Download as ppt, pdf, or txt
You might also like
- IES Test Prep Answer Explanations For SAT GrammarDocument72 pagesIES Test Prep Answer Explanations For SAT GrammarĐ̸̢͓͉̣͔̭̜̭͉̰́͌͑͊̇̏̕̚͜͜ͅứ̷̢̛̘̭̤͎̩̣̩̊̆̑̓̽̓͗ͅc̴̟͈̠̤̪͈͍̰̟̤̮̆̄̈́̈̃̏̃̑̊͠͝ä̷̧̰̲̦́̒̐͝ṉ̵̾̀͗̾h̷̥͆͑̍͌͆̋̈́́͒͂̇͘̚ Đ̸̢͓͉̣͔̭̜̭͉̰́͌͑͊̇̏̕̚͜͜ͅứ̷̢̛̘̭̤͎̩̣̩̊̆̑̓̽̓͗ͅc̴̟͈̠̤̪͈͍̰̟̤̮̆̄̈́̈̃̏̃̑̊͠͝ä̷̧̰̲̦́̒̐͝ṉ̵̾̀͗̾h̷̥͆͑̍͌͆̋̈́́͒͂̇͘75% (4)
- ENACb 1Document166 pagesENACb 1DarrylpnzNo ratings yet
- Extention PDF Cath Lab TechDocument2 pagesExtention PDF Cath Lab TechChrisNo ratings yet
- Tutorial Chapter 1 - 0 ThermodynamicDocument2 pagesTutorial Chapter 1 - 0 ThermodynamicSufferedMuchNo ratings yet
- AnastesiDocument22 pagesAnastesidhitadwynNo ratings yet
- AHA Vs ERC GuidelinesDocument39 pagesAHA Vs ERC GuidelinesYoel Harianto100% (2)
- Use of Anticoagulants During Pregnancy and PostpartumDocument26 pagesUse of Anticoagulants During Pregnancy and PostpartumAdi SabarwalNo ratings yet
- Richards JE, Damage Control Resuscitation in Traumatic Hemorrhage, It Is More Than, Anesthesiol 2023Document13 pagesRichards JE, Damage Control Resuscitation in Traumatic Hemorrhage, It Is More Than, Anesthesiol 2023jorge fabregatNo ratings yet
- Difficult Airway AlgorithmDocument48 pagesDifficult Airway AlgorithmshikhaNo ratings yet
- Bullous Lung DiseaseDocument25 pagesBullous Lung DiseaseAmenhotep89100% (1)
- Konas Perdatin 2019Document66 pagesKonas Perdatin 2019Akreditasi RSPC19No ratings yet
- Resusitasi NeonatusDocument22 pagesResusitasi NeonatusnikkitaihsanNo ratings yet
- 183 Difficult Airway Management (Gabungan)Document135 pages183 Difficult Airway Management (Gabungan)lathifa_nurNo ratings yet
- 029 Reddy PDFDocument59 pages029 Reddy PDFKonas Xi PalembangNo ratings yet
- Anesthesia For Plastic Surgery ProceduresDocument35 pagesAnesthesia For Plastic Surgery ProceduresSergio ArbelaezNo ratings yet
- Shock On TraumaDocument36 pagesShock On TraumaMeviraf BennyNo ratings yet
- Surviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedDocument32 pagesSurviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedAdli Wafi Jabbar100% (1)
- Thoracic Segmental Spinal Anaesthesia/ General Anaesthesia For Laproscopy SurgeryDocument8 pagesThoracic Segmental Spinal Anaesthesia/ General Anaesthesia For Laproscopy SurgeryIJAR JOURNALNo ratings yet
- Tehnik - Tehnik Analgesia Post OperasiDocument32 pagesTehnik - Tehnik Analgesia Post OperasiGuntur Aryo PuntodewoNo ratings yet
- OK - Modul Ortho - Bone Cement Implantation SyndromeDocument18 pagesOK - Modul Ortho - Bone Cement Implantation SyndromeWanditoGayuhUtomoNo ratings yet
- 02 Patient Safety Bedah Anestesiologi WEBINARDocument73 pages02 Patient Safety Bedah Anestesiologi WEBINARSiti AisyahNo ratings yet
- Monitoring PerioperatipDocument54 pagesMonitoring Perioperatipjavajavu100% (1)
- Journal Reading AminophyllineDocument76 pagesJournal Reading AminophyllinePandhu Suprobo100% (1)
- ShockDocument39 pagesShockCut Ristina OlviaNo ratings yet
- AnestesiDocument11 pagesAnestesiAnonymous 8w9QEGNo ratings yet
- Pre-Op Preparation and Assessment of Pediatric PatientsDocument62 pagesPre-Op Preparation and Assessment of Pediatric PatientsBedahanakugmNo ratings yet
- Anaesthesia For The Obese PatientDocument8 pagesAnaesthesia For The Obese Patientstephanus henryNo ratings yet
- PDF Heart FailureDocument30 pagesPDF Heart FailureNitya Manggala JayaNo ratings yet
