
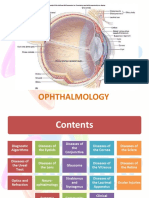
RETINA
RETINA
You might also like
- Penetrating Keratoplasty StepsDocument57 pagesPenetrating Keratoplasty StepsVishwajeetNo ratings yet
- David R. Hawkins - Attractor Field TechniqueDocument55 pagesDavid R. Hawkins - Attractor Field TechniqueMarkWoodxxx84% (31)
- Ico Oscar SicsDocument5 pagesIco Oscar Sicsbrahmani pitanatriNo ratings yet
- OphthalmologyDocument144 pagesOphthalmologyrosaririsNo ratings yet
- Papiledema 3Document27 pagesPapiledema 3nellieauthorNo ratings yet
- Mata Tenang Visus Turun MendadakDocument75 pagesMata Tenang Visus Turun MendadakDianMuliasariNo ratings yet
- Dr. Dr. Habibah S. Muhiddin, SP.M (K) : Departement of Ophthalmology Faculty of Medicine Hasanuddin UniversityDocument31 pagesDr. Dr. Habibah S. Muhiddin, SP.M (K) : Departement of Ophthalmology Faculty of Medicine Hasanuddin UniversityRey AlwiwikhNo ratings yet
- Anisman Acute Vision LossDocument68 pagesAnisman Acute Vision Lossarnol3090No ratings yet
- Veno Occlusive Disease of RetinaDocument81 pagesVeno Occlusive Disease of RetinaPreetiNo ratings yet
- Correlation of Retinal Structural Alteration With Retinal Sensitivity Loss: A Prospective StudyDocument26 pagesCorrelation of Retinal Structural Alteration With Retinal Sensitivity Loss: A Prospective StudyAbhishek KothariNo ratings yet
- 14th SOM LAMPUNG 2020 PROPOSALDocument23 pages14th SOM LAMPUNG 2020 PROPOSALnovitaNo ratings yet
- Ocular Toxoplasmosis: Causative Agent Toxoplasma Gondi An Obligate, Intracellular ParasiteDocument15 pagesOcular Toxoplasmosis: Causative Agent Toxoplasma Gondi An Obligate, Intracellular Parasitehenok biruk100% (1)
- A Course in Low Vision PracticeDocument12 pagesA Course in Low Vision PracticeDr. Candy Delos Reyes-BarluadoNo ratings yet
- Retina Examination and Drawing: CEH Retinal TeamDocument39 pagesRetina Examination and Drawing: CEH Retinal TeamrzmNo ratings yet
- Mata Tenang Visus Turun MendadakDocument74 pagesMata Tenang Visus Turun MendadakYeni AnggrainiNo ratings yet
- Disease of UveaDocument21 pagesDisease of UveaMarshet GeteNo ratings yet
- Low VisionDocument36 pagesLow VisionIqbal HabibieNo ratings yet
- Clinical Approach To Optic Neuropathies: DiagnosisDocument14 pagesClinical Approach To Optic Neuropathies: Diagnosiskmathewjames100% (1)
- Anterior Chamber Angle Assessment TechniquesDocument29 pagesAnterior Chamber Angle Assessment TechniquesSabyasachi100% (4)
- Observations During Fundus ExaminationDocument3 pagesObservations During Fundus ExaminationAn'umillah Arini ZidnaNo ratings yet
- Central Serous Retinopathy PPT-2Document28 pagesCentral Serous Retinopathy PPT-2Vaishu SgsNo ratings yet
- Printout DONE... PM MCQs 2019 EYEDocument32 pagesPrintout DONE... PM MCQs 2019 EYEKiran ShahNo ratings yet
- RAPDDocument2 pagesRAPDAlpascaFirdausNo ratings yet
- 94 - CH 10 - Symptoms in Heterophoria and Heterotropia and The Psychological Effects of Strabismus P. 153-157Document5 pages94 - CH 10 - Symptoms in Heterophoria and Heterotropia and The Psychological Effects of Strabismus P. 153-157Catleya ProtacioNo ratings yet
- Anatomy and Histology of ConjunctivaDocument36 pagesAnatomy and Histology of ConjunctivaMohan RamNo ratings yet
- Diagram TMGDocument20 pagesDiagram TMGBima RizkiNo ratings yet
- Anatomi Dan Embriologi Mata: Julie D BarlianaDocument31 pagesAnatomi Dan Embriologi Mata: Julie D BarlianaAyunita PermataNo ratings yet
- Laporan Kasus Katarak Fathonah (1102013108) .Id - enDocument48 pagesLaporan Kasus Katarak Fathonah (1102013108) .Id - enAnonymous ZbhBxeEVNo ratings yet
