Download as pptx, pdf, or txt
You might also like
- EKG Clep TestDocument13 pagesEKG Clep TestElissa LafondNo ratings yet
- ACLS Study Guide NewDocument35 pagesACLS Study Guide NewNIRANJANA SHALINI100% (1)
- EKG WorkbookDocument22 pagesEKG WorkbookZiac Lortab100% (1)
- Adult Advanced Life Support2Document34 pagesAdult Advanced Life Support2drDilanNo ratings yet
- Resuscitation Council (UK)Document18 pagesResuscitation Council (UK)Abdelfattah RashwanNo ratings yet
- BCLS 2Document73 pagesBCLS 2Praveen Ravishankaran100% (1)
- Advanced Life Support AlgorithmDocument34 pagesAdvanced Life Support AlgorithmmariamNo ratings yet
- 3.ALS Algorithms Advanced Life SupportDocument1 page3.ALS Algorithms Advanced Life SupportLucian Alin DinuNo ratings yet
- Cardiorespiratory Arrest (FS)Document88 pagesCardiorespiratory Arrest (FS)haerul ikhsanNo ratings yet
- Dvanced Cardiac Life SupportDocument72 pagesDvanced Cardiac Life Supportolivia100% (1)
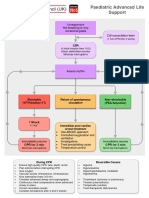
- Paediatric Advanced Life Support: Call For Help 2222 Commence/continue CPR (5 Initial Breaths Then CV Ratio 15:2)Document1 pagePaediatric Advanced Life Support: Call For Help 2222 Commence/continue CPR (5 Initial Breaths Then CV Ratio 15:2)Vijay RNo ratings yet
- Advanced Cardiac Life SupportDocument68 pagesAdvanced Cardiac Life SupportKim Halipa-Que LaurenteNo ratings yet
- BLS and ACLS SurveysDocument29 pagesBLS and ACLS SurveysMosab AfanahNo ratings yet
- 3 Combined AHA BLS ACLS Updates CombinedDocument5 pages3 Combined AHA BLS ACLS Updates Combinedamanrup randhawa100% (1)
- ACLS - Guidelines From 2005USADocument62 pagesACLS - Guidelines From 2005USAsbontchevNo ratings yet
- Adult Advanced Life SupportDocument23 pagesAdult Advanced Life SupportbigpriapNo ratings yet
- Cardiorespiratory Arrest (FS)Document55 pagesCardiorespiratory Arrest (FS)Ahmad AzharNo ratings yet
- Advanced Cardiac Life SupportDocument8 pagesAdvanced Cardiac Life Supportcool kipsNo ratings yet
- A (ACLS) - 2015: Dvanced Cardiac Life SupportDocument52 pagesA (ACLS) - 2015: Dvanced Cardiac Life SupportNajmussaqibNo ratings yet
- ACLSDocument275 pagesACLSShajahan SideequeNo ratings yet
- PalsalgoDocument1 pagePalsalgozacklim_2000No ratings yet
- Perkembangan Baru Resusitasi Jantung ParuDocument27 pagesPerkembangan Baru Resusitasi Jantung ParuMarcelina Aprisia PrimadiNo ratings yet
- Immediate Life SupportDocument63 pagesImmediate Life Supportmatrixkhalifa9955No ratings yet
- Cardiopulmonary ResuscitationDocument29 pagesCardiopulmonary ResuscitationSarahNo ratings yet
- Adult Advanced Life Support Algorithm 2021 Aug 2023Document1 pageAdult Advanced Life Support Algorithm 2021 Aug 2023cknihilnewNo ratings yet
- Bls & Acls & DC ShockDocument70 pagesBls & Acls & DC Shockpop lopNo ratings yet
- Basic Life Support (BLS) and Advanced Cardiovascular Life Support (ACLS)Document35 pagesBasic Life Support (BLS) and Advanced Cardiovascular Life Support (ACLS)rajNo ratings yet
- C P R -د باسمDocument15 pagesC P R -د باسمrahaf.almomaniNo ratings yet
- Cardiac Arrest PDFDocument4 pagesCardiac Arrest PDFYogi drNo ratings yet
