Download as pptx, pdf, or txt
You might also like
- Tureks Orthopaedics - Principles and Their ApplicDocument1 pageTureks Orthopaedics - Principles and Their Applicqu402113No ratings yet
- Hip ExaminationDocument84 pagesHip ExaminationDeepak Kumar100% (1)
- Bruce Ecker, Laurel Hulley - Depth Oriented Brief Therapy - How To Be Brief When You Were Trained To Be Deep and Vice Versa-Jossey-Bass (1995)Document306 pagesBruce Ecker, Laurel Hulley - Depth Oriented Brief Therapy - How To Be Brief When You Were Trained To Be Deep and Vice Versa-Jossey-Bass (1995)John Smith85% (13)
- Orthopedic VIVA Made Easy: November 2020Document15 pagesOrthopedic VIVA Made Easy: November 2020EmailNo ratings yet
- Pesticide Applicator Core ManualDocument206 pagesPesticide Applicator Core Manualdodsm100% (2)
- Spine TraumaDocument7 pagesSpine TraumafadlinNo ratings yet
- Orthopaedic Management in Cerebral Palsy, 2nd EditionFrom EverandOrthopaedic Management in Cerebral Palsy, 2nd EditionHelen Meeks HorstmannRating: 3 out of 5 stars3/5 (2)
- Free Preview - The Stall Slayer PDFDocument9 pagesFree Preview - The Stall Slayer PDFRohit RumadeNo ratings yet
- Dr. Sunil Kumar Sharma Senior Resident, Dept. of Neurology G.M.C., KOTADocument67 pagesDr. Sunil Kumar Sharma Senior Resident, Dept. of Neurology G.M.C., KOTAsuckeydluffyNo ratings yet
- Examination of SpineDocument54 pagesExamination of Spinenams ortho100% (1)
- Shoulder Joint AssessmentDocument92 pagesShoulder Joint Assessmentsonali tushamerNo ratings yet
- Spine Examination: Mario Johan Heryputra 11.2012.208Document29 pagesSpine Examination: Mario Johan Heryputra 11.2012.208Mario Johan Heryputra100% (1)
- IvdpDocument89 pagesIvdpFelix Sabu100% (1)
- The Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic AnatomyDocument50 pagesThe Leg: - Orthopedic Anatomy - Clinical Anatomy - Radiologic Anatomyspeedy.catNo ratings yet
- Examination of The Upper Cervical Spine PDFDocument22 pagesExamination of The Upper Cervical Spine PDFiikemNo ratings yet
- Examination of Cervical SpineDocument39 pagesExamination of Cervical SpinedrkanthikirangNo ratings yet
- Orthopaedics OsceDocument39 pagesOrthopaedics OsceLana Loco50% (2)
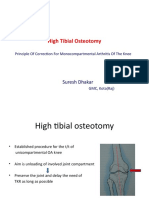
- High Tibial Osteotomy: Suresh DhakarDocument40 pagesHigh Tibial Osteotomy: Suresh DhakarAtul PandeyNo ratings yet
- Total Hip Replacement PPDocument22 pagesTotal Hip Replacement PPAnonymous dGfXuDd5No ratings yet
- A Case Report On Potts Spine Spinal TubeDocument3 pagesA Case Report On Potts Spine Spinal TubeyaneemayNo ratings yet
- Wrist and HandDocument3 pagesWrist and HandCherrie MaeNo ratings yet
- Interlocking NailingDocument211 pagesInterlocking NailingJulio EspinozaNo ratings yet
- Orthopaedic AnatomyDocument1 pageOrthopaedic Anatomyintan rosliNo ratings yet
- Computer Aided Diagnosis System For Lumbar Spinal Stenosis Using X-Ray ImagesDocument45 pagesComputer Aided Diagnosis System For Lumbar Spinal Stenosis Using X-Ray Imagesroky100% (1)
- Total Hip ReplacementDocument152 pagesTotal Hip Replacementminas100% (3)
- Thoracolumbar FracturesDocument29 pagesThoracolumbar FracturesFernaldi Anggadha100% (1)
- Examination of Hand & Common Hand InjuriesDocument165 pagesExamination of Hand & Common Hand InjuriesPriya GK100% (1)
- Varus Knee Classification and CorrectionDocument8 pagesVarus Knee Classification and CorrectionPraharshaNo ratings yet
- Ilizarov PresentationDocument50 pagesIlizarov PresentationSolomon Sekar100% (1)
- Knee ExaminationDocument54 pagesKnee ExaminationZed HarrisNo ratings yet
- DNB Orthopaedics Theory PapersDocument23 pagesDNB Orthopaedics Theory PapersmystraviNo ratings yet
