Download as ppt, pdf, or txt
You might also like
- (Medicalstudyzone - Com) Medicine - Irfan Masood LatestDocument701 pages(Medicalstudyzone - Com) Medicine - Irfan Masood LatestMajid Ahmed FareaNo ratings yet
- Surgical Finals Passing The Clinical PDFDocument40 pagesSurgical Finals Passing The Clinical PDFnetradeep67% (3)
- What Is The Speed of Handpiece Used in OMFSDocument2 pagesWhat Is The Speed of Handpiece Used in OMFSkem100% (1)
- Outline Post Exposure Prophylaxis (Pep)Document9 pagesOutline Post Exposure Prophylaxis (Pep)Matt PNo ratings yet
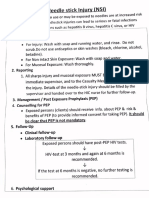
- Needle: Stick Injury (NSI)Document5 pagesNeedle: Stick Injury (NSI)dr rajoreNo ratings yet
- Post Exposure Prophylaxis For HivDocument21 pagesPost Exposure Prophylaxis For Hivdr.a.k.gupta6924No ratings yet
- NPEP Procedure Flowchart TemplateDocument2 pagesNPEP Procedure Flowchart TemplatededekfridayNo ratings yet
- Post Exposure Prophylaxis Imep TotDocument47 pagesPost Exposure Prophylaxis Imep TotHarshaWakodkarNo ratings yet
- Needle Stick InjuryDocument27 pagesNeedle Stick InjuryVishal ThakareNo ratings yet
- Post-Exposure Prophylaxis: DR Shazia Shams Lecturer PHI, NagpurDocument36 pagesPost-Exposure Prophylaxis: DR Shazia Shams Lecturer PHI, NagpurHarshaWakodkarNo ratings yet
- HIV Infection Fact SheetDocument38 pagesHIV Infection Fact SheetYu Mong LeeNo ratings yet
- Needle Stick Injury Prevention and Management: Nirupama Sahoo ICNDocument18 pagesNeedle Stick Injury Prevention and Management: Nirupama Sahoo ICNSantoshMohapatraNo ratings yet
- Hiv Factsheet Biomedical Prevention Hiv Prep PepDocument2 pagesHiv Factsheet Biomedical Prevention Hiv Prep PepMagie FaragNo ratings yet
- What Is HIV?Document8 pagesWhat Is HIV?Quan ThieuNo ratings yet
- REVIEWER - Management of Patients With Immune Deficiency DisordersDocument2 pagesREVIEWER - Management of Patients With Immune Deficiency DisordersRaquel HatulanNo ratings yet
- Medical Virology: Dr. Dalia M. Mohsen Prof. in MicrobiologyDocument43 pagesMedical Virology: Dr. Dalia M. Mohsen Prof. in MicrobiologyDalia M. MohsenNo ratings yet
- Mammoth: Chapter 36: HIV & AIDSDocument14 pagesMammoth: Chapter 36: HIV & AIDSBreeanne GallonNo ratings yet
- CDC Hiv Pep101Document2 pagesCDC Hiv Pep101Sangeetha HospitalNo ratings yet
- Slide Hiv AidsDocument39 pagesSlide Hiv Aidsandirio7486No ratings yet
- Lecture EightDocument4 pagesLecture EightJohnNo ratings yet
- Hepatitis B PDFDocument15 pagesHepatitis B PDFAvicenna_MSCNo ratings yet
- The Person Living With: Hiv/Disease Hiv/DiseaseDocument59 pagesThe Person Living With: Hiv/Disease Hiv/DiseasejaydipNo ratings yet
- Needle Stick InjuriesDocument24 pagesNeedle Stick InjuriesSarthak LaboratoryNo ratings yet
- CD Hiv-Aids PDF ReviewerDocument33 pagesCD Hiv-Aids PDF ReviewerMeryville JacildoNo ratings yet
- AidsDocument9 pagesAidsanishpantha530No ratings yet
- En - Acc Exposure Blood Body Fluids - PosterDocument1 pageEn - Acc Exposure Blood Body Fluids - Posterdhira aninditaNo ratings yet
