
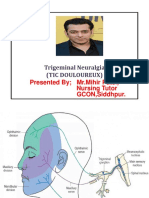
Trigeminal Neuralgia
Trigeminal Neuralgia
You might also like
- Cranial Nerve AssessmentDocument42 pagesCranial Nerve AssessmentValeryn Quiman100% (8)
- Oral Cancer 26.3.19Document23 pagesOral Cancer 26.3.19Pradeep100% (2)
- DACRYOCYSTITISDocument34 pagesDACRYOCYSTITISAriyanie Nurtania100% (1)
- Diseases of Oral CavityDocument60 pagesDiseases of Oral Cavityfredrick damian80% (5)
- Introduction To Agada Tantra, Visha & It's Classification, Properties & Action of Visha, Diagnosis of Poisoning, Treatment of PoisoningDocument123 pagesIntroduction To Agada Tantra, Visha & It's Classification, Properties & Action of Visha, Diagnosis of Poisoning, Treatment of PoisoningAbiskar Adhikari100% (14)
- Trigeminal NeuralgiaDocument15 pagesTrigeminal NeuralgiaMihir Patel75% (4)
- Anatomy of The Facial NerveDocument75 pagesAnatomy of The Facial NerveRao Rizwan Shakoor67% (3)
- Sialogogue and Anti-SialogogueDocument20 pagesSialogogue and Anti-SialogogueFoysal Sirazee60% (10)
- Sterisol Instructions For UseDocument10 pagesSterisol Instructions For UseJoe Shewale100% (1)
- CONJUNCTIVITISDocument67 pagesCONJUNCTIVITISNauli Panjaitan86% (7)
- Dandy WalkerDocument12 pagesDandy WalkerzarithNo ratings yet
- Trigeminal Neuralgia Oral SurgeryDocument48 pagesTrigeminal Neuralgia Oral SurgeryFourthMolar.com67% (3)
- Trigeminal NeuralgiaDocument3 pagesTrigeminal NeuralgiaAira Alaro50% (2)
- SyncopeDocument28 pagesSyncopeDurgesh PushkarNo ratings yet
- Sialogogue and Anti SialogogueDocument6 pagesSialogogue and Anti SialogoguePutri Farahmida50% (2)
- Bell's PalsyDocument20 pagesBell's PalsyVishesh JainNo ratings yet
- OsteomyelitisDocument21 pagesOsteomyelitisSurgeonZak50% (2)
- Sialogogues & Anti SailogoguesDocument43 pagesSialogogues & Anti SailogoguesTavleen KaurNo ratings yet
- Anaphylactic Shock LectureDocument32 pagesAnaphylactic Shock LectureIchal 'petta' Malebbi100% (1)
- Trigeminal Neuralgia and Its ManagementDocument79 pagesTrigeminal Neuralgia and Its ManagementRohit SharmaNo ratings yet
- Bell' Palsy - PPT Report - PPT FINALDocument21 pagesBell' Palsy - PPT Report - PPT FINALCarshena Cuares100% (1)
- Raynaud's Disease - JERAIZADocument23 pagesRaynaud's Disease - JERAIZAmaU439No ratings yet
- StomatitisDocument44 pagesStomatitisNessa Layos Morillo100% (1)
- Head InjuryDocument31 pagesHead InjuryZawawi Ibnu Rosyid0% (1)
- Eye Banking OphthalmologyDocument21 pagesEye Banking Ophthalmologyvivekrajbhilai5850100% (2)
- Vertebrobasilar Insufficiency/Syndrome: Hitesh Rohit (3 Year BPT)Document14 pagesVertebrobasilar Insufficiency/Syndrome: Hitesh Rohit (3 Year BPT)Hitesh N RohitNo ratings yet
- Balanced Diet: Bhavya Mds I Year Department of Conservative Dentistry & EndodonticsDocument76 pagesBalanced Diet: Bhavya Mds I Year Department of Conservative Dentistry & EndodonticsMayank AggarwalNo ratings yet
- By: Sarika Yadav Asst. LecturerDocument49 pagesBy: Sarika Yadav Asst. LecturerSarika YadavNo ratings yet
- TMJ DislocationDocument56 pagesTMJ DislocationAlok BhardwajNo ratings yet
- Meniere DiseaseDocument16 pagesMeniere DiseaseNavjot Brar100% (2)
