Download as ppt, pdf, or txt
You might also like
- Wca-16 Rolls Royce - 250 TV Bow & Stern Tunnel Thrusters PDFDocument115 pagesWca-16 Rolls Royce - 250 TV Bow & Stern Tunnel Thrusters PDFANo ratings yet
- CPG 19Document78 pagesCPG 19anon-24970100% (1)
- Treatment of VKC: 1. Nonpharmacologic Treatment 2. Pharmacologic Treatment 3. Surgery TreatmentDocument18 pagesTreatment of VKC: 1. Nonpharmacologic Treatment 2. Pharmacologic Treatment 3. Surgery TreatmentAllen SallyNo ratings yet
- Tutorial Chapter 1 - 0 ThermodynamicDocument2 pagesTutorial Chapter 1 - 0 ThermodynamicSufferedMuchNo ratings yet
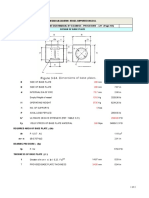
- Leg Support Calculation PDFDocument2 pagesLeg Support Calculation PDFSanjay MoreNo ratings yet
- Glaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913From EverandGlaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913No ratings yet
- Cataract And Small Pupil Management Manual Techniques: 2022, #1From EverandCataract And Small Pupil Management Manual Techniques: 2022, #1No ratings yet
- Ophthalmology History TakingDocument12 pagesOphthalmology History TakingRizki MeizikriNo ratings yet
- Nungki-Esodeviations & ExodeviationsDocument36 pagesNungki-Esodeviations & ExodeviationsNia RoosdhantiaNo ratings yet
- UveaDocument83 pagesUveaShewit TeklehaymanotNo ratings yet
- Week 4 - Development of The EyeDocument5 pagesWeek 4 - Development of The EyeAleia GoNo ratings yet
- Optic NeuritisDocument32 pagesOptic NeuritisNajaf Ali Khan100% (1)
- Night MiopiaDocument8 pagesNight MiopiamurilobsouzaNo ratings yet
- StrabismusDocument19 pagesStrabismusSoumya Ranjan PandaNo ratings yet
- Orientation, History Taking and ExaminationDocument77 pagesOrientation, History Taking and ExaminationMuhammad AwaisNo ratings yet
- Trabeculectomy TechniqueDocument8 pagesTrabeculectomy TechniqueJose Antonio Fuentes VegaNo ratings yet
- Soft Contact Lens DesignDocument82 pagesSoft Contact Lens DesignRuthi HnamteNo ratings yet
- Investigation in OptometryDocument10 pagesInvestigation in Optometryrapid73No ratings yet
- What Is Retinoscopy?: Myopia HyperopiaDocument4 pagesWhat Is Retinoscopy?: Myopia HyperopiababyswitNo ratings yet
- Eyes On Eyecare - 2021 - Dry Eye ReportDocument28 pagesEyes On Eyecare - 2021 - Dry Eye ReportEsther AlonsoNo ratings yet
- Mechanisms of Cataract Formation: Nicholas Phelps Brown MD, FRCS, FrcophthDocument7 pagesMechanisms of Cataract Formation: Nicholas Phelps Brown MD, FRCS, FrcophthQomariah RiaNo ratings yet
- Anisometropia in Children and Its ProblemDocument37 pagesAnisometropia in Children and Its ProblemekaNo ratings yet
- Soft Multifocal Simultaneous Image Contact Lenses A ReviewDocument21 pagesSoft Multifocal Simultaneous Image Contact Lenses A ReviewBAYUNo ratings yet
- Low Vision ChartsDocument13 pagesLow Vision ChartsAkash BJ SmartNo ratings yet
- OculomotorDocument41 pagesOculomotorcmirceaNo ratings yet
- Smith Test, Goniolens, Shadow TestDocument3 pagesSmith Test, Goniolens, Shadow TestJLo100% (1)
- 1 - Orientation, History Taking and ExaminationDocument96 pages1 - Orientation, History Taking and ExaminationHari ShresthaNo ratings yet
- Refractive Errors: Dr. Leow Thye YngDocument55 pagesRefractive Errors: Dr. Leow Thye YngRaissaNo ratings yet
- American Optometric Association. Glaucoma HTTP - WWW - Aoa.org - Glaucoma - Xml.Document8 pagesAmerican Optometric Association. Glaucoma HTTP - WWW - Aoa.org - Glaucoma - Xml.Adriana Falla100% (1)
- Anatomy of Eyelid: Presenter:-Dr. Vijayalaxmi Moderator:-Dr. SanjanaDocument49 pagesAnatomy of Eyelid: Presenter:-Dr. Vijayalaxmi Moderator:-Dr. SanjanaRidhi Bhandari100% (1)
- 4 Contact LensesDocument17 pages4 Contact LensesRaison D EtreNo ratings yet