- PDF DocumentDocument1 pagePDF DocumentellaNo ratings yet
- Sharp Injury Surveillance CMEDocument47 pagesSharp Injury Surveillance CMENOR HASSIDANo ratings yet
- PM - Materi 1 HIV AIDS RevDocument72 pagesPM - Materi 1 HIV AIDS RevSaly AlatasNo ratings yet
- HIV Testing Labs FlowchartDocument1 pageHIV Testing Labs Flowcharthamody662002No ratings yet
- Hiv/Aids: Wagiyo, SKP., M.Kep., SP MatDocument34 pagesHiv/Aids: Wagiyo, SKP., M.Kep., SP MatNettha Bintang DhiafakhriNo ratings yet
- Hepatitis A-EDocument34 pagesHepatitis A-EVer Garcera TalosigNo ratings yet
- 4 HivDocument33 pages4 HivAmr KhayyalNo ratings yet
- CDC Hiv Consumer Info Sheet Pep 101Document2 pagesCDC Hiv Consumer Info Sheet Pep 101No NameNo ratings yet
- Hepatitis A-E Viruses: Farida Purnamasari.,SKM 2012Document51 pagesHepatitis A-E Viruses: Farida Purnamasari.,SKM 2012siapaa01No ratings yet
- Hiv Seminar 2019Document49 pagesHiv Seminar 2019clarice_condeno100% (1)
- RABIES TreatmentDocument8 pagesRABIES TreatmentJomarNo ratings yet
- Influenza: What We Know: Mohammad Nuriman Bin Mohd Zainuddin (Aa0890) Lablink, KPJ Puteri Specialist HospitalDocument24 pagesInfluenza: What We Know: Mohammad Nuriman Bin Mohd Zainuddin (Aa0890) Lablink, KPJ Puteri Specialist Hospitaliman zainuddinNo ratings yet
- Screening For Transfusion-Transmissible Infections: Pgi Pauline BaluisDocument60 pagesScreening For Transfusion-Transmissible Infections: Pgi Pauline BaluisPahw BaluisNo ratings yet
- CDC Hiv Pep101Document1 pageCDC Hiv Pep101api-359864813No ratings yet
- Viral Hepatitis For NursesDocument44 pagesViral Hepatitis For Nursesjohnfoday2022No ratings yet
- HEPATITIS B in The WorkplaceDocument51 pagesHEPATITIS B in The WorkplaceApril Joy MercadoNo ratings yet
- Hep B VirusDocument20 pagesHep B VirusBhupesh ChandNo ratings yet
- Occupational Health Risks For Healthcare WorkersDocument32 pagesOccupational Health Risks For Healthcare WorkersSyi VeenaNo ratings yet
- AIDSDocument36 pagesAIDSMohamed TahaNo ratings yet
- Progress in Clinical Research (Linda-Gail Bekker MBCHB, DTMH, DCH, FCP (SA), PHD.)Document171 pagesProgress in Clinical Research (Linda-Gail Bekker MBCHB, DTMH, DCH, FCP (SA), PHD.)National Press FoundationNo ratings yet
- Hiv and AidsDocument2 pagesHiv and AidsEllaine FernandezNo ratings yet
- Vis Rabies PDFDocument2 pagesVis Rabies PDFFA AnthonyNo ratings yet
- HivDocument29 pagesHivSUTHAN100% (2)
- Post Exposure Prophylaxis: Hepatitis B, Hepatitis C and HivDocument10 pagesPost Exposure Prophylaxis: Hepatitis B, Hepatitis C and HivQaiser ZamanNo ratings yet
- Hepatitis A-E Viruses: An OverviewDocument49 pagesHepatitis A-E Viruses: An OverviewDeepak VermaNo ratings yet
- Virology - HIV LectureDocument20 pagesVirology - HIV LecturealetheacolleenpNo ratings yet
- 21W COVID-19 - Public Health and Vaccine UpdateDocument31 pages21W COVID-19 - Public Health and Vaccine UpdateViraj RavihansaNo ratings yet
- Hepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetDocument48 pagesHepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetNurhidayahNo ratings yet