- Mata MerahDocument59 pagesMata MerahAmalliaPradisthaNo ratings yet
- Age-Related Macular Disease: Fitriani Umi Hasanah 201820401011121 Pembimbing: Dr. Fatin Hamamah, SP.MDocument28 pagesAge-Related Macular Disease: Fitriani Umi Hasanah 201820401011121 Pembimbing: Dr. Fatin Hamamah, SP.MKim NayoungNo ratings yet
- LEUKOKORIADocument3 pagesLEUKOKORIAFahlevie EpinNo ratings yet
- Aao Bab 4Document3 pagesAao Bab 4ria mutiaraNo ratings yet
- Gupta Et Al. - 2015 - Retinal Anatomy and PathologyDocument12 pagesGupta Et Al. - 2015 - Retinal Anatomy and PathologyFelicia SutarliNo ratings yet
- Toric IolDocument15 pagesToric IolPande AdityoNo ratings yet
- BHP Phaco Umum Dan Langganan BHP Dengan Lensa Premium KALBE 2,100,000 NO BHP Satuan Pemakaian Harga TotalDocument7 pagesBHP Phaco Umum Dan Langganan BHP Dengan Lensa Premium KALBE 2,100,000 NO BHP Satuan Pemakaian Harga Totalr.mardhiyah delimaNo ratings yet
- Soal Subdivisi Roo Eyelid NeoplasmDocument8 pagesSoal Subdivisi Roo Eyelid NeoplasmBudhi KaromaNo ratings yet
- Subluksasi LensaDocument12 pagesSubluksasi LensaDede GunawanNo ratings yet
- Diagram For Ophtal NoteDocument7 pagesDiagram For Ophtal NoteSiam Weng LoongNo ratings yet
- Soal OFKOMDocument3 pagesSoal OFKOMDian ArianiNo ratings yet
- A Review of Anti-Vegf Agents For Proliferative Diabetic RetinopathyDocument7 pagesA Review of Anti-Vegf Agents For Proliferative Diabetic RetinopathyIJAR JOURNALNo ratings yet
- Diseases of The Optic Nerve 09Document25 pagesDiseases of The Optic Nerve 09somebody_maNo ratings yet
- Limbal DermoidDocument4 pagesLimbal DermoidPranjali ChhayaNo ratings yet
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- Presentasi Low VisionDocument30 pagesPresentasi Low VisionAySa AysaNo ratings yet
- Periorbital and Orbital CellulitisDocument51 pagesPeriorbital and Orbital CellulitisJoanne BlancoNo ratings yet
- AmblyopiaDocument33 pagesAmblyopiaSujon PaulNo ratings yet
- Trauma MataDocument57 pagesTrauma MataFatmala Umi MaisarahNo ratings yet
- Corneal Drawing and Other StructureDocument2 pagesCorneal Drawing and Other StructureOden Mahyudin50% (2)
- Ophthalmology Card AnswersDocument29 pagesOphthalmology Card AnswersRaihan MahmudNo ratings yet
- Ocular EmergDocument61 pagesOcular EmergKBR RS UNHAS100% (1)
- Retinitis Pigmentosa: Common Clinical ConditionsDocument32 pagesRetinitis Pigmentosa: Common Clinical ConditionsDhruval Parekh100% (1)
- Kuliah LV-LOW Vision DeviceDocument22 pagesKuliah LV-LOW Vision DevicemazidahzulfaNo ratings yet
- Kuliah KBK - Anesthesia For Ophthalmic SurgeryDocument18 pagesKuliah KBK - Anesthesia For Ophthalmic SurgeryAndy Abraham RanganNo ratings yet
- Right Lower Lid Entropion in A 79-Year-Old Female: A Case-ReportDocument4 pagesRight Lower Lid Entropion in A 79-Year-Old Female: A Case-Reportfadil ahmadiNo ratings yet
- Scleritis: Moderator: DR Sangeetha Patil Presenter: DR Shraddha SudarshanDocument85 pagesScleritis: Moderator: DR Sangeetha Patil Presenter: DR Shraddha Sudarshanshraddha sudarshanNo ratings yet
- CataractDocument126 pagesCataractSahul Hameed100% (2)
- Uveitis: - Presented By: - The Boys Batch 28Document40 pagesUveitis: - Presented By: - The Boys Batch 28Abdul MajeedNo ratings yet
- 19 Rationale of Retinal Detachment ManagementDocument87 pages19 Rationale of Retinal Detachment ManagementvajasaNo ratings yet
- Evaluation of PupilDocument28 pagesEvaluation of PupilArlinda Silva PrameswariNo ratings yet
- Glaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913From EverandGlaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913No ratings yet
- Hey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsFrom EverandHey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsNo ratings yet
- Photo TherapyDocument7 pagesPhoto TherapyMaysa Ismail100% (1)
- Acute Management of Pulmonary Embolism - American College of CardiologyDocument22 pagesAcute Management of Pulmonary Embolism - American College of CardiologyRaja GopalNo ratings yet
- Esophageal VaricesDocument3 pagesEsophageal VaricesSasa LuarNo ratings yet
- Medtech Laws and Bioethics MTE 114Document3 pagesMedtech Laws and Bioethics MTE 114Lowin NavarroNo ratings yet
- Insulin AspartDocument2 pagesInsulin AspartPatricia MaglasangNo ratings yet
- Initial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentDocument3 pagesInitial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentLamNo ratings yet
- Safety Training ProgramDocument43 pagesSafety Training ProgramBhavesh PatelNo ratings yet
- Scenihr o 046Document116 pagesScenihr o 046Ana NicoletaNo ratings yet
- Hipaa Privacy NoticeDocument5 pagesHipaa Privacy Noticeapi-580264080No ratings yet
- Mrinal DissertationDocument49 pagesMrinal DissertationMRINAL RATNAMNo ratings yet
- WI Medication AdministrationDocument11 pagesWI Medication AdministrationVin BitzNo ratings yet
- PhenylketonuriaDocument1 pagePhenylketonuriaHolly SevillanoNo ratings yet
- Guideline For Empanelment of Hospital Under MA Yojana PDFDocument43 pagesGuideline For Empanelment of Hospital Under MA Yojana PDFVijay BaldaniyaNo ratings yet
- Activity Desig FINAL SPORTS AND ARTS 1Document4 pagesActivity Desig FINAL SPORTS AND ARTS 1Marc QuiaNo ratings yet
- Public Perceptions of Arguments Supporting and OpposingDocument23 pagesPublic Perceptions of Arguments Supporting and OpposingmafmortensonNo ratings yet
- Master The Pike - ForumsDocument2 pagesMaster The Pike - ForumsJacklynlim LkcNo ratings yet
- 3.mellennium Development Goals (MDG)Document30 pages3.mellennium Development Goals (MDG)Brave TulaganNo ratings yet
- Developer Productivity-SPACE FrameworkDocument29 pagesDeveloper Productivity-SPACE FrameworkSrinivasan VenkatNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineGodfrey Loth Sales Alcansare Jr.No ratings yet
- Hand Washing LessonDocument6 pagesHand Washing Lessonapi-278856455No ratings yet
- Photography NC Ii: Visual Arts SectorDocument71 pagesPhotography NC Ii: Visual Arts SectorPaul Omar PastranoNo ratings yet
- Emmanuel'S Resort: Samay, BalingasagDocument4 pagesEmmanuel'S Resort: Samay, BalingasagBryan LluismaNo ratings yet
- Kuliah ATLSDocument63 pagesKuliah ATLSDwianggriany Adhetia Piesca Widoretno100% (1)
- Miakatar17432825 Contemporary Teacher Leadership Report Assignment 1Document39 pagesMiakatar17432825 Contemporary Teacher Leadership Report Assignment 1api-408516682No ratings yet
- Test Health and DiseasesDocument4 pagesTest Health and DiseasesAndrea Anderson-HydeNo ratings yet
- Subjective: Short Term: Independent: Short TermDocument2 pagesSubjective: Short Term: Independent: Short TermCamille SesaldoNo ratings yet
- President Kaguta Museveni's Speech On Covid-19 As of 18 June 2021Document26 pagesPresident Kaguta Museveni's Speech On Covid-19 As of 18 June 2021The Campus TimesNo ratings yet
- Cerebro Lys inDocument18 pagesCerebro Lys inKathleen PalomariaNo ratings yet
- Dental Town 2016Document23 pagesDental Town 2016Tahir AliNo ratings yet
























































