- Chronic Otitis Media Types, Investigations, TreatmentDocument43 pagesChronic Otitis Media Types, Investigations, TreatmentPrasanna DattaNo ratings yet
- Cysts of Oral CavityDocument112 pagesCysts of Oral CavityMukhallat Qazi100% (1)
- Ameloblastoma: Submitted byDocument9 pagesAmeloblastoma: Submitted byJana AliNo ratings yet
- Local AnesthesiaDocument121 pagesLocal AnesthesiaGabriela Cocieru Motelica100% (2)
- Pathophysiology of Pain and Pain Assessment PDFDocument12 pagesPathophysiology of Pain and Pain Assessment PDFRaisa AriesthaNo ratings yet
- Facial NerveDocument80 pagesFacial Nerverasagna reddyNo ratings yet
- Pemphigus vulgarisPPTDocument23 pagesPemphigus vulgarisPPTSiti HanisaNo ratings yet
- The EarDocument59 pagesThe EarJasmin Jacob100% (5)
- Carcinoma TongueDocument39 pagesCarcinoma TongueVijay Krishna Murthy33% (3)
- Deep Bite 6Document97 pagesDeep Bite 6Manjunath Bellary100% (2)
- Congestive Heart Failure PDFDocument49 pagesCongestive Heart Failure PDFVerinice NañascaNo ratings yet
- OsteomyelitisDocument47 pagesOsteomyelitisArmand Al HaraaniNo ratings yet
- SHASTIUPAKRAMAIJAARDocument10 pagesSHASTIUPAKRAMAIJAARRavi SharmaNo ratings yet
- Lichen Planus: DR Hira BashirDocument37 pagesLichen Planus: DR Hira BashirSaroash SadruddinNo ratings yet
- GINGIVITISDocument43 pagesGINGIVITISRamyaNo ratings yet
- Question Papers For Bds Second YearDocument6 pagesQuestion Papers For Bds Second Yearsridevi sivaramakrishnanNo ratings yet
- Anchorage in OrthodonticsDocument103 pagesAnchorage in OrthodonticsEmad Ahmad Anis100% (2)
- NSAIDsDocument12 pagesNSAIDsjelly100% (1)
- Routes of Drug AdministrationDocument42 pagesRoutes of Drug AdministrationKandarp PatelNo ratings yet
- Oral Pathology - Physical & Chemical Injuries of Oral CavityDocument44 pagesOral Pathology - Physical & Chemical Injuries of Oral CavityRachit Srivastava83% (18)
- ENCEPHALITISDocument37 pagesENCEPHALITISNida NaazNo ratings yet
- Preanesthetic Medication PDFDocument5 pagesPreanesthetic Medication PDFSayan NagNo ratings yet
- Eye ExaminationDocument23 pagesEye Examinationcynthia167No ratings yet
- Healing of Oral WoundsDocument73 pagesHealing of Oral WoundsMadhvendra Singh80% (5)
- Peripheral NeuropathyDocument87 pagesPeripheral NeuropathyAsaraf AliNo ratings yet
- Stevens-Johnson Syndrome CASEDocument38 pagesStevens-Johnson Syndrome CASEChristy Rose AgrisNo ratings yet
- N TrigeminusDocument11 pagesN TrigeminusNatalia TeteleptaNo ratings yet
- Facial Pain:: Types of NeuralgiaDocument7 pagesFacial Pain:: Types of NeuralgiaNada BrassnNo ratings yet
- Orofacial Pain: DR Samreen Younas Pgr-I (FCPS) OmfsDocument49 pagesOrofacial Pain: DR Samreen Younas Pgr-I (FCPS) OmfsmishaNo ratings yet
- Trigeminal Neura L Gi A and Its Management: Rahul Sharma Dept of OMFS DAV Dental CollegeDocument79 pagesTrigeminal Neura L Gi A and Its Management: Rahul Sharma Dept of OMFS DAV Dental CollegeIsyana Khaerunisa100% (2)
- Management Trigeminal NeuralgiaDocument28 pagesManagement Trigeminal NeuralgiaApeksha JadhavNo ratings yet
