Download as ppt, pdf, or txt
You might also like
- Premalignant Lesions and Conditions: Submitted by-BALJEET KAUR B.D.S.-3 Year Roll No.15Document60 pagesPremalignant Lesions and Conditions: Submitted by-BALJEET KAUR B.D.S.-3 Year Roll No.15Rajat NangiaNo ratings yet
- Continuation Sheet TemplateDocument5 pagesContinuation Sheet TemplateWandy SejeliNo ratings yet
- Occupational Lung DiseaseDocument24 pagesOccupational Lung DiseaseprachitiNo ratings yet
- Chronic Obstructive Lung Diseases and Chronic Restrictive Lung DiseasesDocument59 pagesChronic Obstructive Lung Diseases and Chronic Restrictive Lung DiseasesGEORGENo ratings yet
- Chronic Obstructive Disease by HibaDocument38 pagesChronic Obstructive Disease by HibahibaNo ratings yet
- Dr. Sana Bashir DPT, MS-CPPTDocument46 pagesDr. Sana Bashir DPT, MS-CPPTbkdfiesefll100% (1)
- Neurology in TableDocument93 pagesNeurology in TableHassan Bani SaeidNo ratings yet
- BronchiectasisDocument60 pagesBronchiectasisArulNo ratings yet
- 2023.2024chronic Obstructive Pulmonary DiseaseDocument17 pages2023.2024chronic Obstructive Pulmonary Diseasesameh EidNo ratings yet
- Respiratory Failure PresentationDocument13 pagesRespiratory Failure PresentationHusnain Irshad AlviNo ratings yet
- Cystic Lung DiseasesDocument31 pagesCystic Lung DiseasesMuthannathb Thb100% (1)
- Review ArdsDocument25 pagesReview ArdsAdel HamadaNo ratings yet
- Hypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesDocument51 pagesHypersensitivity Pneumonitis: Diagnostic and Therapeutic ChallengesskchhabraNo ratings yet
- Acute Dyspnea First RevisionDocument56 pagesAcute Dyspnea First RevisionAradhanaRamchandaniNo ratings yet
- Occupational Lung DiseasesDocument75 pagesOccupational Lung DiseasesAnonymous h1XAlApsU100% (1)
- Respiratory Failure: Barry WardleDocument28 pagesRespiratory Failure: Barry Wardleapi-19826220No ratings yet
- Gold and Gina Guideline For Copd and AsthmaDocument56 pagesGold and Gina Guideline For Copd and AsthmaSomnath Das Gupta100% (1)
- Study Notes Respiratory SystemDocument19 pagesStudy Notes Respiratory SystemAnde Mangkuluhur Azhari ThalibbanNo ratings yet
- Asthma + COPD (Full)Document115 pagesAsthma + COPD (Full)selamsew alemuNo ratings yet
- 2nd Announcement JakNews 2024Document19 pages2nd Announcement JakNews 2024Nando EllaNo ratings yet
- Bronchiectasis: Dr.K.M.LakshmanarajanDocument238 pagesBronchiectasis: Dr.K.M.LakshmanarajanKM Lakshmana Rajan0% (1)
- 17 Multiple Cystic Lung DiseasesDocument18 pages17 Multiple Cystic Lung DiseasesMhmd Koros100% (1)
- Invasive Pulmonary Aspergi Llosis: Seminars in Respiratory and Critical Care MedicineDocument24 pagesInvasive Pulmonary Aspergi Llosis: Seminars in Respiratory and Critical Care MedicineChengShiun ShiueNo ratings yet
- Recurrent Respiratory Papillomatosis: FaringDocument49 pagesRecurrent Respiratory Papillomatosis: FaringIchsanJuliansyahNo ratings yet
- Sailedinitis PDFDocument8 pagesSailedinitis PDFNavatha MorthaNo ratings yet
- Ards 2Document7 pagesArds 2LUCIBELLOT1No ratings yet
- TBL - PneumothoraxDocument26 pagesTBL - PneumothoraxÁýáFáŕőúgNo ratings yet
- 13Lec-Approach To Neonates With Suspected Congenital InfectionsDocument56 pages13Lec-Approach To Neonates With Suspected Congenital InfectionsMinerva Stanciu100% (1)
- Asphyxialconditions 120917062150 Phpapp02Document93 pagesAsphyxialconditions 120917062150 Phpapp02minaaminmaNo ratings yet
- Resp Bronch N LaDocument56 pagesResp Bronch N LaMansi GandhiNo ratings yet
- Head Injury 1Document33 pagesHead Injury 1drvishal bhattNo ratings yet
- Bronchiectasis: Prepared By: Michelle TamorDocument17 pagesBronchiectasis: Prepared By: Michelle TamorMichelle TamorNo ratings yet