- Spine Fracture and DislocationDocument74 pagesSpine Fracture and DislocationLydiaKainamaa100% (2)
- Spinal TraumaDocument81 pagesSpinal TraumaharilNo ratings yet
- Leg Ankle Orthopaedic Conditions FinalDocument26 pagesLeg Ankle Orthopaedic Conditions Finalangel bolfriNo ratings yet
- Soft Tissue Balance KneeDocument10 pagesSoft Tissue Balance KneeNitin BansalNo ratings yet
- Femoral Neck FracturesDocument8 pagesFemoral Neck FracturesMorshed Mahbub AbirNo ratings yet
- The Talonavicular and Subtalar Joints The Calcaneopedal Unit ConceptDocument11 pagesThe Talonavicular and Subtalar Joints The Calcaneopedal Unit ConceptAnonymous kdBDppigENo ratings yet
- Peripheral NerveDocument6 pagesPeripheral NerveNur Atiqah ZainalNo ratings yet
- Customers Who Viewed Also Viewed: Paperback - 10 December 2017Document4 pagesCustomers Who Viewed Also Viewed: Paperback - 10 December 2017Rajesh Itha100% (1)
- Management Tibial Plateau FractureDocument45 pagesManagement Tibial Plateau FracturePurushothama Rao NalamatiNo ratings yet
- CTEVDocument61 pagesCTEVSylvia LoongNo ratings yet
- Interventional Spine Procedures A Case-Based Approach PDFDocument215 pagesInterventional Spine Procedures A Case-Based Approach PDFdrhms2000100% (2)
- Orthopedic Imaging: A Practical Approach: Adam Greenspan 6th EditionDocument11 pagesOrthopedic Imaging: A Practical Approach: Adam Greenspan 6th EditionNovien WilindaNo ratings yet
- Surgical Approaches ElbowDocument68 pagesSurgical Approaches ElbowPrakash AyyaduraiNo ratings yet
- Principles of Tendon Transfer in The Hand and ForearmDocument9 pagesPrinciples of Tendon Transfer in The Hand and Forearm'Ema Surya PertiwiNo ratings yet
- Injuries of Wrist and HandDocument34 pagesInjuries of Wrist and HandMugunthan Rangiah100% (2)
- DNB Qs 10 Yrs PDFDocument65 pagesDNB Qs 10 Yrs PDFHaribabu ArumugamNo ratings yet
- Thesis TopicDocument5 pagesThesis TopicSrikant KonchadaNo ratings yet
- Ulnar Nerve PalsyDocument63 pagesUlnar Nerve PalsyArben Cenollari100% (1)
- Trauma & Orthopaedic SurgeryDocument120 pagesTrauma & Orthopaedic SurgeryOstazNo ratings yet
- Internal Derangement of Knee - 2Document113 pagesInternal Derangement of Knee - 2sushil2207No ratings yet
- Approach To FractureDocument17 pagesApproach To FractureRebecca WongNo ratings yet
- Orthopath Final ReviewDocument16 pagesOrthopath Final ReviewharrischoeNo ratings yet
- Shoulder DislocationDocument29 pagesShoulder DislocationAndaleeb ZehraNo ratings yet
- Metatarsalgia: Yakshita Chaube B.P.T Final YearDocument18 pagesMetatarsalgia: Yakshita Chaube B.P.T Final YearKapil LakhwaraNo ratings yet
- Flexor Tendon Injuries: DR Manoj Kumar OrtopaedicsDocument50 pagesFlexor Tendon Injuries: DR Manoj Kumar OrtopaedicsManoj Kumar100% (1)
- Compressive Neuropathy of Upper LimbDocument49 pagesCompressive Neuropathy of Upper LimbYamunaVaaneeSivalingamNo ratings yet
- Shoulder Exam - Shoulder & Elbow - OrthobulletsDocument8 pagesShoulder Exam - Shoulder & Elbow - Orthobulletsbrokenlimit5No ratings yet
- Ankle Fractures - A Logical Approach To Their FixationDocument48 pagesAnkle Fractures - A Logical Approach To Their FixationRoman MosneagaNo ratings yet
- Ankel Heel PainDocument51 pagesAnkel Heel PainMeno Ali100% (1)
- Elbow WristDocument59 pagesElbow Wristdr_asalehNo ratings yet
- Orthopedics Oath C1 Mini-OSCEDocument5 pagesOrthopedics Oath C1 Mini-OSCEHajar AlajlouniNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Declaration Form - Work From Home Attachment 2Document1 pageDeclaration Form - Work From Home Attachment 2BAGUIO CATSNo ratings yet
