
TDM Dan Rancangan Aturan Dosis
TDM Dan Rancangan Aturan Dosis
You might also like
- Test Bank For Medical Surgical Nursing Concepts and Practice 1st Edition by DewitDocument9 pagesTest Bank For Medical Surgical Nursing Concepts and Practice 1st Edition by Dewiteric100% (6)
- Nursing Care Plan For DysmenorrheaDocument3 pagesNursing Care Plan For DysmenorrheaMarife Lipana Reyes73% (22)
- Hospital Management SystemDocument20 pagesHospital Management SystempavanNo ratings yet
- NCP For HypertensionDocument1 pageNCP For HypertensionChristian Daayata0% (1)
- Materi MPPC XXXDocument22 pagesMateri MPPC XXXEther Manuputty II100% (6)
- Causes and Effects of Teenage Pregnancy Among The Female Students and Its Effect On Academic PerformanceDocument12 pagesCauses and Effects of Teenage Pregnancy Among The Female Students and Its Effect On Academic Performancegrossarchive75% (8)
- Disusun Oleh: WIDI TASTARI (16330050) : Farmakoterapi 1 Dosen: Okpri Meila, M.Farm., AptDocument18 pagesDisusun Oleh: WIDI TASTARI (16330050) : Farmakoterapi 1 Dosen: Okpri Meila, M.Farm., AptEnsiNo ratings yet
- Msds AgitaDocument6 pagesMsds Agitaika setiawatiNo ratings yet
- Pengelolaan Dan Penggunaan Obat Di Rumah SakitDocument30 pagesPengelolaan Dan Penggunaan Obat Di Rumah SakitkuronohanaNo ratings yet
- 01 C & D Latar Belakang GPPDocument38 pages01 C & D Latar Belakang GPPPrisma TridaNo ratings yet
- Farmasi Rumah SakitDocument97 pagesFarmasi Rumah SakitkuronohanaNo ratings yet
- GastroparesisDocument7 pagesGastroparesisapi-548943629No ratings yet
- Neuropathy: Departemen Neurologi FK Usu/ Rsup H. Adam Malik MedanDocument41 pagesNeuropathy: Departemen Neurologi FK Usu/ Rsup H. Adam Malik MedanHatta Diana TariganNo ratings yet
- AntihistaminDocument44 pagesAntihistaminDWI RAHMA HALIDANo ratings yet
- Farmakologi Antiagina TTMDocument83 pagesFarmakologi Antiagina TTMEpha Lumban GaolNo ratings yet
- Renal PharmacologyDocument52 pagesRenal PharmacologyashrafNo ratings yet
- FARMAKOEKONOMI1Document38 pagesFARMAKOEKONOMI1AbnerDNeroNo ratings yet
- Farmakoterapi Pada LansiaDocument29 pagesFarmakoterapi Pada LansiaPuterinugraha Wanca ApatyaNo ratings yet
- antiHIPERTENSI 2020Document88 pagesantiHIPERTENSI 2020nabila fikriNo ratings yet
- Depart. Farmakologi Dan Terapeutik: Universitas Sumatera Utara-MedanDocument19 pagesDepart. Farmakologi Dan Terapeutik: Universitas Sumatera Utara-MedanMasyithah TetaNo ratings yet
- HAM Elektrolit KonsentratDocument52 pagesHAM Elektrolit KonsentratNuke Candra DestianNo ratings yet
- Hasyim Kasim: Nephrology and Hypertension Division, Department of Internal Medicine Medical Faculty Hasanuddin UniversityDocument51 pagesHasyim Kasim: Nephrology and Hypertension Division, Department of Internal Medicine Medical Faculty Hasanuddin UniversityMuhammad Yasdar BahriNo ratings yet
- Drug Utilization Study (Dus)Document17 pagesDrug Utilization Study (Dus)Arif Budiman100% (1)
- (A) Pengembangan Obat - OBAT BIOLOGI - Ana Indrayati PDFDocument105 pages(A) Pengembangan Obat - OBAT BIOLOGI - Ana Indrayati PDFNugroho Wisnu PutroNo ratings yet