- HIV Lecture Handout 2021Document10 pagesHIV Lecture Handout 2021Jimilyn GallowayNo ratings yet
- Management 2Document16 pagesManagement 2Moin PandithNo ratings yet
- Immunization AssignmentDocument4 pagesImmunization Assignmentgadoura95No ratings yet
- Rabies Menurut Inet MscapehDocument8 pagesRabies Menurut Inet MscapehenvadNo ratings yet
- Adult ImmunizationDocument43 pagesAdult ImmunizationTris100% (2)
- Hepatitis ADocument21 pagesHepatitis ADownload FilmNo ratings yet
- Pre-Exposure Prophylaxis (PrEP) For HIV Prevention: A Beginners Guide to PrEP for HIV Prevention.From EverandPre-Exposure Prophylaxis (PrEP) For HIV Prevention: A Beginners Guide to PrEP for HIV Prevention.No ratings yet
- Dr. Sebi’s Guide to Conquer Herpes: Learn the Most Effective and Natural Way to Fight Herpes by Following Dr. Sebi’s Alkaline Nutritional GuideFrom EverandDr. Sebi’s Guide to Conquer Herpes: Learn the Most Effective and Natural Way to Fight Herpes by Following Dr. Sebi’s Alkaline Nutritional GuideRating: 5 out of 5 stars5/5 (7)
- Coronavirus Crisis: Information and Help in the 2020 Pandemic - What Everyone Should KnowFrom EverandCoronavirus Crisis: Information and Help in the 2020 Pandemic - What Everyone Should KnowNo ratings yet
- Manwath Multi-Speciality Hospital: Date of Admission:-Name: - Reg. Bed: DiagnosisDocument1 pageManwath Multi-Speciality Hospital: Date of Admission:-Name: - Reg. Bed: DiagnosisnetradeepNo ratings yet
- Ca PenisDocument7 pagesCa PenisnetradeepNo ratings yet
- Nta Review of The Effectiveness of Treatment For Alcohol Problems Fullreport 2006 Alcohol2Document212 pagesNta Review of The Effectiveness of Treatment For Alcohol Problems Fullreport 2006 Alcohol2netradeepNo ratings yet
- Ent DNB DVD TopicsDocument11 pagesEnt DNB DVD TopicsnikitamkNo ratings yet
- Ca PenisDocument7 pagesCa PenisnetradeepNo ratings yet
- FistulaDocument23 pagesFistulanetradeep50% (2)
- Clinical Conditions Associated With Development of Acute Respiratory Distress SyndromeDocument1 pageClinical Conditions Associated With Development of Acute Respiratory Distress SyndromenetradeepNo ratings yet
- For AtdDocument1 pageFor AtdnetradeepNo ratings yet
- Bankruptcy Restructuring in IndiaDocument16 pagesBankruptcy Restructuring in IndianetradeepNo ratings yet
- Metabolic SyDocument3 pagesMetabolic SynetradeepNo ratings yet
- A Case Presentation: Under Guidance ofDocument13 pagesA Case Presentation: Under Guidance ofnetradeepNo ratings yet
- Case Presentation Dept. of Medicine VHLDocument13 pagesCase Presentation Dept. of Medicine VHLnetradeepNo ratings yet
- Career Exploration and PlanningDocument18 pagesCareer Exploration and PlanningJomole JosephNo ratings yet
- Symbiosis University Hospital and Research Center Symbiosis Medical College For Women ( )Document2 pagesSymbiosis University Hospital and Research Center Symbiosis Medical College For Women ( )SIDDHARTH SOMESHNo ratings yet
- Vascular DisordersDocument13 pagesVascular DisordersMichelle Dona MirallesNo ratings yet