- Rose Doe v. The City of New York, Et. Al.Document57 pagesRose Doe v. The City of New York, Et. Al.Daily Caller News FoundationNo ratings yet
- L. Gifford The Mature Organism ModelDocument12 pagesL. Gifford The Mature Organism ModelRoar SyltebøNo ratings yet
- Analisis Penerapan Metode Activity Based Costing (ABC) Dalam Menentukan Tarif Jasa Rawat Inap Di RSUD Kota PrabumulihDocument12 pagesAnalisis Penerapan Metode Activity Based Costing (ABC) Dalam Menentukan Tarif Jasa Rawat Inap Di RSUD Kota PrabumulihAffira AfriNo ratings yet
- Child Rights and You - Wikipedia PDFDocument14 pagesChild Rights and You - Wikipedia PDFpatel mariyamNo ratings yet
- BHS InggrisDocument5 pagesBHS InggrisDeajeng Febby AyuNo ratings yet
- Language Disorders - 5Document27 pagesLanguage Disorders - 5Marta Sampedro GonzalezNo ratings yet
- Development of Push-Pull Osmotic Pump Tablets For A SlightlyDocument4 pagesDevelopment of Push-Pull Osmotic Pump Tablets For A SlightlyphamuyenthuNo ratings yet
- 16012019FV4Q6RWBAnnexure documentofEIAEMP PDFDocument400 pages16012019FV4Q6RWBAnnexure documentofEIAEMP PDFJainam Shah100% (1)
- Hope - 1 Grade 11: Exercise For FitnessDocument6 pagesHope - 1 Grade 11: Exercise For FitnessTABBAL JAN PAOLONo ratings yet
- WEEK 2: 12A, 12B, 12G Ôn Tập Khảo Sát Pronunciation ClosestDocument6 pagesWEEK 2: 12A, 12B, 12G Ôn Tập Khảo Sát Pronunciation ClosestHàNhậtNguyễnNo ratings yet
- Illuminating The Aura of Nostalgia: Perceptions of Time, Place, and Identity (ANASTASIA PLATOFF)Document33 pagesIlluminating The Aura of Nostalgia: Perceptions of Time, Place, and Identity (ANASTASIA PLATOFF)Anastasia PlatoffNo ratings yet
- Your AnswersDocument5 pagesYour AnswersHa TranNo ratings yet
- Zoom For Healthcare: One Platform For Virtual Care & CommunicationDocument2 pagesZoom For Healthcare: One Platform For Virtual Care & CommunicationDespacho virtualNo ratings yet
- A New Growth Strategy For Developing NationsDocument16 pagesA New Growth Strategy For Developing NationsmumoshitakeshiNo ratings yet
- ANALISIS PENERAPAN SISTEM LOCKOUTTAGOUT (LOTO) PADA BAGIAN OPERASI DAN PEMELIHARAAN DI PT. X TANJUNG EMAS KOTA SEMARANG (Berdasarkan Standar OSHA 29 CFR Part 1910.147 Dan Part 1910.333) PDFDocument11 pagesANALISIS PENERAPAN SISTEM LOCKOUTTAGOUT (LOTO) PADA BAGIAN OPERASI DAN PEMELIHARAAN DI PT. X TANJUNG EMAS KOTA SEMARANG (Berdasarkan Standar OSHA 29 CFR Part 1910.147 Dan Part 1910.333) PDFAfif Fayadh VictoryNo ratings yet
- MCQ in OphthalmologyDocument108 pagesMCQ in OphthalmologySushi HtetNo ratings yet
- HypothermiaDocument5 pagesHypothermiaMRS CHAKRAPANINo ratings yet
- Local Exhaust Ventilation LEV Guidance PDFDocument72 pagesLocal Exhaust Ventilation LEV Guidance PDFJoaquim Reis100% (2)
- Creating A Geriatric Emergency Department John Schumacher Full Chapter PDFDocument69 pagesCreating A Geriatric Emergency Department John Schumacher Full Chapter PDFmourdegoma100% (5)
- Adolescence and Preg Position PaperDocument2 pagesAdolescence and Preg Position PaperNichole Trisha MontalbaNo ratings yet
- Kiran Raju - Techversant PayslipDocument3 pagesKiran Raju - Techversant PayslipCap RJNo ratings yet
- Celebrating Worthing College 2012 SpeadsDocument9 pagesCelebrating Worthing College 2012 SpeadsWorthing College-SportNo ratings yet
- Hormones ImbalanceDocument3 pagesHormones ImbalanceKiran KhanNo ratings yet
- Ayurvedic Medicine For Bhutansha RasaDocument6 pagesAyurvedic Medicine For Bhutansha RasaKolluri RajeshNo ratings yet
- Knowledge ManagementDocument63 pagesKnowledge Managementrahul-singh-6592No ratings yet
- Substance AbuseDocument54 pagesSubstance AbuseCharles CastilloNo ratings yet