- Farmakoterapi AntihipertensiDocument37 pagesFarmakoterapi AntihipertensipkmbangilNo ratings yet
- Maya Septriana S.Si., Apt., M.SiDocument18 pagesMaya Septriana S.Si., Apt., M.SiNur Ima ErvianaNo ratings yet
- Prescribing Antipsychotics in Geriatric Patients:: First of 3 PartsDocument8 pagesPrescribing Antipsychotics in Geriatric Patients:: First of 3 PartsAlexRázuri100% (1)
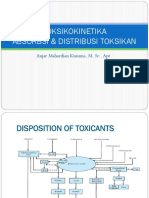
- Toksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptDocument51 pagesToksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptRossy OchieNo ratings yet
- Kirim Ukai HipertensiDocument18 pagesKirim Ukai HipertensiBobbyGunarsoNo ratings yet
- I. Farmakoterapi RasionalDocument24 pagesI. Farmakoterapi RasionalAthirah M.NoerNo ratings yet
- Managing Drug Suply ISTNDocument16 pagesManaging Drug Suply ISTNIndra PratamaNo ratings yet
- Implementasi Metode Kaizen Terhadap Kepuasan Pasien Di Instalasi Farmasi RuDocument6 pagesImplementasi Metode Kaizen Terhadap Kepuasan Pasien Di Instalasi Farmasi RuEndai FajarNo ratings yet
- Farmakoepidemiologi 2018 UmmDocument23 pagesFarmakoepidemiologi 2018 UmmSeptiani Ayu100% (1)
- Clinical Pharmacy The KidnyDocument34 pagesClinical Pharmacy The KidnyAta07No ratings yet
- Obat Saluran Cerna: Anjar Mahardian Kusuma, M. SC., AptDocument27 pagesObat Saluran Cerna: Anjar Mahardian Kusuma, M. SC., AptanikNo ratings yet
- Asuhan Kefarmasian: Ahmad SalehDocument45 pagesAsuhan Kefarmasian: Ahmad SalehDjunaiddin FarmasiNo ratings yet
- Drug Related ProblemDocument13 pagesDrug Related ProblemLinda Yuni LestariNo ratings yet
- Hipertensi: Dr. Made Winatra Satya PutraDocument16 pagesHipertensi: Dr. Made Winatra Satya PutraMade Winatra Satya PutraNo ratings yet
- Standar Operasional Prosedur Kids Amp Baby SpaDocument34 pagesStandar Operasional Prosedur Kids Amp Baby SpaFegi mentari putrierlinaNo ratings yet
- Beyond-Use-DateDocument9 pagesBeyond-Use-DateAnidraqif Hastina100% (1)
- Farmakokinetik Dasar At14sDocument42 pagesFarmakokinetik Dasar At14sElfiana IfaNo ratings yet
- Hipertensi 2Document43 pagesHipertensi 2Sri AfniNo ratings yet
- Pengantar Farmakoterapi Penyakit InfeksiDocument27 pagesPengantar Farmakoterapi Penyakit InfeksiAlunaficha Melody KiraniaNo ratings yet
- Toxicology: Clinical Chemistry Iii LectureDocument42 pagesToxicology: Clinical Chemistry Iii LectureMaria Cecilia FloresNo ratings yet
- 275 280 Drug Related Problems Antipsikotik Pada Pasien Skizofrenia PDFDocument6 pages275 280 Drug Related Problems Antipsikotik Pada Pasien Skizofrenia PDFtiarasrisudarsihNo ratings yet
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocument3 pagesGERD Algorithm Review Definition and Pathophysiology: NO YESdianyNo ratings yet
- A.2 Kesesuaian Penggunaan Obat Dengan Formularium Rumah SakitDocument14 pagesA.2 Kesesuaian Penggunaan Obat Dengan Formularium Rumah SakitRida NurulNo ratings yet