- Immune Mediated Myopathies.5Document22 pagesImmune Mediated Myopathies.5wahby khatir100% (1)
- Occlusal TraumaDocument3 pagesOcclusal TraumaAbdullah SaleemNo ratings yet
- Fluids & Electrolyte NewDocument154 pagesFluids & Electrolyte NewMaria Visitacion100% (2)
- Test of Memory Malingering (TOMM)Document11 pagesTest of Memory Malingering (TOMM)Helping OthersNo ratings yet
- Glipizide Patient HandoutDocument3 pagesGlipizide Patient HandoutsilvanaanggraeniNo ratings yet
- CVA - Compilation of All BooksDocument4 pagesCVA - Compilation of All BooksJohnpeter EsporlasNo ratings yet
- (A) Multiple Choice Questions & Answers: Corona Quiz & Updates For Students (Dated: 01.04.2020)Document4 pages(A) Multiple Choice Questions & Answers: Corona Quiz & Updates For Students (Dated: 01.04.2020)Susmi RoyNo ratings yet
- MCI Screening TestDocument249 pagesMCI Screening TestmohammadsayfooNo ratings yet
- FNCPDocument3 pagesFNCPDjan Kurvie ValencerinaNo ratings yet
- NCMB 312 MS RLE WEEK 15 Concept Mapping GI BleedingDocument2 pagesNCMB 312 MS RLE WEEK 15 Concept Mapping GI BleedinggabbyNo ratings yet
- CASE STUDY PheumoniaDocument5 pagesCASE STUDY PheumoniaEdelweiss Marie CayetanoNo ratings yet
- Clinical Treatment of Obsessive Compulsive DisordeDocument11 pagesClinical Treatment of Obsessive Compulsive DisordeThálita PachecoNo ratings yet
- 7 - The Biliary TractDocument48 pages7 - The Biliary TractKim RamosNo ratings yet
- Drug Study 1Document5 pagesDrug Study 1Alen Alano100% (1)
- Morphology Morphology: Gross: White, Chalky Fat NecrosisDocument50 pagesMorphology Morphology: Gross: White, Chalky Fat NecrosisJc GaldosNo ratings yet
- HW#4 PaharmacologyDocument5 pagesHW#4 PaharmacologyMICHAEL GABRIEL JIMENEZNo ratings yet
- Fbi BlokDocument1 pageFbi BlokRumidi NgadiniNo ratings yet
- Thyroid Disease in PregnancyDocument17 pagesThyroid Disease in Pregnancydaniel100% (1)
- Eye Bags ReliefDocument27 pagesEye Bags ReliefNatsu DragneelNo ratings yet
- Methodical Manual For Independent Work of Students On 6 CourseDocument129 pagesMethodical Manual For Independent Work of Students On 6 CourseAzra AzmunaNo ratings yet
- The Final FRCR Complete Revision Notes-Pages-Deleted - PagenumberDocument364 pagesThe Final FRCR Complete Revision Notes-Pages-Deleted - PagenumberObaidy AlbushaherNo ratings yet
- Coronavirus: Say True or False Answer The Following QuestionsDocument1 pageCoronavirus: Say True or False Answer The Following QuestionsMARIONo ratings yet
- Optic NeurolitisDocument33 pagesOptic NeurolitisMoukdavanh KhamkhouneNo ratings yet
- Psychiatric NursingDocument87 pagesPsychiatric NursingemythereseNo ratings yet
- Vaccine and Autism MisinformationDocument10 pagesVaccine and Autism Misinformationapi-547401454No ratings yet
- What Is HIVDocument18 pagesWhat Is HIVTaufik KhanNo ratings yet
- Kelly and Kay HallDocument7 pagesKelly and Kay HallSatyendra KumarNo ratings yet
- Obsessive-Compulsive Disorder (OCD)Document16 pagesObsessive-Compulsive Disorder (OCD)Yousef A. MehdawiNo ratings yet
- Guidelines For SCC (R)Document86 pagesGuidelines For SCC (R)lionmusikaNo ratings yet

























































































