Download as ppt, pdf, or txt
You might also like
- Community Diagnosis - StrategyDocument18 pagesCommunity Diagnosis - StrategyAjao Rukayat100% (1)
- Historical Perspective of Environmental HealthDocument11 pagesHistorical Perspective of Environmental HealthMatt67% (3)
- SYLLABUS Nurse Grade-II ExamDocument3 pagesSYLLABUS Nurse Grade-II ExamDivyesh PatelNo ratings yet
- Hydrolysis of Nucleic AcidsDocument7 pagesHydrolysis of Nucleic Acidskeepersake81% (16)
- Primary Health CareDocument68 pagesPrimary Health CareShena Mie Adis Vallecera100% (1)
- Primary Health CareDocument30 pagesPrimary Health CareSan SiddzNo ratings yet
- Determinants of Health: by Sujatha JayabalDocument44 pagesDeterminants of Health: by Sujatha JayabalSujatha J JayabalNo ratings yet
- 04 IPHS Primary Health CentreDocument20 pages04 IPHS Primary Health CentreKailash NagarNo ratings yet
- Department of HealthDocument9 pagesDepartment of HealthRosely M. MalloNo ratings yet
- Components of NRHM 1Document36 pagesComponents of NRHM 1Jeba Powlose SisilyNo ratings yet
- Apollo Hospitals Medical TourismDocument26 pagesApollo Hospitals Medical TourismDeepak SinghNo ratings yet
- Review OF Rmnch+A, RCH Including Other Maternal Health Programme and IdspDocument73 pagesReview OF Rmnch+A, RCH Including Other Maternal Health Programme and IdspGargi pandeyNo ratings yet
- Mother and Child Health Part 2.Ppt FinalDocument102 pagesMother and Child Health Part 2.Ppt FinalJohann Dexter Malimban Glorioso100% (1)
- National AIDS Control Programme: For Final Year BAMS StudentsDocument7 pagesNational AIDS Control Programme: For Final Year BAMS StudentsViswa GiriNo ratings yet
- Ayushman Bharat YojanaDocument28 pagesAyushman Bharat YojanaParth VasaveNo ratings yet
- National Health Policy and PlanDocument92 pagesNational Health Policy and PlanChetan BhattaNo ratings yet
- Introduction To Public HealthDocument24 pagesIntroduction To Public HealthGaurav PuriNo ratings yet
- Health Administration NewDocument10 pagesHealth Administration NewjessyNo ratings yet
- Drug Induced Pulmonary DiseasesDocument26 pagesDrug Induced Pulmonary Diseaseswiona morasNo ratings yet
- Functions of Public HealthDocument30 pagesFunctions of Public Healthteklay100% (1)
- Maternal and Child Health ServicesDocument45 pagesMaternal and Child Health Servicesshijuvarghesepg0% (1)
- Understanding Quality and Satisfaction in Public Hospital Services - A Nationwide Inpatient Survey in GreeceDocument6 pagesUnderstanding Quality and Satisfaction in Public Hospital Services - A Nationwide Inpatient Survey in GreeceShimaditya NuraeniNo ratings yet
- HPMI For Print April.11Document118 pagesHPMI For Print April.11EzanaNo ratings yet
- History, Evolution & Classification of HospitalsDocument10 pagesHistory, Evolution & Classification of HospitalsAnonymous ibmeej9100% (1)
- JSS Hospital ReportDocument16 pagesJSS Hospital ReportVarg DurielNo ratings yet
- Knowledge Attitude and Practice of Mothers Regarding Weaning in Rular Community LahoreDocument6 pagesKnowledge Attitude and Practice of Mothers Regarding Weaning in Rular Community LahorePriyanjali SainiNo ratings yet
- TQM MbaDocument143 pagesTQM Mbaponnasaikumar100% (1)
- Concept of PHCDocument78 pagesConcept of PHCsunielgowdaNo ratings yet
- CHN (1) Community Health NursingDocument1 pageCHN (1) Community Health NursingImation DataNo ratings yet
- Npcdcs 180920052508 PDFDocument34 pagesNpcdcs 180920052508 PDFNeethu VincentNo ratings yet
- TDM of DigoxinDocument13 pagesTDM of DigoxinMounika16 PedamalluNo ratings yet