- Journal Medicinus April 2021Document80 pagesJournal Medicinus April 2021Yuliastuti RahayuNo ratings yet
- Biliary Tract Dis Pancreatitis 2015Document143 pagesBiliary Tract Dis Pancreatitis 2015eiad-mahmoudNo ratings yet
- Weeek 1Document29 pagesWeeek 1Alvin De lunaNo ratings yet
- Pendekatan SOAP Farmasi KlinikDocument40 pagesPendekatan SOAP Farmasi KlinikmadeNo ratings yet
- Medication Error-Hisfarmasi PresentationDocument102 pagesMedication Error-Hisfarmasi PresentationLaura Khristiani MarbunNo ratings yet
- HYPERLIPIDEMIADocument11 pagesHYPERLIPIDEMIAFina Ahmad FitrianaNo ratings yet
- CV Tri Murti AndayaniDocument7 pagesCV Tri Murti AndayaniAmalia UlfaNo ratings yet
- Chrono Pharmaco LDocument46 pagesChrono Pharmaco LJaved AliNo ratings yet
- Mineral Homeostasis BoneDocument20 pagesMineral Homeostasis BoneSawsan Z. JwaiedNo ratings yet
- Drug Interaction Report PDFDocument111 pagesDrug Interaction Report PDFbaerbaNo ratings yet
- Case-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Document53 pagesCase-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Ditia RahimNo ratings yet
- Bioavailabilitas & BioekivalenDocument27 pagesBioavailabilitas & Bioekivalendonghaesayangela100% (1)
- Therapeutic Drug Monitoring: RVS Chaitanya KoppalaDocument33 pagesTherapeutic Drug Monitoring: RVS Chaitanya KoppalaDr. Raghavendra Kumar Gunda100% (1)
- Therapeutic Drug MonitoringDocument50 pagesTherapeutic Drug MonitoringKapusetti Vanaja0% (1)
- TDM ClassDocument26 pagesTDM Classsayan mandalNo ratings yet
- TDM ClassDocument30 pagesTDM ClassKettavan DaNo ratings yet
- Therapeutic Drug Monitoring: Saeed Alqahtani, Pharmd, PHDDocument78 pagesTherapeutic Drug Monitoring: Saeed Alqahtani, Pharmd, PHDAnonymous hF5zAdvwCC50% (2)
- Dr. Ruth NamyaloDocument62 pagesDr. Ruth NamyaloHarun MohamedNo ratings yet
- Nama (Diisi Dengan Nama Peserta) No - Identitas (Diisi Dengan NIP/NRP/NPP/NIK) Jenis - Kelamin (Pilih Satu)Document23 pagesNama (Diisi Dengan Nama Peserta) No - Identitas (Diisi Dengan NIP/NRP/NPP/NIK) Jenis - Kelamin (Pilih Satu)adelin ransunNo ratings yet
- OtodexDocument2 pagesOtodexadelin ransunNo ratings yet
- Lila Bintarizki Daftar PustakaDocument2 pagesLila Bintarizki Daftar Pustakaadelin ransunNo ratings yet
- Association of Pre-Antiretroviral Treatment Body Mass Index With Cd4 T-Lymphocyte Immune Reconstitution Among HIV-Infected Adults and AdolescentsDocument8 pagesAssociation of Pre-Antiretroviral Treatment Body Mass Index With Cd4 T-Lymphocyte Immune Reconstitution Among HIV-Infected Adults and Adolescentsadelin ransunNo ratings yet
- Ijphcs: A Comparison of Hiv/Aids Health Policy in Selected Developed and Developing CountriesDocument14 pagesIjphcs: A Comparison of Hiv/Aids Health Policy in Selected Developed and Developing Countriesadelin ransunNo ratings yet
- 13B Week 1 NRG 303 Trends and IssuesDocument7 pages13B Week 1 NRG 303 Trends and IssuesERAN MARK ROJASNo ratings yet