- Pulmonary HypertensionDocument26 pagesPulmonary Hypertensionakoeljames8543No ratings yet
- Acute Coronary Syndrome: by DR Moustafa Kamal Eldin, MD Lecturer of Cardiology Faculty of Medicine Fayoum UniversityDocument24 pagesAcute Coronary Syndrome: by DR Moustafa Kamal Eldin, MD Lecturer of Cardiology Faculty of Medicine Fayoum UniversityAbdulrahman Ahmed100% (1)
- Approach To Cough and HemoptysisDocument24 pagesApproach To Cough and Hemoptysisbansaleliza26No ratings yet
- Empyema 2Document31 pagesEmpyema 2Michelle SalimNo ratings yet
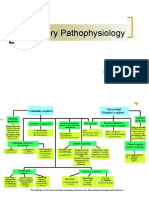
- Respiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDocument12 pagesRespiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDoc JacqueNo ratings yet
- BTS Sarcoidosis Clinical StatementDocument17 pagesBTS Sarcoidosis Clinical StatementDarrin WiebeNo ratings yet
- "Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareDocument51 pages"Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareSohil ElfarNo ratings yet
- Pulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung MetastasesDocument5 pagesPulmonary Sarcoidosis Presenting With Cannonball Pattern Mimicking Lung MetastasesIJAR JOURNALNo ratings yet
- Spiro Me Try Cheat Sheet 09Document2 pagesSpiro Me Try Cheat Sheet 09Yudha Perwira PutraNo ratings yet
- Diagnosis of PneumoconiosisDocument55 pagesDiagnosis of PneumoconiosiselsaNo ratings yet
- Surfactant PresentationDocument18 pagesSurfactant PresentationMaadaNo ratings yet
- The Pneumonias: Associate Professor Dr. Lauren Ţiu ŞorodocDocument60 pagesThe Pneumonias: Associate Professor Dr. Lauren Ţiu ŞorodocCristina Georgiana CoticăNo ratings yet
- Chronic Obstructive Pulmonary Disease: Martina S., Selda S., Sarah A.G., Dina H., Sonia C. UMFT Victor Babes'Document39 pagesChronic Obstructive Pulmonary Disease: Martina S., Selda S., Sarah A.G., Dina H., Sonia C. UMFT Victor Babes'Petcu FlorinaNo ratings yet
- Prone VentilationDocument25 pagesProne VentilationHazel AsperaNo ratings yet
- Diaphragm AnatomyDocument19 pagesDiaphragm AnatomyasujithdrNo ratings yet
- CryptococcosisDocument25 pagesCryptococcosisinvisibleyetinvincibleNo ratings yet
- Primary Pulmonary TuberculosisDocument4 pagesPrimary Pulmonary TuberculosisdocdorkmeNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument14 pagesChronic Obstructive Pulmonary DiseaseJohn Christopher LucesNo ratings yet
- Clinical ExDocument123 pagesClinical ExDeepti ChaharNo ratings yet
- ENT Quick ReviewDocument6 pagesENT Quick ReviewWade100% (1)
- Sleep Apnoea - Prof - DR K.K.PDocument44 pagesSleep Apnoea - Prof - DR K.K.PjialeongNo ratings yet
- HYPOCALCEMIADocument27 pagesHYPOCALCEMIAJeffri SetiawanNo ratings yet
- B4 DyspneaDocument100 pagesB4 DyspneaAnonymous HH3c17osNo ratings yet
- Asthma DR Moses KazevuDocument25 pagesAsthma DR Moses KazevuMoses Jr KazevuNo ratings yet
- Cor PulmonaleDocument8 pagesCor PulmonaleAymen OmerNo ratings yet
- Lung AbcessDocument12 pagesLung AbcessABI OFFICIALNo ratings yet
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- 8 Signs and Symptoms of Vitamin D DeficiencyDocument14 pages8 Signs and Symptoms of Vitamin D DeficiencyM. K. HossainNo ratings yet
- Medical MCQ Center Tuberculosis MCQsDocument4 pagesMedical MCQ Center Tuberculosis MCQsBanu KubendiranNo ratings yet
- Sample CollectionDocument8 pagesSample CollectionwillowmaecayabyabNo ratings yet
- Prestasi Akademik 3Document6 pagesPrestasi Akademik 3Jr SparkNo ratings yet
- Expanded HIV Pre-Exposure Prophylaxis PrEP ImplemeDocument11 pagesExpanded HIV Pre-Exposure Prophylaxis PrEP ImplemeLuana MarinsNo ratings yet
