Download as ppt, pdf, or txt
You might also like
- Centrifugal Pumps: Process Calculation / Data SheetDocument3 pagesCentrifugal Pumps: Process Calculation / Data SheetMurali MuthuNo ratings yet
- Chest TraumaDocument4 pagesChest TraumaTrishia GuillermoNo ratings yet
- NoseDocument15 pagesNoseArooshaNo ratings yet
- Effects of Pressure ChangesDocument55 pagesEffects of Pressure Changesamro kirkisawiNo ratings yet
- S T A R T: Imple Riage ND Apid ReatmentDocument17 pagesS T A R T: Imple Riage ND Apid ReatmentNavine NavNo ratings yet
- Shanz - Ent 1.02 Middle EarDocument3 pagesShanz - Ent 1.02 Middle EarPetrina XuNo ratings yet
- Thoracic Trauma EIDCPDocument52 pagesThoracic Trauma EIDCPAris RamdhaniNo ratings yet
- DR - Ravinder Singh Nagi Asst ProffessorDocument52 pagesDR - Ravinder Singh Nagi Asst ProffessorPrabaa KharanNo ratings yet
- BIMC Update PresentationDocument25 pagesBIMC Update PresentationWahyuNo ratings yet
- X RaysDocument1 pageX Rayszubair syedNo ratings yet
- ENT Radiology ADocument64 pagesENT Radiology AMitulsinh M RavaljiNo ratings yet
- Salivary Glands - Anatomy & Clinical Examination-1Document59 pagesSalivary Glands - Anatomy & Clinical Examination-1vinitha kattaNo ratings yet
- Shanz - Ent 1.07 NoseDocument4 pagesShanz - Ent 1.07 NosePetrina XuNo ratings yet
- Tehnik Dasar Laparoskopik - Pneumoperatonium-Veress NeedleDocument31 pagesTehnik Dasar Laparoskopik - Pneumoperatonium-Veress NeedleDaniel LesmanaNo ratings yet
- Eye & EntDocument124 pagesEye & EntAstik MukherjeeNo ratings yet
- Stenotic Valvular Heart Disease and Its Anaesthetic ManagementDocument75 pagesStenotic Valvular Heart Disease and Its Anaesthetic ManagementDr MounicaNo ratings yet
- Mediastinum AsudaDocument15 pagesMediastinum Asudaasudamajid9No ratings yet
- 4bi 1le Active RecallDocument4 pages4bi 1le Active RecallAlexandryaHaleNo ratings yet
- Lecture 1 Otitis MediaDocument82 pagesLecture 1 Otitis MediaTarun SharmaNo ratings yet
- Goldlin Beaulah.A Clinical Instructor - EdDocument75 pagesGoldlin Beaulah.A Clinical Instructor - EdBeyene FelekeNo ratings yet
- Trauma AssessmentDocument77 pagesTrauma AssessmentMary Jane TiangsonNo ratings yet
- Large Bowel Series: Barium EnemaDocument5 pagesLarge Bowel Series: Barium EnemaKaye A. JardinicoNo ratings yet
- Airway Devices PPT-1Document77 pagesAirway Devices PPT-1Armaanjeet SinghNo ratings yet
- Practice Guidelines For Juniors 01 June 2016Document3 pagesPractice Guidelines For Juniors 01 June 2016ElaineNo ratings yet
- Pediatric InstrumentsDocument30 pagesPediatric InstrumentsSanjit PandeyNo ratings yet
- Maxillofascial Surgery AnesthesiaDocument62 pagesMaxillofascial Surgery AnesthesiaHossam atefNo ratings yet
- Common ENT ProblemsDocument41 pagesCommon ENT ProblemsMohamed GhabrunNo ratings yet
- CBL Os TraumaDocument35 pagesCBL Os TraumaKirthiga15No ratings yet
- Craniotomy FlapsDocument41 pagesCraniotomy FlapsKaramsi Gopinath NaikNo ratings yet
- ATLS TemplateDocument6 pagesATLS Templatesyasya100% (1)
- TracheostomyDocument42 pagesTracheostomyEnt IMDCNo ratings yet
- Endoscopic Sinus SurgeryDocument33 pagesEndoscopic Sinus SurgeryruthmindosiahaanNo ratings yet
- 312 RM - Tracheostomy Care SuctioningDocument4 pages312 RM - Tracheostomy Care Suctioningesbercinio8528valNo ratings yet