Download as ppt, pdf, or txt
You might also like
- Cranial Nerve AssessmentDocument42 pagesCranial Nerve AssessmentValeryn Quiman100% (8)
- Oral Cancer 26.3.19Document23 pagesOral Cancer 26.3.19Pradeep100% (2)
- DACRYOCYSTITISDocument34 pagesDACRYOCYSTITISAriyanie Nurtania100% (1)
- Diseases of Oral CavityDocument60 pagesDiseases of Oral Cavityfredrick damian80% (5)
- Introduction To Agada Tantra, Visha & It's Classification, Properties & Action of Visha, Diagnosis of Poisoning, Treatment of PoisoningDocument123 pagesIntroduction To Agada Tantra, Visha & It's Classification, Properties & Action of Visha, Diagnosis of Poisoning, Treatment of PoisoningAbiskar Adhikari100% (14)
- Trigeminal NeuralgiaDocument15 pagesTrigeminal NeuralgiaMihir Patel75% (4)
- Anatomy of The Facial NerveDocument75 pagesAnatomy of The Facial NerveRao Rizwan Shakoor67% (3)
- Sialogogue and Anti-SialogogueDocument20 pagesSialogogue and Anti-SialogogueFoysal Sirazee60% (10)
- Sterisol Instructions For UseDocument10 pagesSterisol Instructions For UseJoe Shewale100% (1)
- CONJUNCTIVITISDocument67 pagesCONJUNCTIVITISNauli Panjaitan86% (7)
- Dandy WalkerDocument12 pagesDandy WalkerzarithNo ratings yet
- Trigeminal Neuralgia Oral SurgeryDocument48 pagesTrigeminal Neuralgia Oral SurgeryFourthMolar.com67% (3)
- Trigeminal NeuralgiaDocument3 pagesTrigeminal NeuralgiaAira Alaro50% (2)
- SyncopeDocument28 pagesSyncopeDurgesh PushkarNo ratings yet
- Sialogogue and Anti SialogogueDocument6 pagesSialogogue and Anti SialogoguePutri Farahmida50% (2)
- Bell's PalsyDocument20 pagesBell's PalsyVishesh JainNo ratings yet
- OsteomyelitisDocument21 pagesOsteomyelitisSurgeonZak50% (2)
- Sialogogues & Anti SailogoguesDocument43 pagesSialogogues & Anti SailogoguesTavleen KaurNo ratings yet
- Anaphylactic Shock LectureDocument32 pagesAnaphylactic Shock LectureIchal 'petta' Malebbi100% (1)
- Trigeminal Neuralgia and Its ManagementDocument79 pagesTrigeminal Neuralgia and Its ManagementRohit SharmaNo ratings yet
- Bell' Palsy - PPT Report - PPT FINALDocument21 pagesBell' Palsy - PPT Report - PPT FINALCarshena Cuares100% (1)
- Raynaud's Disease - JERAIZADocument23 pagesRaynaud's Disease - JERAIZAmaU439No ratings yet
- StomatitisDocument44 pagesStomatitisNessa Layos Morillo100% (1)
- Head InjuryDocument31 pagesHead InjuryZawawi Ibnu Rosyid0% (1)
- Eye Banking OphthalmologyDocument21 pagesEye Banking Ophthalmologyvivekrajbhilai5850100% (2)
- Vertebrobasilar Insufficiency/Syndrome: Hitesh Rohit (3 Year BPT)Document14 pagesVertebrobasilar Insufficiency/Syndrome: Hitesh Rohit (3 Year BPT)Hitesh N RohitNo ratings yet
- Balanced Diet: Bhavya Mds I Year Department of Conservative Dentistry & EndodonticsDocument76 pagesBalanced Diet: Bhavya Mds I Year Department of Conservative Dentistry & EndodonticsMayank AggarwalNo ratings yet
- By: Sarika Yadav Asst. LecturerDocument49 pagesBy: Sarika Yadav Asst. LecturerSarika YadavNo ratings yet
- TMJ DislocationDocument56 pagesTMJ DislocationAlok BhardwajNo ratings yet