- Stay Healthy During, and Be Safe After Remember These Phrases. These Will Assist Us andDocument2 pagesStay Healthy During, and Be Safe After Remember These Phrases. These Will Assist Us andAlthea Mitzi DimafelixNo ratings yet
- C A Tel A T : CO /vac Up A S: 1st Topic: Cabuyao Hotline NumbersDocument6 pagesC A Tel A T : CO /vac Up A S: 1st Topic: Cabuyao Hotline NumbersKatherine Gayle GuiaNo ratings yet
- Lakhovsky Info and ResultDocument6 pagesLakhovsky Info and ResultfUnCk googlet spyNo ratings yet
- Safe and Clean Environment in Hospital 237640255Document38 pagesSafe and Clean Environment in Hospital 237640255Akanksha SinghNo ratings yet
- Sample Qns 18Document15 pagesSample Qns 18kapingaofficialNo ratings yet
- Complete Textbook of Phlebotomy 5th Edition by Hoeltke ISBN Solution ManualDocument13 pagesComplete Textbook of Phlebotomy 5th Edition by Hoeltke ISBN Solution Manualsook100% (27)
- Assessment Form CRF Dwinda Maulina RahmaDocument4 pagesAssessment Form CRF Dwinda Maulina RahmaolinNo ratings yet
- NCP Deficient Fluid VolumeDocument5 pagesNCP Deficient Fluid VolumeCHRISTINE GRACE ELLONo ratings yet
- Covid19 and Its Global Impact On Food and AgricultureDocument4 pagesCovid19 and Its Global Impact On Food and AgricultureFrank Ian EscorsaNo ratings yet
- Distribusi Gingivitis Pada Pasien SkizofreniaDocument6 pagesDistribusi Gingivitis Pada Pasien SkizofreniafaniaNo ratings yet
- Sustainable Safety in Cemeteries - Andre Van Den BergDocument45 pagesSustainable Safety in Cemeteries - Andre Van Den BergMackoy MarasiganNo ratings yet
- Case Report: Urachal Adenocarcinoma: A Case Report With Key Imaging Findings and Radiologic-Pathologic CorrelationDocument6 pagesCase Report: Urachal Adenocarcinoma: A Case Report With Key Imaging Findings and Radiologic-Pathologic Correlationchristian hansNo ratings yet
- Alkan Health Science Business and Technology CollegeDocument62 pagesAlkan Health Science Business and Technology CollegejibrNo ratings yet
- Cerebral Palsy ChildDocument14 pagesCerebral Palsy Childpriyadarade97No ratings yet
- Funda RLEDocument29 pagesFunda RLECharisse CaydanNo ratings yet
- Clinical Naturopathy - Sample ChapterDocument78 pagesClinical Naturopathy - Sample ChapterKamal Gowda70% (10)
- Final Pit 2020 IsbnDocument20 pagesFinal Pit 2020 IsbnYohanes FirmansyahNo ratings yet
- Diagnosa IcdDocument13 pagesDiagnosa IcdAnnisa Putri AbisekaNo ratings yet
- Weekly Influenza Report Week Ending Saturday October 10 2020Document9 pagesWeekly Influenza Report Week Ending Saturday October 10 2020KATVNo ratings yet
- Review Article: Understanding The Mechanisms of Proteinuria: Therapeutic ImplicationsDocument14 pagesReview Article: Understanding The Mechanisms of Proteinuria: Therapeutic ImplicationsNadya SandyaNo ratings yet
- EHRASurvey ManagementofAFinCKDPatients FinalManuscriptDocument10 pagesEHRASurvey ManagementofAFinCKDPatients FinalManuscriptLabontu IustinaNo ratings yet
- 418-M3-Cu14 Nursing Care of Clients in Emergency Situations 1 - AbcsDocument9 pages418-M3-Cu14 Nursing Care of Clients in Emergency Situations 1 - AbcsDanica FrancoNo ratings yet
- Introductory Medical Surgical Nursing 10Th Edition Timby Test Bank Full Chapter PDFDocument17 pagesIntroductory Medical Surgical Nursing 10Th Edition Timby Test Bank Full Chapter PDFmrissaancun100% (11)
- Clinical Spotlight Review - Management of Choledocholithiasis - A SAGES PublicationDocument15 pagesClinical Spotlight Review - Management of Choledocholithiasis - A SAGES PublicationMu TelaNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policyanil sangwanNo ratings yet