- Opium: Retail and Wholesale Prices and Purity Levels: Breakdown by Drug, Region and Country or TerritoryDocument19 pagesOpium: Retail and Wholesale Prices and Purity Levels: Breakdown by Drug, Region and Country or TerritoryboombaNo ratings yet
- Drug Desensitization PenicillinDocument19 pagesDrug Desensitization PenicillinpdahlianaNo ratings yet
- Audiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The LiteratureDocument12 pagesAudiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The Literaturericardorojas2403No ratings yet
- Medicaid Adult Dental Benefits Overview Appendix - 091519Document6 pagesMedicaid Adult Dental Benefits Overview Appendix - 091519carzhallNo ratings yet
- Module 5 Lec 3Document17 pagesModule 5 Lec 3Shivang DhoundiyalNo ratings yet
- Pro - Seks BebasDocument12 pagesPro - Seks BebasMOCH. FIKRI KHAUTALNo ratings yet
- Construction Safety and Health ProgramDocument63 pagesConstruction Safety and Health ProgramAlmher RemolloNo ratings yet
- Guidelines For Maternity Care 2016Document148 pagesGuidelines For Maternity Care 2016MjunjuNo ratings yet
- ZEBRA Pen SDS R 301Document6 pagesZEBRA Pen SDS R 301chusqueteNo ratings yet
- HMO Proposal For Individual Family Account REGULAR-UPDATED AS OF JULY 2...Document11 pagesHMO Proposal For Individual Family Account REGULAR-UPDATED AS OF JULY 2...Arron BuenavistaNo ratings yet
- Family TIES Resource Directory 2020Document218 pagesFamily TIES Resource Directory 2020juanmiguelperez20kNo ratings yet
- Medial Epicondylitis (Golfer's Elbow) - Shoulder & Elbow - OrthobulletsDocument8 pagesMedial Epicondylitis (Golfer's Elbow) - Shoulder & Elbow - OrthobulletsSylvia GraceNo ratings yet
- Material Safety Data Sheet Hyperplast ES901: 1: Product and Company IdentificationDocument4 pagesMaterial Safety Data Sheet Hyperplast ES901: 1: Product and Company IdentificationStewart CredoNo ratings yet
- Swimmer Syndrome in WildlifeDocument2 pagesSwimmer Syndrome in WildlifeALicjaNo ratings yet
- Talacogon - 4th Quarter PresentationDocument48 pagesTalacogon - 4th Quarter PresentationRomeo AbrigoNo ratings yet
- The Infant of An Addicted MotherDocument15 pagesThe Infant of An Addicted Mothernursereview100% (8)
- Health Education ProcessDocument25 pagesHealth Education Processdailygrind00011No ratings yet
- Abdominal Acupuncture For DepressionDocument35 pagesAbdominal Acupuncture For DepressionAGNESE YOLOTZIN OLIVERA TORO REYESNo ratings yet
- Eas 749 2010 Brown Sugar SpecificationDocument10 pagesEas 749 2010 Brown Sugar SpecificationFelix MwandukaNo ratings yet
- Student Stress ChecklistDocument2 pagesStudent Stress ChecklistAlaiza Maas LanonNo ratings yet
- Patient SatisfactionDocument6 pagesPatient SatisfactionDon Chiaw ManongdoNo ratings yet
- A Guide To The Safe Storage of Explosive MaterialsDocument27 pagesA Guide To The Safe Storage of Explosive MaterialsPrecision Blasting LLCNo ratings yet
- 2016practical Urinalysis in The Cat 1Document13 pages2016practical Urinalysis in The Cat 1Danahi Carrizo BarahonaNo ratings yet