- Form Pg-Sga PDFDocument2 pagesForm Pg-Sga PDFzain syalsabilaNo ratings yet
- 2015 JMP Academic Calendar Y1 5 BMed PDFDocument1 page2015 JMP Academic Calendar Y1 5 BMed PDFc3144394_783391065No ratings yet
- Occupational Therapy and Dementia Fact SheetDocument3 pagesOccupational Therapy and Dementia Fact SheetVeraNo ratings yet
- Muskuloskeletal Disorder Menggunakan: Analisa Dan Penilaian Risiko Metode Manual Tasks Risk Assessment (Mantra)Document8 pagesMuskuloskeletal Disorder Menggunakan: Analisa Dan Penilaian Risiko Metode Manual Tasks Risk Assessment (Mantra)Dirgntra AlanNo ratings yet
- Computational Fluid Dynamics and Trigeminal Sensory Examinations of Empty Nose Syndrome PatientsDocument60 pagesComputational Fluid Dynamics and Trigeminal Sensory Examinations of Empty Nose Syndrome Patientsmadhumitha srinivasNo ratings yet
- SARS: The Inside Story: Where Did SARS Come From?Document6 pagesSARS: The Inside Story: Where Did SARS Come From?ZauzaNo ratings yet
- Prefinal ProgramDocument1 pagePrefinal ProgramHussein AhmedNo ratings yet
- Osteochondroma of The Coronoid Process of The MandibleDocument4 pagesOsteochondroma of The Coronoid Process of The MandiblegtawidhiNo ratings yet
- Nursing Care For A Client With Chest Trauma: Reported By: Jazon, Gabriel Liberon PDocument100 pagesNursing Care For A Client With Chest Trauma: Reported By: Jazon, Gabriel Liberon PGabriel Liberon P. JazonNo ratings yet
- Pain ManagementDocument25 pagesPain ManagementnurminieNo ratings yet
- Arogya Sanjeevani PremiumDocument16 pagesArogya Sanjeevani PremiumGiriMahaNo ratings yet
- Malaria Control BrochureDocument2 pagesMalaria Control BrochureEkwoh Okwuchukwu ENo ratings yet
- IMNCIDocument26 pagesIMNCIrakeshr2007No ratings yet
- NPC 10 12 2015Document240 pagesNPC 10 12 2015SyaefudinNo ratings yet
- Acquired Heart DiseasesDocument41 pagesAcquired Heart DiseasesSaman SarKoNo ratings yet
- Hemolytic Uremic SyndromeDocument1 pageHemolytic Uremic SyndromeAndrea TeranNo ratings yet
- Phillipine Herbal MedicineDocument23 pagesPhillipine Herbal MedicineCENTHREE MAGALLANESNo ratings yet
- Kuliah 11 IBUV Anestesi Pada Hewan Besar PDFDocument29 pagesKuliah 11 IBUV Anestesi Pada Hewan Besar PDFElsi RahmadhaniNo ratings yet
- List of Attendees - Sorted by CountryDocument48 pagesList of Attendees - Sorted by CountryAmalia Tri Utami50% (2)
- Assignment # 01: Morton's NeuromaDocument5 pagesAssignment # 01: Morton's Neuromazoha hassanNo ratings yet
- ECSB - Flip ChartDocument51 pagesECSB - Flip ChartSeeker6801No ratings yet
- Mal de DebarquementDocument10 pagesMal de DebarquementFelipeAsenjoÁlvarezNo ratings yet
- Medication Errors - Where Do They Happen - The Pharmaceutical JournalDocument7 pagesMedication Errors - Where Do They Happen - The Pharmaceutical JournalAre Pee EtcNo ratings yet
- Pre Feasibility Report of Pharmacy Business in PakistanDocument26 pagesPre Feasibility Report of Pharmacy Business in Pakistanzaheer100% (1)
- ZXVZXCVZDocument1 pageZXVZXCVZjoycechicagoNo ratings yet