- Anatomy of Uvea: Dr. Binu AsharafDocument48 pagesAnatomy of Uvea: Dr. Binu AsharafBinu AshrafNo ratings yet
- Ocular EmergDocument61 pagesOcular EmergKBR RS UNHAS100% (1)
- Clinical Optometry Primary Eye CareDocument3 pagesClinical Optometry Primary Eye CareDanielle SangalangNo ratings yet
- Artificial TearsDocument36 pagesArtificial TearsFahmi Rizal100% (1)
- Optics - Contact Lens Related - MMSDocument38 pagesOptics - Contact Lens Related - MMSManmohan ShahNo ratings yet
- Method of Extending The Range of The KeratometerDocument3 pagesMethod of Extending The Range of The KeratometerDanielle SangalangNo ratings yet
- Contact Lenses Chemicals, Methods, and Applications PDFDocument448 pagesContact Lenses Chemicals, Methods, and Applications PDFantonioNo ratings yet
- AniseikoniaDocument40 pagesAniseikoniahenok biruk100% (1)
- Accommodation Dysfunction: DR Neelu AgrawalDocument30 pagesAccommodation Dysfunction: DR Neelu AgrawalNeelu MundhadaAgrawalNo ratings yet
- Development of Binocular Vision: University of Gondar Department of Optometry by Nebiyat FelekeDocument35 pagesDevelopment of Binocular Vision: University of Gondar Department of Optometry by Nebiyat Felekehenok birukNo ratings yet
- Colour Vision AnomaliesDocument27 pagesColour Vision AnomaliesGershon Hayford100% (1)
- 01-Eyehistory Part2Document3 pages01-Eyehistory Part2sharu4291No ratings yet
- Concomitant SquintDocument21 pagesConcomitant SquintShivani Nair100% (1)
- RefraksiDocument84 pagesRefraksinaroetocapkutilNo ratings yet
- Ocular Manifestations of Thyroid DiseaseDocument20 pagesOcular Manifestations of Thyroid Diseasevivekrajbhilai5850No ratings yet
- 6.cross-Cylinder Technique For Determining AstigmatismDocument4 pages6.cross-Cylinder Technique For Determining Astigmatismtoman88No ratings yet
- 2010 Clinical Guide To Ophthalmic DrugsDocument52 pages2010 Clinical Guide To Ophthalmic DrugsJonathan PenmNo ratings yet
- 8-Strabismus & AmbliopiaDocument24 pages8-Strabismus & AmbliopiaMuhammad Faisal100% (1)
- OptoPrep Part1 StudyCalendar 6-Month PDFDocument7 pagesOptoPrep Part1 StudyCalendar 6-Month PDFmelanieNo ratings yet
- Mechanical Properties of Contact Lens Materials EKDocument10 pagesMechanical Properties of Contact Lens Materials EKAybüke ÇalıkoğluNo ratings yet
- Diseases of Lacrimal ApparatusDocument46 pagesDiseases of Lacrimal Apparatusসপ্নে ছোয়া মন100% (1)
- Contact Lenses For ChildrenDocument6 pagesContact Lenses For ChildrenmelikebooksNo ratings yet
- Congenital Strabismus: S. Vanitha, B.optom, 3 YearDocument23 pagesCongenital Strabismus: S. Vanitha, B.optom, 3 YearDivya Priya Dharmalingam100% (1)
- RGP Lens MeasurementDocument5 pagesRGP Lens MeasurementSumon SarkarNo ratings yet
- Bifocal Contact Lenses PDFDocument10 pagesBifocal Contact Lenses PDFLauw Dwi AndrikNo ratings yet
- Optometric Optics-II Dispensing OpticsDocument2 pagesOptometric Optics-II Dispensing OpticsABHIJIT DEBNATH100% (1)
- Anomalie VisionDocument13 pagesAnomalie VisionblueiceNo ratings yet
- (K14) - Contact LensesDocument33 pages(K14) - Contact LensesSyarifah FauziahNo ratings yet
- Large ExotropiaDocument67 pagesLarge ExotropiaTri Kartika UtomoNo ratings yet
- Intra-Ocular Lens: Vishnu NarayananDocument38 pagesIntra-Ocular Lens: Vishnu NarayananArif MohammadNo ratings yet
- Divergent Strabismus (1) - 10Document65 pagesDivergent Strabismus (1) - 10Lavanya MadabushiNo ratings yet
- Examination of The Eye - GitaDocument42 pagesExamination of The Eye - Gitaalfarizyjefry100% (1)
- AD Review PDFDocument13 pagesAD Review PDFalfarizyjefryNo ratings yet
- Case Report PresentationDocument27 pagesCase Report PresentationalfarizyjefryNo ratings yet