- 07 One Missing StrokeDocument10 pages07 One Missing StrokeMiura AngNo ratings yet





























































































Download as pptx, pdf, or txt
You might also like
- Test Bank For Medical Surgical Nursing Concepts and Practice 1st Edition by DewitDocument9 pagesTest Bank For Medical Surgical Nursing Concepts and Practice 1st Edition by Dewiteric100% (6)
- Nursing Care Plan For DysmenorrheaDocument3 pagesNursing Care Plan For DysmenorrheaMarife Lipana Reyes73% (22)
- Hospital Management SystemDocument20 pagesHospital Management SystempavanNo ratings yet
- NCP For HypertensionDocument1 pageNCP For HypertensionChristian Daayata0% (1)
- Materi MPPC XXXDocument22 pagesMateri MPPC XXXEther Manuputty II100% (6)
- Causes and Effects of Teenage Pregnancy Among The Female Students and Its Effect On Academic PerformanceDocument12 pagesCauses and Effects of Teenage Pregnancy Among The Female Students and Its Effect On Academic Performancegrossarchive75% (8)
- Disusun Oleh: WIDI TASTARI (16330050) : Farmakoterapi 1 Dosen: Okpri Meila, M.Farm., AptDocument18 pagesDisusun Oleh: WIDI TASTARI (16330050) : Farmakoterapi 1 Dosen: Okpri Meila, M.Farm., AptEnsiNo ratings yet
- Msds AgitaDocument6 pagesMsds Agitaika setiawatiNo ratings yet
- Pengelolaan Dan Penggunaan Obat Di Rumah SakitDocument30 pagesPengelolaan Dan Penggunaan Obat Di Rumah SakitkuronohanaNo ratings yet
- 01 C & D Latar Belakang GPPDocument38 pages01 C & D Latar Belakang GPPPrisma TridaNo ratings yet
- Farmasi Rumah SakitDocument97 pagesFarmasi Rumah SakitkuronohanaNo ratings yet
- GastroparesisDocument7 pagesGastroparesisapi-548943629No ratings yet
- Neuropathy: Departemen Neurologi FK Usu/ Rsup H. Adam Malik MedanDocument41 pagesNeuropathy: Departemen Neurologi FK Usu/ Rsup H. Adam Malik MedanHatta Diana TariganNo ratings yet
- AntihistaminDocument44 pagesAntihistaminDWI RAHMA HALIDANo ratings yet
- Farmakologi Antiagina TTMDocument83 pagesFarmakologi Antiagina TTMEpha Lumban GaolNo ratings yet
- Renal PharmacologyDocument52 pagesRenal PharmacologyashrafNo ratings yet
- FARMAKOEKONOMI1Document38 pagesFARMAKOEKONOMI1AbnerDNeroNo ratings yet
- Farmakoterapi Pada LansiaDocument29 pagesFarmakoterapi Pada LansiaPuterinugraha Wanca ApatyaNo ratings yet
- antiHIPERTENSI 2020Document88 pagesantiHIPERTENSI 2020nabila fikriNo ratings yet
- Depart. Farmakologi Dan Terapeutik: Universitas Sumatera Utara-MedanDocument19 pagesDepart. Farmakologi Dan Terapeutik: Universitas Sumatera Utara-MedanMasyithah TetaNo ratings yet
- HAM Elektrolit KonsentratDocument52 pagesHAM Elektrolit KonsentratNuke Candra DestianNo ratings yet
- Hasyim Kasim: Nephrology and Hypertension Division, Department of Internal Medicine Medical Faculty Hasanuddin UniversityDocument51 pagesHasyim Kasim: Nephrology and Hypertension Division, Department of Internal Medicine Medical Faculty Hasanuddin UniversityMuhammad Yasdar BahriNo ratings yet
- Drug Utilization Study (Dus)Document17 pagesDrug Utilization Study (Dus)Arif Budiman100% (1)