- Meniere DiseaseDocument16 pagesMeniere DiseaseNavjot Brar100% (2)
- Chronic Otitis Media Types, Investigations, TreatmentDocument43 pagesChronic Otitis Media Types, Investigations, TreatmentPrasanna DattaNo ratings yet
- Cysts of Oral CavityDocument112 pagesCysts of Oral CavityMukhallat Qazi100% (1)
- Ameloblastoma: Submitted byDocument9 pagesAmeloblastoma: Submitted byJana AliNo ratings yet
- Local AnesthesiaDocument121 pagesLocal AnesthesiaGabriela Cocieru Motelica100% (2)
- Pathophysiology of Pain and Pain Assessment PDFDocument12 pagesPathophysiology of Pain and Pain Assessment PDFRaisa AriesthaNo ratings yet
- Facial NerveDocument80 pagesFacial Nerverasagna reddyNo ratings yet
- Pemphigus vulgarisPPTDocument23 pagesPemphigus vulgarisPPTSiti HanisaNo ratings yet
- The EarDocument59 pagesThe EarJasmin Jacob100% (5)
- Carcinoma TongueDocument39 pagesCarcinoma TongueVijay Krishna Murthy33% (3)
- Deep Bite 6Document97 pagesDeep Bite 6Manjunath Bellary100% (2)
- Congestive Heart Failure PDFDocument49 pagesCongestive Heart Failure PDFVerinice NañascaNo ratings yet
- OsteomyelitisDocument47 pagesOsteomyelitisArmand Al HaraaniNo ratings yet
- SHASTIUPAKRAMAIJAARDocument10 pagesSHASTIUPAKRAMAIJAARRavi SharmaNo ratings yet
- Lichen Planus: DR Hira BashirDocument37 pagesLichen Planus: DR Hira BashirSaroash SadruddinNo ratings yet
- GINGIVITISDocument43 pagesGINGIVITISRamyaNo ratings yet
- Question Papers For Bds Second YearDocument6 pagesQuestion Papers For Bds Second Yearsridevi sivaramakrishnanNo ratings yet
- Anchorage in OrthodonticsDocument103 pagesAnchorage in OrthodonticsEmad Ahmad Anis100% (2)
- NSAIDsDocument12 pagesNSAIDsjelly100% (1)
- Routes of Drug AdministrationDocument42 pagesRoutes of Drug AdministrationKandarp PatelNo ratings yet
- Oral Pathology - Physical & Chemical Injuries of Oral CavityDocument44 pagesOral Pathology - Physical & Chemical Injuries of Oral CavityRachit Srivastava83% (18)
- ENCEPHALITISDocument37 pagesENCEPHALITISNida NaazNo ratings yet
- Preanesthetic Medication PDFDocument5 pagesPreanesthetic Medication PDFSayan NagNo ratings yet
- Eye ExaminationDocument23 pagesEye Examinationcynthia167No ratings yet
- Healing of Oral WoundsDocument73 pagesHealing of Oral WoundsMadhvendra Singh80% (5)
- Peripheral NeuropathyDocument87 pagesPeripheral NeuropathyAsaraf AliNo ratings yet
- Stevens-Johnson Syndrome CASEDocument38 pagesStevens-Johnson Syndrome CASEChristy Rose AgrisNo ratings yet
- N TrigeminusDocument11 pagesN TrigeminusNatalia TeteleptaNo ratings yet
- Facial Pain:: Types of NeuralgiaDocument7 pagesFacial Pain:: Types of NeuralgiaNada BrassnNo ratings yet
- Orofacial Pain: DR Samreen Younas Pgr-I (FCPS) OmfsDocument49 pagesOrofacial Pain: DR Samreen Younas Pgr-I (FCPS) OmfsmishaNo ratings yet
- Trigeminal Neura L Gi A and Its Management: Rahul Sharma Dept of OMFS DAV Dental CollegeDocument79 pagesTrigeminal Neura L Gi A and Its Management: Rahul Sharma Dept of OMFS DAV Dental CollegeIsyana Khaerunisa100% (2)
- Management Trigeminal NeuralgiaDocument28 pagesManagement Trigeminal NeuralgiaApeksha JadhavNo ratings yet