- Alma Ata DeclarationDocument21 pagesAlma Ata DeclarationJim Christian EllaserNo ratings yet
- Lesson 5 - Electronic Health Record and Clinical Informatics - PPT StudentDocument42 pagesLesson 5 - Electronic Health Record and Clinical Informatics - PPT Studentbeer_ettaaNo ratings yet
- Community PharmacyDocument90 pagesCommunity Pharmacyadili soohaaNo ratings yet
- CM 7.3 Source of Epidemiological DataDocument16 pagesCM 7.3 Source of Epidemiological DataSonal DayamaNo ratings yet
- Health Promotion and Disease PreventionDocument21 pagesHealth Promotion and Disease PreventionHajra MirzaNo ratings yet
- Port Health - OverviewDocument30 pagesPort Health - OverviewKay BristolNo ratings yet
- Indian Public Health Standard IIDocument19 pagesIndian Public Health Standard IIKailash NagarNo ratings yet
- National Aids Control Programme Phase-Iv Current Status and Critical AppraisalDocument71 pagesNational Aids Control Programme Phase-Iv Current Status and Critical AppraisalNeethu Vincent100% (1)
- Management Information System in HealthcareDocument3 pagesManagement Information System in HealthcareThirdy AquinoNo ratings yet
- Basic Public Health (1) - MergedDocument89 pagesBasic Public Health (1) - Mergedrimsha tariqNo ratings yet
- Indian Public Health Standards (IPHS)Document2 pagesIndian Public Health Standards (IPHS)Nikcy N M NicklavoseNo ratings yet
- Pharmaceutical CareDocument7 pagesPharmaceutical Caresomayya waliNo ratings yet
- Health Care Delivery SystemDocument65 pagesHealth Care Delivery SystemTamanna RedhuNo ratings yet
- Introduction of Public Health Nursing: Mr. Kailash NagarDocument37 pagesIntroduction of Public Health Nursing: Mr. Kailash NagarKailash NagarNo ratings yet
- NHSRC - Operational Guidelines On Maternal and Newborn HealthDocument46 pagesNHSRC - Operational Guidelines On Maternal and Newborn HealthNational Child Health Resource Centre (NCHRC)No ratings yet
- Complete CHEW CurriculumDocument162 pagesComplete CHEW CurriculumAbdulhamidNo ratings yet
- Current Health TechnologyDocument47 pagesCurrent Health TechnologyDolisha WarbiNo ratings yet
- Chapter 5 EpidemiologyDocument7 pagesChapter 5 EpidemiologyJohn Rick OrineNo ratings yet
- National Health Programmes: Dr. M.L. SiddarajuDocument40 pagesNational Health Programmes: Dr. M.L. SiddarajuGaoudam NatarajanNo ratings yet
- Primary Health Care: Dr. Ariful Bari ChowdhuryDocument39 pagesPrimary Health Care: Dr. Ariful Bari ChowdhuryTanni ChowdhuryNo ratings yet
- National Health Policy 2009 PakistanDocument38 pagesNational Health Policy 2009 PakistanAbdul Wahab KhanNo ratings yet
- Primary Health CareDocument2 pagesPrimary Health CareShamsa RiazNo ratings yet
- ErhunDocument46 pagesErhunOlufemi OmotayoNo ratings yet
- Unit 1 PPT FinalDocument9 pagesUnit 1 PPT FinalRochelle Anne Abad Banda100% (1)
- Trainin On Compassionate, Respectful and Caring Health ProfessionalsDocument21 pagesTrainin On Compassionate, Respectful and Caring Health ProfessionalsnibretzwNo ratings yet
- Health Care SystemDocument13 pagesHealth Care SystemMarie MayNo ratings yet
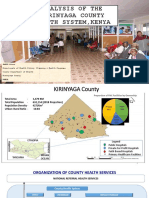
- Analysis of The Kirinyaga County Health System - Esbon - GakuuDocument18 pagesAnalysis of The Kirinyaga County Health System - Esbon - Gakuuesbon gakuu100% (1)
- Community Diagnosis - Ms. Dorothy - 13476Document91 pagesCommunity Diagnosis - Ms. Dorothy - 13476Janet MbandiNo ratings yet
- Chronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesFrom EverandChronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Lesson Plan Sience - Body PartsDocument4 pagesLesson Plan Sience - Body Partsapi-307376252No ratings yet
- Organic Halides Introduction Class-1 NotesDocument15 pagesOrganic Halides Introduction Class-1 Notessiddhartha singhNo ratings yet
- Microsoft Project TOCDocument5 pagesMicrosoft Project TOCali_zulfikarNo ratings yet
- PTS MATH GRADE 3 ICP (2022-2023) - Abidah FixDocument4 pagesPTS MATH GRADE 3 ICP (2022-2023) - Abidah FixAnita Noor Maidah S.Pd.i. SD Lab UMNo ratings yet
- EN Subiecte Locala 19-20 GIMNAZIU 5-8 A-BDocument16 pagesEN Subiecte Locala 19-20 GIMNAZIU 5-8 A-BSpiridon AndreeaNo ratings yet
- 21CC 4 U6Document10 pages21CC 4 U6Adrian Spanu100% (1)
- Ultrasonic InterferometerDocument22 pagesUltrasonic InterferometerakshatguptaNo ratings yet
- Health The Basics 11th Edition Donatelle Test BankDocument19 pagesHealth The Basics 11th Edition Donatelle Test BankJosephWilliamsinaom100% (6)
- Explosion Protection - E PDFDocument7 pagesExplosion Protection - E PDFAPCANo ratings yet
- 84501-9200-9L-008 Rev-0 Technical Inspection Services Company Final Documentation RequirementsDocument7 pages84501-9200-9L-008 Rev-0 Technical Inspection Services Company Final Documentation RequirementsPeni M. SaptoargoNo ratings yet
- Revisit of Harriott's Method For Process ControlDocument3 pagesRevisit of Harriott's Method For Process ControlkiddhoNo ratings yet
- Tut Sheet7Document2 pagesTut Sheet7Ekta SharmaNo ratings yet
- BNVD Eaufrance Metadonnees Vente 20230130Document16 pagesBNVD Eaufrance Metadonnees Vente 20230130moussaouiNo ratings yet
- DLL Mother TongueDocument41 pagesDLL Mother TongueMarxPascualBlancoNo ratings yet
- Sandy Point Brochure 2016Document7 pagesSandy Point Brochure 2016miller999No ratings yet
- (LN) Orc Eroica - Volume 01 (YP)Document282 pages(LN) Orc Eroica - Volume 01 (YP)FBINo ratings yet
- Onco, TSG & CancerDocument8 pagesOnco, TSG & Cancersumera120488No ratings yet
- Alcantara - Module 10 - 2ged SS-03Document2 pagesAlcantara - Module 10 - 2ged SS-03Janine AlcantaraNo ratings yet
- Grade 7 Lesson: ReproductionDocument4 pagesGrade 7 Lesson: ReproductionJoedelyn Wagas100% (2)
- KISI USP INGGRIS Kelas 12Document39 pagesKISI USP INGGRIS Kelas 12Deny Cahyo SaputroNo ratings yet
- WRAP - Case Study - Aggregates - The Channel Tunnel Rail LinkDocument2 pagesWRAP - Case Study - Aggregates - The Channel Tunnel Rail LinkFatmah El WardagyNo ratings yet
- Quisumbing Vs MERALCODocument1 pageQuisumbing Vs MERALCORiss GammadNo ratings yet
- Summary of Current Charges (RS) : Talk To Us SMSDocument13 pagesSummary of Current Charges (RS) : Talk To Us SMSBrandon FloresNo ratings yet
- 'Beware of Being Burgoyned.': Marching Toward Monmouth, Delaware River To Freehold, 18 To 27 June 1778Document35 pages'Beware of Being Burgoyned.': Marching Toward Monmouth, Delaware River To Freehold, 18 To 27 June 1778John U. Rees100% (1)
- Experiencing Postsocialist CapitalismDocument251 pagesExperiencing Postsocialist CapitalismjelisNo ratings yet
- Mapeh GR9 First Quarter ReviewerDocument8 pagesMapeh GR9 First Quarter ReviewerRalph Emerson SantillanNo ratings yet
- Safety Manual (B-80687EN 10)Document35 pagesSafety Manual (B-80687EN 10)Jander Luiz TomaziNo ratings yet
- Asset Accounting (J62) - Process DiagramsDocument8 pagesAsset Accounting (J62) - Process DiagramsMohammed Nawaz ShariffNo ratings yet
- Certificate ASHWINIDocument4 pagesCertificate ASHWINIbloodspray167No ratings yet