- Cardiac Arrest Advanced Life Support PDFDocument1 pageCardiac Arrest Advanced Life Support PDFCristina TrofimovNo ratings yet
- Cardiac Arrest Advanced Life SupportDocument1 pageCardiac Arrest Advanced Life SupportCristina TrofimovNo ratings yet
- Paediatric ALS A3Document1 pagePaediatric ALS A3Ali HusseinNo ratings yet
- Advanced Cardiac Life Support (ACLS)Document17 pagesAdvanced Cardiac Life Support (ACLS)Siti Rahima HarahapNo ratings yet
- 8-Adult Advanced Life Support Algorithm 2021Document1 page8-Adult Advanced Life Support Algorithm 2021khaledNo ratings yet
- DC Shock + AritmiaDocument34 pagesDC Shock + AritmiaSuparno Adi SantikaNo ratings yet
- ACLS Book (New)Document23 pagesACLS Book (New)Essa AyazNo ratings yet
- Poster 10 PALS 01 01 ENG V20100927 PDFDocument1 pagePoster 10 PALS 01 01 ENG V20100927 PDFAndy XiaoNo ratings yet
- AHA 2010 - 2015 Guidlines For CPR by Dody FirmandaDocument34 pagesAHA 2010 - 2015 Guidlines For CPR by Dody FirmandaismihabNo ratings yet
- Paediatric Advanced Life Support: Resuscitation Council (UK)Document12 pagesPaediatric Advanced Life Support: Resuscitation Council (UK)zacklim_2000100% (1)
- ACLS Simplify AlgorithmDocument6 pagesACLS Simplify AlgorithmKristine Monforte Coma UritaNo ratings yet
- 2005 ACLS Guidelines 5.15Document11 pages2005 ACLS Guidelines 5.15gr8_nurseNo ratings yet
- Cardiorespiratory ArrestDocument51 pagesCardiorespiratory ArrestIrham KhairiNo ratings yet
- PalsDocument1 pagePalslordroentgenNo ratings yet
- Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDocument64 pagesDepartemen Kardiologi FK USU RSUP. H. Adam Malik MedanBonitavanyNo ratings yet
- ECG WorksheetDocument4 pagesECG WorksheetNikki GuisonNo ratings yet
- Pulseless Ventricular Tachycardia/Ventricular Fibrillation Algorithm (Figure 8-5)Document1 pagePulseless Ventricular Tachycardia/Ventricular Fibrillation Algorithm (Figure 8-5)Maya AritonangNo ratings yet
- Cardio ACLS PDFDocument9 pagesCardio ACLS PDFfrankies fpNo ratings yet
- Advanced Cardiac Life SupportDocument28 pagesAdvanced Cardiac Life SupportAbdulrahman AlsayyedNo ratings yet
- ACLS Algorithms (2011)Document6 pagesACLS Algorithms (2011)senbonsakuraNo ratings yet
- AlsalgoDocument1 pageAlsalgozacklim_2000No ratings yet
- Alsalgo PDFDocument1 pageAlsalgo PDFDelvanny Alfikri Rekaputri WicaksonoNo ratings yet
- Advanced Cardiac Life SupportDocument37 pagesAdvanced Cardiac Life SupportRoy Acosta GumbanNo ratings yet
- BLS and Advance Cardiac Life SupportDocument135 pagesBLS and Advance Cardiac Life SupportSteffiNo ratings yet
- Code Blue ManagemnetDocument36 pagesCode Blue ManagemnetPreethi BNo ratings yet
- ACLS TeoriDocument27 pagesACLS TeoriTita Luthfia100% (1)
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- A Simple Guide to Hand Tremors, Related Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to Hand Tremors, Related Diseases and Use in Disease DiagnosisRating: 3.5 out of 5 stars3.5/5 (3)
- Physiology of Excitatory and Conducting System of Heart by Dr. Mudassar Ali RoomiDocument17 pagesPhysiology of Excitatory and Conducting System of Heart by Dr. Mudassar Ali RoomiMudassar Roomi100% (3)