- Critical Appraisal Worksheet TherapyDocument2 pagesCritical Appraisal Worksheet TherapyiwakiwakNo ratings yet
- Sepsis 2018Document9 pagesSepsis 2018Gianfranco Tovar Calderón100% (1)
- Prediction Difficult AirwayDocument6 pagesPrediction Difficult AirwayParvathy R NairNo ratings yet
- Anesthesia For Tracheoesophageal Fistula RepairDocument29 pagesAnesthesia For Tracheoesophageal Fistula RepairArop AkechNo ratings yet
- Primary SurveyDocument25 pagesPrimary Surveyapi-98304344No ratings yet
- Gerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistDocument51 pagesGerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistChristian Clyde N. ApigoNo ratings yet
- LaryngospasmDocument5 pagesLaryngospasmnunikdwijatiNo ratings yet
- Anaesthesia For Awake Craniotomy A Modern ApproachDocument4 pagesAnaesthesia For Awake Craniotomy A Modern ApproachPablo Sousa CasasnovasNo ratings yet
- Pediatric AnesthesiaDocument70 pagesPediatric AnesthesiaEliyan KhanimovNo ratings yet
- Anesthesia For Transsphenoidal Pituitary Surgery.Document6 pagesAnesthesia For Transsphenoidal Pituitary Surgery.ismaelNo ratings yet
- Malaysiantriagescalenewrevised2019!1!221014090642 28d8e1aeDocument18 pagesMalaysiantriagescalenewrevised2019!1!221014090642 28d8e1aenaqibsakila4286No ratings yet
- PVC Stoelting Coex 1Document29 pagesPVC Stoelting Coex 1Rudy SiahaanNo ratings yet
- Endometrial Cancer: Nancy Wozniak, MDDocument33 pagesEndometrial Cancer: Nancy Wozniak, MDHervis Fantini100% (1)
- Antiarrhythmic Drugs - Classification and Mechanism of Action.Document1 pageAntiarrhythmic Drugs - Classification and Mechanism of Action.SUMIT KUMAR DASNo ratings yet
- Anaesthesia For NephrectomyDocument4 pagesAnaesthesia For Nephrectomy43gasdemNo ratings yet
- Aspirin in The Primary Prevention of Cardiovascular Disease and CancerDocument16 pagesAspirin in The Primary Prevention of Cardiovascular Disease and CancerCARLOSNo ratings yet
- Booklet Bcu Revisi 5Document8 pagesBooklet Bcu Revisi 5irza nasutionNo ratings yet
- ANESTHESIA in OBSTETRICSDocument159 pagesANESTHESIA in OBSTETRICSemma rose lutellaNo ratings yet
- CASP Checklist: Case Control Study How To Use This Appraisal ToolDocument6 pagesCASP Checklist: Case Control Study How To Use This Appraisal Toolanon_770867052No ratings yet
- Perbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterDocument7 pagesPerbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterAfiani JannahNo ratings yet
- JCCA Is Back-ICU Without Wall 2022 OkDocument23 pagesJCCA Is Back-ICU Without Wall 2022 OkJolatuvelBahanaNo ratings yet
- Perioperative Management of Asthma in Cesarean SectionDocument29 pagesPerioperative Management of Asthma in Cesarean Sectionhouman726254085No ratings yet
- Biodata Parestesi Juli 2011 Edit Ipo ++Document55 pagesBiodata Parestesi Juli 2011 Edit Ipo ++rahmat feryadi0% (1)
- Turp 160328193838Document36 pagesTurp 160328193838Right VentricleNo ratings yet
- Acute Limb IschaemiaDocument32 pagesAcute Limb IschaemiaAnonymous 9wHscM100% (1)
- Complicated AppendicitisDocument4 pagesComplicated AppendicitisMedardo ApoloNo ratings yet
- Management of Post-Operative Nausea and Vomiting in Adults - The Pharmaceutical JournalDocument18 pagesManagement of Post-Operative Nausea and Vomiting in Adults - The Pharmaceutical JournalResti DwiuNo ratings yet
- Pitfalls in Anesthesia MonitoringDocument56 pagesPitfalls in Anesthesia MonitoringDr.Sandeep Kumar Kar100% (1)