- Chest Tubes: Reason For UseDocument15 pagesChest Tubes: Reason For UseJack Keurig67% (3)
- Emergency Procedures Masterclass: Siamak Moayedi, MDDocument23 pagesEmergency Procedures Masterclass: Siamak Moayedi, MDCoding NinjaNo ratings yet
- Bilateral Direct HerniaDocument7 pagesBilateral Direct HerniaTeja Laksana NukanaNo ratings yet
- Primary and Secondary Survey MiraDocument50 pagesPrimary and Secondary Survey MiraAfifah SelamatNo ratings yet
- Supraglottic Airway Devices: Moderator-Dr. Naresh Tyagi Dr. Nishi ThawaitDocument71 pagesSupraglottic Airway Devices: Moderator-Dr. Naresh Tyagi Dr. Nishi ThawaitMark JohnsonNo ratings yet
- 2019, Nasal Trauma and EpistaxisDocument43 pages2019, Nasal Trauma and EpistaxisakeelNo ratings yet
- Cme Trauma Management ZakwanDocument44 pagesCme Trauma Management ZakwansyasyaNo ratings yet
- IT 4 Thoracic TraumaDocument31 pagesIT 4 Thoracic TraumaDesi MawarniNo ratings yet
- BarotraumaDocument26 pagesBarotraumatikahamidahNo ratings yet
- EmergeDocument24 pagesEmergeili_izyanNo ratings yet
- TracheaDocument2 pagesTracheaChalsey Jene LorestoNo ratings yet
- Tracheostomy CareDocument34 pagesTracheostomy CareZgherea Mihai100% (1)
- ENDOSCOPIC ANATOMY of NOSE & PNS.Document57 pagesENDOSCOPIC ANATOMY of NOSE & PNS.Prasanna DattaNo ratings yet
- M.Gopinathan Department of Ent CH.M.CDocument38 pagesM.Gopinathan Department of Ent CH.M.Csuncarn88No ratings yet
- 07.03.44 Neonatal IntubationDocument6 pages07.03.44 Neonatal IntubationAya AshrafNo ratings yet
- ICU OnePager Perc TracheostomyDocument1 pageICU OnePager Perc TracheostomycaioaccorsiNo ratings yet
- Complications of Laparoscopic SurgeriesDocument40 pagesComplications of Laparoscopic Surgeriesrajan kumar100% (10)
- Tracheostomy: by Veronica Robert, MD 4 Moderator DR - SamsonDocument41 pagesTracheostomy: by Veronica Robert, MD 4 Moderator DR - SamsonMacktevin FraterinNo ratings yet
- Sino Nasal MalignanciesDocument32 pagesSino Nasal MalignanciesShivani GauswamiNo ratings yet
- UW (Step 1) ENT - Educational Objectives PDFDocument6 pagesUW (Step 1) ENT - Educational Objectives PDFUsama BilalNo ratings yet
- Neonatal IntubationDocument6 pagesNeonatal IntubationAndrea Nur SabrinaNo ratings yet
- Tracheostomy Care (NCM 112 Rle)Document2 pagesTracheostomy Care (NCM 112 Rle)Rose Ann BollerosNo ratings yet
- Causes and Evaluation of EpiphoraDocument69 pagesCauses and Evaluation of EpiphoraSristi ThakurNo ratings yet
- Anatomi HidungDocument28 pagesAnatomi HidungferyantoachmadNo ratings yet
- Mri Procedure of PNSDocument57 pagesMri Procedure of PNSAsmita BhattNo ratings yet
- Esophagus Lecture Fatima NEW 2015Document31 pagesEsophagus Lecture Fatima NEW 2015Aileen EmyNo ratings yet
- Modern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.From EverandModern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.No ratings yet
- UT Gain or Loss in DBDocument3 pagesUT Gain or Loss in DBgbsubbu100% (1)
- Process Instrumentation 1Document61 pagesProcess Instrumentation 1Charles M Lukusa100% (3)
- Incompressible Fluid Mechanics PDFDocument187 pagesIncompressible Fluid Mechanics PDFPrabhat PiyushNo ratings yet
- Flooding, Dewatering and VentingDocument5 pagesFlooding, Dewatering and VentingAngel NgoNo ratings yet