Download as pptx, pdf, or txt
You might also like
- Penetrating Keratoplasty StepsDocument57 pagesPenetrating Keratoplasty StepsVishwajeetNo ratings yet
- David R. Hawkins - Attractor Field TechniqueDocument55 pagesDavid R. Hawkins - Attractor Field TechniqueMarkWoodxxx84% (31)
- Ico Oscar SicsDocument5 pagesIco Oscar Sicsbrahmani pitanatriNo ratings yet
- OphthalmologyDocument144 pagesOphthalmologyrosaririsNo ratings yet
- Papiledema 3Document27 pagesPapiledema 3nellieauthorNo ratings yet
- Mata Tenang Visus Turun MendadakDocument75 pagesMata Tenang Visus Turun MendadakDianMuliasariNo ratings yet
- Dr. Dr. Habibah S. Muhiddin, SP.M (K) : Departement of Ophthalmology Faculty of Medicine Hasanuddin UniversityDocument31 pagesDr. Dr. Habibah S. Muhiddin, SP.M (K) : Departement of Ophthalmology Faculty of Medicine Hasanuddin UniversityRey AlwiwikhNo ratings yet
- Anisman Acute Vision LossDocument68 pagesAnisman Acute Vision Lossarnol3090No ratings yet
- Veno Occlusive Disease of RetinaDocument81 pagesVeno Occlusive Disease of RetinaPreetiNo ratings yet
- Correlation of Retinal Structural Alteration With Retinal Sensitivity Loss: A Prospective StudyDocument26 pagesCorrelation of Retinal Structural Alteration With Retinal Sensitivity Loss: A Prospective StudyAbhishek KothariNo ratings yet
- 14th SOM LAMPUNG 2020 PROPOSALDocument23 pages14th SOM LAMPUNG 2020 PROPOSALnovitaNo ratings yet
- Ocular Toxoplasmosis: Causative Agent Toxoplasma Gondi An Obligate, Intracellular ParasiteDocument15 pagesOcular Toxoplasmosis: Causative Agent Toxoplasma Gondi An Obligate, Intracellular Parasitehenok biruk100% (1)
- A Course in Low Vision PracticeDocument12 pagesA Course in Low Vision PracticeDr. Candy Delos Reyes-BarluadoNo ratings yet
- Retina Examination and Drawing: CEH Retinal TeamDocument39 pagesRetina Examination and Drawing: CEH Retinal TeamrzmNo ratings yet
- Mata Tenang Visus Turun MendadakDocument74 pagesMata Tenang Visus Turun MendadakYeni AnggrainiNo ratings yet
- Disease of UveaDocument21 pagesDisease of UveaMarshet GeteNo ratings yet
- Low VisionDocument36 pagesLow VisionIqbal HabibieNo ratings yet
- Clinical Approach To Optic Neuropathies: DiagnosisDocument14 pagesClinical Approach To Optic Neuropathies: Diagnosiskmathewjames100% (1)
- Anterior Chamber Angle Assessment TechniquesDocument29 pagesAnterior Chamber Angle Assessment TechniquesSabyasachi100% (4)
- Observations During Fundus ExaminationDocument3 pagesObservations During Fundus ExaminationAn'umillah Arini ZidnaNo ratings yet
- Central Serous Retinopathy PPT-2Document28 pagesCentral Serous Retinopathy PPT-2Vaishu SgsNo ratings yet
- Printout DONE... PM MCQs 2019 EYEDocument32 pagesPrintout DONE... PM MCQs 2019 EYEKiran ShahNo ratings yet
- RAPDDocument2 pagesRAPDAlpascaFirdausNo ratings yet
- 94 - CH 10 - Symptoms in Heterophoria and Heterotropia and The Psychological Effects of Strabismus P. 153-157Document5 pages94 - CH 10 - Symptoms in Heterophoria and Heterotropia and The Psychological Effects of Strabismus P. 153-157Catleya ProtacioNo ratings yet
- Anatomy and Histology of ConjunctivaDocument36 pagesAnatomy and Histology of ConjunctivaMohan RamNo ratings yet
- Diagram TMGDocument20 pagesDiagram TMGBima RizkiNo ratings yet
- Anatomi Dan Embriologi Mata: Julie D BarlianaDocument31 pagesAnatomi Dan Embriologi Mata: Julie D BarlianaAyunita PermataNo ratings yet
- Laporan Kasus Katarak Fathonah (1102013108) .Id - enDocument48 pagesLaporan Kasus Katarak Fathonah (1102013108) .Id - enAnonymous ZbhBxeEVNo ratings yet