- DIVITI Slide Prophylaxis VTE SPPD Ringkas-1Document11 pagesDIVITI Slide Prophylaxis VTE SPPD Ringkas-1Fera NurrizaNo ratings yet
- Aidaa ExtubationDocument7 pagesAidaa ExtubationebmkrNo ratings yet
- Pocketbookofobstetricneonatalnpediatricemergencies PDFDocument378 pagesPocketbookofobstetricneonatalnpediatricemergencies PDFDANANo ratings yet
- Catatan DSTC CourseDocument3 pagesCatatan DSTC CourseHanny FadhilaNo ratings yet
- Pain Medicine Board Review 1st EditionDocument52 pagesPain Medicine Board Review 1st Editionkevin.smart540No ratings yet
- Speech Patterns: Christine Martin - Steph Estavillo - Melanie PadillaDocument24 pagesSpeech Patterns: Christine Martin - Steph Estavillo - Melanie PadillaChristineMartinNo ratings yet
- Catalogo ColonneDocument140 pagesCatalogo Colonneapi-18378576No ratings yet
- Coal Ash Dewatering SolutionDocument23 pagesCoal Ash Dewatering Solution류태하No ratings yet
- Biology Investigatory Project: Malaria: Its Effects and CausesDocument17 pagesBiology Investigatory Project: Malaria: Its Effects and CausesRishi KeshavNo ratings yet
- Background of Philippine Art and Literature in Romantic RealismDocument2 pagesBackground of Philippine Art and Literature in Romantic RealismRaldz CoyocaNo ratings yet
- CSC 2701 - CalculusDocument5 pagesCSC 2701 - CalculusMd Rubaiyat BhuiyanNo ratings yet
- Md. Rizwanur Rahman - CVDocument4 pagesMd. Rizwanur Rahman - CVHimelNo ratings yet
- Relative Color Pickup of Three Different Knits and Predictive Dyeing Recipe FormulationDocument17 pagesRelative Color Pickup of Three Different Knits and Predictive Dyeing Recipe FormulationNguyễn Huy CườngNo ratings yet
- Bigbang PDFDocument772 pagesBigbang PDFLeanne Haddock100% (1)
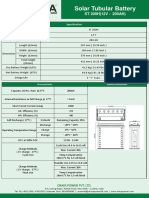
- ST200HDocument2 pagesST200HAnjana DissanayakaNo ratings yet
- هاشم عدي حاتم سيارات ثاني التجربة الثانيهDocument6 pagesهاشم عدي حاتم سيارات ثاني التجربة الثانيههاشم عديNo ratings yet
- 5 25 17 Migraines PowerPointDocument40 pages5 25 17 Migraines PowerPointSaifi AlamNo ratings yet
- Gear Trains: 8.1. Angular Velocity RatioDocument16 pagesGear Trains: 8.1. Angular Velocity RatioaddisudagneNo ratings yet
- An Overview of Discourse AnalysisDocument26 pagesAn Overview of Discourse Analysisjamogi2943No ratings yet
- MGje 6 Fix GX PK Yp RBJ LBRDocument9 pagesMGje 6 Fix GX PK Yp RBJ LBRBANOTH KUMARNo ratings yet
- Sewing Skills Checklist PDFDocument44 pagesSewing Skills Checklist PDFyemkem100% (1)
- Process SequenceDocument2 pagesProcess SequenceUmesh SakhareliyaNo ratings yet
- Lecture 4Document24 pagesLecture 4Geeta AroraNo ratings yet
- Law of Mother Earth BoliviaDocument3 pagesLaw of Mother Earth Boliviarahul banerjeeNo ratings yet
- HDR10+ System Whitepaper: September 4, 2019 HDR10+ Technologies, LLCDocument14 pagesHDR10+ System Whitepaper: September 4, 2019 HDR10+ Technologies, LLCDragomir ConstantinNo ratings yet
- Perdev Module 3Document13 pagesPerdev Module 3Renelyn JacoNo ratings yet
- EQUILIBRIUMDocument1 pageEQUILIBRIUMMohammed IliasNo ratings yet
- Sri Lank An Airline IndustryDocument29 pagesSri Lank An Airline IndustryTuan RifkhanNo ratings yet
- Jack and The Beanstalk Treatment-2Document10 pagesJack and The Beanstalk Treatment-2api-668257195No ratings yet
- En Mongolia 06Document39 pagesEn Mongolia 06Sandeep DasNo ratings yet
- TinyMobileRobots TinySurveyor FlyerDocument4 pagesTinyMobileRobots TinySurveyor FlyerfelipeNo ratings yet