- ParkerORIGACatalog 0952 Valves 1108Document60 pagesParkerORIGACatalog 0952 Valves 1108Jas SumNo ratings yet
- Kidde ECS Fire Suppression System Component DescriptionDocument1 pageKidde ECS Fire Suppression System Component DescriptionSergio HZNo ratings yet
- C1531-15 Standard Test Methods For in Situ Measurement of Masonry Mortar Joint Shear Strength IndexDocument7 pagesC1531-15 Standard Test Methods For in Situ Measurement of Masonry Mortar Joint Shear Strength IndexLorena JimenezNo ratings yet
- OISD STD 236 Refrigerated Storage1 PDFDocument97 pagesOISD STD 236 Refrigerated Storage1 PDFDhiren Prajapati100% (2)
- Equipment Design: Mechanical Aspects Prof. Shabina Khanam Department of Chemical Engineering Indian Institute of Technology - Roorkee TerminologiesDocument18 pagesEquipment Design: Mechanical Aspects Prof. Shabina Khanam Department of Chemical Engineering Indian Institute of Technology - Roorkee Terminologiesdurgesh patelNo ratings yet
- Pressure Vessel Handbook Ninth Edition 1992 PDFDocument481 pagesPressure Vessel Handbook Ninth Edition 1992 PDFjudico60_70175733No ratings yet
- FMDS0128Document103 pagesFMDS0128Suneesh PNo ratings yet
- ST-HST-MKT-01 Hydrostatik Testing Rev.00 PDFDocument13 pagesST-HST-MKT-01 Hydrostatik Testing Rev.00 PDFAffian WidjanarkoNo ratings yet
- Variants of SIMPLEDocument26 pagesVariants of SIMPLEYu Kok HwaNo ratings yet
- ICP First Semester Test ReviewDocument10 pagesICP First Semester Test ReviewKyra HuntNo ratings yet
- Appendix B PDFDocument1 pageAppendix B PDFLuis Felipe Mera GrandasNo ratings yet
- Black Oil DefinitionsDocument21 pagesBlack Oil Definitionsmanish.7417No ratings yet
- Design BasisDocument34 pagesDesign BasisRajesh BarkurNo ratings yet
- Irrigation Engineering and Hydraulic Structure Santosh Kumar GargDocument165 pagesIrrigation Engineering and Hydraulic Structure Santosh Kumar GargAnand RatnaNo ratings yet
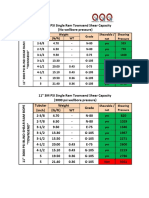
- Shear Matrix TownsendDocument1 pageShear Matrix TownsendBoedi SyafiqNo ratings yet
- 6th Chemistry Book - Vol-2Document118 pages6th Chemistry Book - Vol-2karansharma690100% (1)
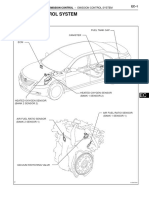
- Emission Control System: Parts LocationDocument23 pagesEmission Control System: Parts LocationNassar Al-EssawiNo ratings yet
- 2 Phase Flow AGA EqnDocument12 pages2 Phase Flow AGA EqnSUDARSAN SNo ratings yet
- Fluid Mech Sheet 4 IAETDocument11 pagesFluid Mech Sheet 4 IAET3bdo MahmoudNo ratings yet
- Comparative Pressure/Vacuum Units : Mbar Torr In. of HG (Absolute) (Absolute) (Gauge)Document1 pageComparative Pressure/Vacuum Units : Mbar Torr In. of HG (Absolute) (Absolute) (Gauge)mecambNo ratings yet
- Rv-Rvalve NF00033 1111Document12 pagesRv-Rvalve NF00033 1111David MoleroNo ratings yet
- Binks Mach 1Sl HVLP Spray Gun 7000-Xxxx-XDocument8 pagesBinks Mach 1Sl HVLP Spray Gun 7000-Xxxx-XKevin KellyNo ratings yet
- SkinDocument8 pagesSkinYamal E Askoul TNo ratings yet
- Methods Optimization in Accelerated Solvent ExtractionDocument4 pagesMethods Optimization in Accelerated Solvent ExtractionSyed 'UmarNo ratings yet
- Heatless Adsorption Dryers Ultrapac ClassicDocument4 pagesHeatless Adsorption Dryers Ultrapac ClassicДмитрий КоваленкоNo ratings yet