- Mata MerahDocument59 pagesMata MerahAmalliaPradisthaNo ratings yet
- Age-Related Macular Disease: Fitriani Umi Hasanah 201820401011121 Pembimbing: Dr. Fatin Hamamah, SP.MDocument28 pagesAge-Related Macular Disease: Fitriani Umi Hasanah 201820401011121 Pembimbing: Dr. Fatin Hamamah, SP.MKim NayoungNo ratings yet
- LEUKOKORIADocument3 pagesLEUKOKORIAFahlevie EpinNo ratings yet
- Aao Bab 4Document3 pagesAao Bab 4ria mutiaraNo ratings yet
- Gupta Et Al. - 2015 - Retinal Anatomy and PathologyDocument12 pagesGupta Et Al. - 2015 - Retinal Anatomy and PathologyFelicia SutarliNo ratings yet
- Toric IolDocument15 pagesToric IolPande AdityoNo ratings yet
- BHP Phaco Umum Dan Langganan BHP Dengan Lensa Premium KALBE 2,100,000 NO BHP Satuan Pemakaian Harga TotalDocument7 pagesBHP Phaco Umum Dan Langganan BHP Dengan Lensa Premium KALBE 2,100,000 NO BHP Satuan Pemakaian Harga Totalr.mardhiyah delimaNo ratings yet
- Soal Subdivisi Roo Eyelid NeoplasmDocument8 pagesSoal Subdivisi Roo Eyelid NeoplasmBudhi KaromaNo ratings yet
- Subluksasi LensaDocument12 pagesSubluksasi LensaDede GunawanNo ratings yet
- Diagram For Ophtal NoteDocument7 pagesDiagram For Ophtal NoteSiam Weng LoongNo ratings yet
- Soal OFKOMDocument3 pagesSoal OFKOMDian ArianiNo ratings yet
- A Review of Anti-Vegf Agents For Proliferative Diabetic RetinopathyDocument7 pagesA Review of Anti-Vegf Agents For Proliferative Diabetic RetinopathyIJAR JOURNALNo ratings yet
- Diseases of The Optic Nerve 09Document25 pagesDiseases of The Optic Nerve 09somebody_maNo ratings yet
- Limbal DermoidDocument4 pagesLimbal DermoidPranjali ChhayaNo ratings yet
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- Presentasi Low VisionDocument30 pagesPresentasi Low VisionAySa AysaNo ratings yet
- Periorbital and Orbital CellulitisDocument51 pagesPeriorbital and Orbital CellulitisJoanne BlancoNo ratings yet
- AmblyopiaDocument33 pagesAmblyopiaSujon PaulNo ratings yet
- Trauma MataDocument57 pagesTrauma MataFatmala Umi MaisarahNo ratings yet
- Corneal Drawing and Other StructureDocument2 pagesCorneal Drawing and Other StructureOden Mahyudin50% (2)
- Ophthalmology Card AnswersDocument29 pagesOphthalmology Card AnswersRaihan MahmudNo ratings yet
- Ocular EmergDocument61 pagesOcular EmergKBR RS UNHAS100% (1)
- Retinitis Pigmentosa: Common Clinical ConditionsDocument32 pagesRetinitis Pigmentosa: Common Clinical ConditionsDhruval Parekh100% (1)
- Kuliah LV-LOW Vision DeviceDocument22 pagesKuliah LV-LOW Vision DevicemazidahzulfaNo ratings yet
- Kuliah KBK - Anesthesia For Ophthalmic SurgeryDocument18 pagesKuliah KBK - Anesthesia For Ophthalmic SurgeryAndy Abraham RanganNo ratings yet
- Right Lower Lid Entropion in A 79-Year-Old Female: A Case-ReportDocument4 pagesRight Lower Lid Entropion in A 79-Year-Old Female: A Case-Reportfadil ahmadiNo ratings yet
- Scleritis: Moderator: DR Sangeetha Patil Presenter: DR Shraddha SudarshanDocument85 pagesScleritis: Moderator: DR Sangeetha Patil Presenter: DR Shraddha Sudarshanshraddha sudarshanNo ratings yet
- CataractDocument126 pagesCataractSahul Hameed100% (2)
- Uveitis: - Presented By: - The Boys Batch 28Document40 pagesUveitis: - Presented By: - The Boys Batch 28Abdul MajeedNo ratings yet
- 19 Rationale of Retinal Detachment ManagementDocument87 pages19 Rationale of Retinal Detachment ManagementvajasaNo ratings yet
- Evaluation of PupilDocument28 pagesEvaluation of PupilArlinda Silva PrameswariNo ratings yet
- Glaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913From EverandGlaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913No ratings yet
- Hey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsFrom EverandHey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsNo ratings yet
- Photo TherapyDocument7 pagesPhoto TherapyMaysa Ismail100% (1)
- Acute Management of Pulmonary Embolism - American College of CardiologyDocument22 pagesAcute Management of Pulmonary Embolism - American College of CardiologyRaja GopalNo ratings yet
- Esophageal VaricesDocument3 pagesEsophageal VaricesSasa LuarNo ratings yet
- Medtech Laws and Bioethics MTE 114Document3 pagesMedtech Laws and Bioethics MTE 114Lowin NavarroNo ratings yet
- Insulin AspartDocument2 pagesInsulin AspartPatricia MaglasangNo ratings yet
- Initial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentDocument3 pagesInitial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentLamNo ratings yet
- Safety Training ProgramDocument43 pagesSafety Training ProgramBhavesh PatelNo ratings yet
- Scenihr o 046Document116 pagesScenihr o 046Ana NicoletaNo ratings yet
- Hipaa Privacy NoticeDocument5 pagesHipaa Privacy Noticeapi-580264080No ratings yet
- Mrinal DissertationDocument49 pagesMrinal DissertationMRINAL RATNAMNo ratings yet
- WI Medication AdministrationDocument11 pagesWI Medication AdministrationVin BitzNo ratings yet
- PhenylketonuriaDocument1 pagePhenylketonuriaHolly SevillanoNo ratings yet
- Guideline For Empanelment of Hospital Under MA Yojana PDFDocument43 pagesGuideline For Empanelment of Hospital Under MA Yojana PDFVijay BaldaniyaNo ratings yet
- Activity Desig FINAL SPORTS AND ARTS 1Document4 pagesActivity Desig FINAL SPORTS AND ARTS 1Marc QuiaNo ratings yet
- Public Perceptions of Arguments Supporting and OpposingDocument23 pagesPublic Perceptions of Arguments Supporting and OpposingmafmortensonNo ratings yet
- Master The Pike - ForumsDocument2 pagesMaster The Pike - ForumsJacklynlim LkcNo ratings yet
- 3.mellennium Development Goals (MDG)Document30 pages3.mellennium Development Goals (MDG)Brave TulaganNo ratings yet
- Developer Productivity-SPACE FrameworkDocument29 pagesDeveloper Productivity-SPACE FrameworkSrinivasan VenkatNo ratings yet
- Informed Consent Form For The Astrazeneca Covid-19 VaccineDocument1 pageInformed Consent Form For The Astrazeneca Covid-19 VaccineGodfrey Loth Sales Alcansare Jr.No ratings yet
- Hand Washing LessonDocument6 pagesHand Washing Lessonapi-278856455No ratings yet
- Photography NC Ii: Visual Arts SectorDocument71 pagesPhotography NC Ii: Visual Arts SectorPaul Omar PastranoNo ratings yet
- Emmanuel'S Resort: Samay, BalingasagDocument4 pagesEmmanuel'S Resort: Samay, BalingasagBryan LluismaNo ratings yet
- Kuliah ATLSDocument63 pagesKuliah ATLSDwianggriany Adhetia Piesca Widoretno100% (1)
- Miakatar17432825 Contemporary Teacher Leadership Report Assignment 1Document39 pagesMiakatar17432825 Contemporary Teacher Leadership Report Assignment 1api-408516682No ratings yet
- Test Health and DiseasesDocument4 pagesTest Health and DiseasesAndrea Anderson-HydeNo ratings yet
- Subjective: Short Term: Independent: Short TermDocument2 pagesSubjective: Short Term: Independent: Short TermCamille SesaldoNo ratings yet
- President Kaguta Museveni's Speech On Covid-19 As of 18 June 2021Document26 pagesPresident Kaguta Museveni's Speech On Covid-19 As of 18 June 2021The Campus TimesNo ratings yet
- Cerebro Lys inDocument18 pagesCerebro Lys inKathleen PalomariaNo ratings yet
- Dental Town 2016Document23 pagesDental Town 2016Tahir AliNo ratings yet