part 1)Janiña NatividadNo ratings yet
- Ust HtaDocument5 pagesUst HtaSteven SantosNo ratings yet
- Learning Activity Sheet Name of Student: - Learning Area-Grade Level: Mathematics-Grade 6 Date: - I. Introductory ConceptDocument9 pagesLearning Activity Sheet Name of Student: - Learning Area-Grade Level: Mathematics-Grade 6 Date: - I. Introductory ConceptANGELINA RAMBOYONGNo ratings yet
- Melon Growing Tips PDFDocument1 pageMelon Growing Tips PDFTaahirah Ben ZinatNo ratings yet
- Highlights of Netbeans Ide 7.0 Keyboard Shortcuts & Code TemplatesDocument2 pagesHighlights of Netbeans Ide 7.0 Keyboard Shortcuts & Code TemplatesJOSEPH DAVID CASTILLONo ratings yet
- Job 1 Workout CalendarDocument1 pageJob 1 Workout CalendarnatalipaskalNo ratings yet
- Marie Rochelle - Dangerous BetDocument4 pagesMarie Rochelle - Dangerous BetPaulette Jones50% (2)
- CS401 Bankers Algorithm Exercise FINALDocument6 pagesCS401 Bankers Algorithm Exercise FINALManoj SinwarNo ratings yet