- Electrical Conduction System of The HeartDocument1 pageElectrical Conduction System of The HeartRyl WonNo ratings yet
- Aclsrhythmtest11 PDFDocument7 pagesAclsrhythmtest11 PDFmonir610% (1)
- Chest Pain: Caitlin Everson (Clinical Fellow AED)Document194 pagesChest Pain: Caitlin Everson (Clinical Fellow AED)lisserranoNo ratings yet
- Perianesthetic ArrhythmiasDocument10 pagesPerianesthetic Arrhythmiastaner_soysurenNo ratings yet
- ArrhythmiaDocument55 pagesArrhythmiaDonjeta AbaziNo ratings yet
- Diagnosis and Management of AFDocument135 pagesDiagnosis and Management of AFMatthew ChristopherNo ratings yet
- Antiarrhythmic Drugs - AMBOSS TWODocument6 pagesAntiarrhythmic Drugs - AMBOSS TWOOpio IsaacNo ratings yet
- Cavotricuspid Isthmus: Anatomy, Electrophysiology, and Long-Term OutcomeDocument5 pagesCavotricuspid Isthmus: Anatomy, Electrophysiology, and Long-Term Outcomeapi-26166949No ratings yet
- 24hr ECG InterpretationDocument26 pages24hr ECG InterpretationMariaNo ratings yet
- Pace MakerDocument9 pagesPace MakerTridib RNo ratings yet
- Palpitations AND Heartbeat Disorders: By: Aisha Sara Tasnim Physician: DR SsebulibaDocument22 pagesPalpitations AND Heartbeat Disorders: By: Aisha Sara Tasnim Physician: DR SsebulibaNinaNo ratings yet
- Basic ECG InterpretationDocument62 pagesBasic ECG Interpretationmohannadalkwiese3No ratings yet
- Catalogo Fluke Biomedical 2019Document37 pagesCatalogo Fluke Biomedical 2019Fabricio AlmeidaNo ratings yet
- Procedure For DefibrillationDocument6 pagesProcedure For DefibrillationTasia DeastutiNo ratings yet
- Basic Life Support and Advanced Cardiovascular Life SupportDocument90 pagesBasic Life Support and Advanced Cardiovascular Life SupportRakhshanda khan100% (1)
- Rhythm EKG Rate (BPM) Rhythm EKG InterventionsDocument6 pagesRhythm EKG Rate (BPM) Rhythm EKG InterventionsRawabi rawabi1997No ratings yet
- ECG - ACLS 2020 ModuleDocument68 pagesECG - ACLS 2020 ModuleRasheedAladdinNGuiomala100% (1)
- ArrhythmiasDocument57 pagesArrhythmiasAmra ahmedNo ratings yet
- Miniaturized Reveal LINQ Insertable Cardiac MonitoDocument7 pagesMiniaturized Reveal LINQ Insertable Cardiac MonitoLetícia JanuziNo ratings yet
- Modified by Dr. Salah H Sinjary College of Medicine HMU Department of Medicine 07504454134Document47 pagesModified by Dr. Salah H Sinjary College of Medicine HMU Department of Medicine 07504454134Chro MANo ratings yet
- Final AnnouncementDocument19 pagesFinal AnnouncementDea PrazwalithaNo ratings yet
- Bifascicular Block Revealing Steinerts Myotonic DystrophyDocument8 pagesBifascicular Block Revealing Steinerts Myotonic DystrophyIJAR JOURNALNo ratings yet
- Exam Bioelectricity TUDeft 10april2015 - AnswersDocument12 pagesExam Bioelectricity TUDeft 10april2015 - AnswersJan MatyášNo ratings yet
- Pan Tompkins AlgorithmDocument6 pagesPan Tompkins AlgorithmSwarubini PJNo ratings yet
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- Slide Master Apm CPR N AedDocument46 pagesSlide Master Apm CPR N AedDivyaaNo ratings yet
- Lange Smart Charts: Pharmacology, 2e Medications Affecting Cardiac and Renal FunctionDocument2 pagesLange Smart Charts: Pharmacology, 2e Medications Affecting Cardiac and Renal FunctionSaulNo ratings yet