- 2018 Jadwal 2018 Revisi Final-1Document18 pages2018 Jadwal 2018 Revisi Final-1alfarizyjefryNo ratings yet
- Daftar Kelompok Kepaniteraan Klinik FK Untan 2018: No Nama Mahasiswa NIM Kelompok KeteranganDocument18 pagesDaftar Kelompok Kepaniteraan Klinik FK Untan 2018: No Nama Mahasiswa NIM Kelompok KeteranganalfarizyjefryNo ratings yet
- Business Presentation YAKULTDocument12 pagesBusiness Presentation YAKULTJosuaNo ratings yet
- Visual Storytelling The Digital Video Documentary - Original PDFDocument44 pagesVisual Storytelling The Digital Video Documentary - Original PDFjparanoti100% (1)
- Anthropological Thought Session by DR G. VivekanandaDocument277 pagesAnthropological Thought Session by DR G. Vivekanandahamtum7861No ratings yet
- English Final Test Grade XiiDocument9 pagesEnglish Final Test Grade XiiLiza RahmawatiNo ratings yet
- Credit Card Fraud Detection Using Improved Deep Learning ModelsDocument22 pagesCredit Card Fraud Detection Using Improved Deep Learning ModelsrauhNo ratings yet
- SOM016 - Hook Release System For Life Boats. Norsafe TOR mk2.Document20 pagesSOM016 - Hook Release System For Life Boats. Norsafe TOR mk2.arfaoui salimNo ratings yet
- TSB-1139 8SC Wiring DiagramDocument2 pagesTSB-1139 8SC Wiring Diagramxavier marsNo ratings yet
- Wind EnergyDocument6 pagesWind EnergyRajat DubeyNo ratings yet
- Behaviour of Hollow Core Slabs Under Point LoadsDocument17 pagesBehaviour of Hollow Core Slabs Under Point LoadsVálter LúcioNo ratings yet
- 5 25 17 Migraines PowerPointDocument40 pages5 25 17 Migraines PowerPointSaifi AlamNo ratings yet
- Final Firefly Reading & Writing AnswerDocument70 pagesFinal Firefly Reading & Writing AnswerVamshidhar ReddyNo ratings yet
- BEL PE Question Papers For ECE With Answers - 6 Knowledge AddaDocument14 pagesBEL PE Question Papers For ECE With Answers - 6 Knowledge AddaVishwanand ThombareNo ratings yet
- Palliative Ultrasound-Guided Endoscopic Diode Laser Ablation of Transitional Cell Carcinomas of The Lower Urinary Tract in Dogs.Document10 pagesPalliative Ultrasound-Guided Endoscopic Diode Laser Ablation of Transitional Cell Carcinomas of The Lower Urinary Tract in Dogs.Dante Nathaniel FajardoNo ratings yet
- Is-Cal01 Design Carbon Accounting On Site Rev.02Document6 pagesIs-Cal01 Design Carbon Accounting On Site Rev.02shoba9945No ratings yet
- Material Balance PDFDocument31 pagesMaterial Balance PDFApril Joy HaroNo ratings yet
- HEI Tech Sheet 110Document15 pagesHEI Tech Sheet 110Suganya LokeshNo ratings yet
- The Fruit Garden CAL: Columbine & AcanthusDocument7 pagesThe Fruit Garden CAL: Columbine & AcanthusMiraNo ratings yet
- DC Jow Ga Beginner CurriculumDocument2 pagesDC Jow Ga Beginner CurriculumKevinNo ratings yet
- An Overview of Discourse AnalysisDocument26 pagesAn Overview of Discourse Analysisjamogi2943No ratings yet
- Bristol Comp Catalog 4Document102 pagesBristol Comp Catalog 4Popica ClaudiuNo ratings yet
- Geometry - Olympiad Material BY DR SHYAM SUNDAR AGRAWALDocument67 pagesGeometry - Olympiad Material BY DR SHYAM SUNDAR AGRAWALdrssagrawalNo ratings yet
- UntitledDocument4 pagesUntitleddwky KrnwnNo ratings yet
- Arthur Lumley Davi̇ds-Sultan Ii. Mahmuta-1832Document318 pagesArthur Lumley Davi̇ds-Sultan Ii. Mahmuta-1832cengizozakinciNo ratings yet
- UntitledDocument14 pagesUntitlednaresh kumarNo ratings yet
- Oil & Chemical Tanker Summer 7 - Prepurchase Survey Report - S&a 230098 PpsDocument62 pagesOil & Chemical Tanker Summer 7 - Prepurchase Survey Report - S&a 230098 Ppsp_k_sahuNo ratings yet
- Tax System SriLankaDocument44 pagesTax System SriLankamandarak7146No ratings yet
- Operation Reasrech On IglooDocument18 pagesOperation Reasrech On IglooMd Yeasin ArafatNo ratings yet