- Immune Mediated Myopathies.5Document22 pagesImmune Mediated Myopathies.5wahby khatir100% (1)
- Occlusal TraumaDocument3 pagesOcclusal TraumaAbdullah SaleemNo ratings yet
- Fluids & Electrolyte NewDocument154 pagesFluids & Electrolyte NewMaria Visitacion100% (2)
- Test of Memory Malingering (TOMM)Document11 pagesTest of Memory Malingering (TOMM)Helping OthersNo ratings yet
- Glipizide Patient HandoutDocument3 pagesGlipizide Patient HandoutsilvanaanggraeniNo ratings yet
- CVA - Compilation of All BooksDocument4 pagesCVA - Compilation of All BooksJohnpeter EsporlasNo ratings yet
- (A) Multiple Choice Questions & Answers: Corona Quiz & Updates For Students (Dated: 01.04.2020)Document4 pages(A) Multiple Choice Questions & Answers: Corona Quiz & Updates For Students (Dated: 01.04.2020)Susmi RoyNo ratings yet
- MCI Screening TestDocument249 pagesMCI Screening TestmohammadsayfooNo ratings yet
- FNCPDocument3 pagesFNCPDjan Kurvie ValencerinaNo ratings yet
- NCMB 312 MS RLE WEEK 15 Concept Mapping GI BleedingDocument2 pagesNCMB 312 MS RLE WEEK 15 Concept Mapping GI BleedinggabbyNo ratings yet
- CASE STUDY PheumoniaDocument5 pagesCASE STUDY PheumoniaEdelweiss Marie CayetanoNo ratings yet
- Clinical Treatment of Obsessive Compulsive DisordeDocument11 pagesClinical Treatment of Obsessive Compulsive DisordeThálita PachecoNo ratings yet
- 7 - The Biliary TractDocument48 pages7 - The Biliary TractKim RamosNo ratings yet
- Drug Study 1Document5 pagesDrug Study 1Alen Alano100% (1)
- Morphology Morphology: Gross: White, Chalky Fat NecrosisDocument50 pagesMorphology Morphology: Gross: White, Chalky Fat NecrosisJc GaldosNo ratings yet
- HW#4 PaharmacologyDocument5 pagesHW#4 PaharmacologyMICHAEL GABRIEL JIMENEZNo ratings yet
- Fbi BlokDocument1 pageFbi BlokRumidi NgadiniNo ratings yet
- Thyroid Disease in PregnancyDocument17 pagesThyroid Disease in Pregnancydaniel100% (1)
- Eye Bags ReliefDocument27 pagesEye Bags ReliefNatsu DragneelNo ratings yet
- Methodical Manual For Independent Work of Students On 6 CourseDocument129 pagesMethodical Manual For Independent Work of Students On 6 CourseAzra AzmunaNo ratings yet
- The Final FRCR Complete Revision Notes-Pages-Deleted - PagenumberDocument364 pagesThe Final FRCR Complete Revision Notes-Pages-Deleted - PagenumberObaidy AlbushaherNo ratings yet
- Coronavirus: Say True or False Answer The Following QuestionsDocument1 pageCoronavirus: Say True or False Answer The Following QuestionsMARIONo ratings yet
- Optic NeurolitisDocument33 pagesOptic NeurolitisMoukdavanh KhamkhouneNo ratings yet
- Psychiatric NursingDocument87 pagesPsychiatric NursingemythereseNo ratings yet
- Vaccine and Autism MisinformationDocument10 pagesVaccine and Autism Misinformationapi-547401454No ratings yet
- What Is HIVDocument18 pagesWhat Is HIVTaufik KhanNo ratings yet
- Kelly and Kay HallDocument7 pagesKelly and Kay HallSatyendra KumarNo ratings yet
- Obsessive-Compulsive Disorder (OCD)Document16 pagesObsessive-Compulsive Disorder (OCD)Yousef A. MehdawiNo ratings yet
- Guidelines For SCC (R)Document86 pagesGuidelines For SCC (R)lionmusikaNo ratings yet