- (A) Pengembangan Obat - OBAT BIOLOGI - Ana Indrayati PDFDocument105 pages(A) Pengembangan Obat - OBAT BIOLOGI - Ana Indrayati PDFNugroho Wisnu PutroNo ratings yet
- Farmakoterapi AntihipertensiDocument37 pagesFarmakoterapi AntihipertensipkmbangilNo ratings yet
- Maya Septriana S.Si., Apt., M.SiDocument18 pagesMaya Septriana S.Si., Apt., M.SiNur Ima ErvianaNo ratings yet
- Prescribing Antipsychotics in Geriatric Patients:: First of 3 PartsDocument8 pagesPrescribing Antipsychotics in Geriatric Patients:: First of 3 PartsAlexRázuri100% (1)
- Toksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptDocument51 pagesToksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptRossy OchieNo ratings yet
- Kirim Ukai HipertensiDocument18 pagesKirim Ukai HipertensiBobbyGunarsoNo ratings yet
- I. Farmakoterapi RasionalDocument24 pagesI. Farmakoterapi RasionalAthirah M.NoerNo ratings yet
- Managing Drug Suply ISTNDocument16 pagesManaging Drug Suply ISTNIndra PratamaNo ratings yet
- Implementasi Metode Kaizen Terhadap Kepuasan Pasien Di Instalasi Farmasi RuDocument6 pagesImplementasi Metode Kaizen Terhadap Kepuasan Pasien Di Instalasi Farmasi RuEndai FajarNo ratings yet
- Farmakoepidemiologi 2018 UmmDocument23 pagesFarmakoepidemiologi 2018 UmmSeptiani Ayu100% (1)
- Clinical Pharmacy The KidnyDocument34 pagesClinical Pharmacy The KidnyAta07No ratings yet
- Obat Saluran Cerna: Anjar Mahardian Kusuma, M. SC., AptDocument27 pagesObat Saluran Cerna: Anjar Mahardian Kusuma, M. SC., AptanikNo ratings yet
- Asuhan Kefarmasian: Ahmad SalehDocument45 pagesAsuhan Kefarmasian: Ahmad SalehDjunaiddin FarmasiNo ratings yet
- Drug Related ProblemDocument13 pagesDrug Related ProblemLinda Yuni LestariNo ratings yet
- Hipertensi: Dr. Made Winatra Satya PutraDocument16 pagesHipertensi: Dr. Made Winatra Satya PutraMade Winatra Satya PutraNo ratings yet
- Standar Operasional Prosedur Kids Amp Baby SpaDocument34 pagesStandar Operasional Prosedur Kids Amp Baby SpaFegi mentari putrierlinaNo ratings yet
- Beyond-Use-DateDocument9 pagesBeyond-Use-DateAnidraqif Hastina100% (1)
- Farmakokinetik Dasar At14sDocument42 pagesFarmakokinetik Dasar At14sElfiana IfaNo ratings yet
- Hipertensi 2Document43 pagesHipertensi 2Sri AfniNo ratings yet
- Pengantar Farmakoterapi Penyakit InfeksiDocument27 pagesPengantar Farmakoterapi Penyakit InfeksiAlunaficha Melody KiraniaNo ratings yet
- Toxicology: Clinical Chemistry Iii LectureDocument42 pagesToxicology: Clinical Chemistry Iii LectureMaria Cecilia FloresNo ratings yet
- 275 280 Drug Related Problems Antipsikotik Pada Pasien Skizofrenia PDFDocument6 pages275 280 Drug Related Problems Antipsikotik Pada Pasien Skizofrenia PDFtiarasrisudarsihNo ratings yet
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocument3 pagesGERD Algorithm Review Definition and Pathophysiology: NO YESdianyNo ratings yet
- A.2 Kesesuaian Penggunaan Obat Dengan Formularium Rumah SakitDocument14 pagesA.2 Kesesuaian Penggunaan Obat Dengan Formularium Rumah SakitRida NurulNo ratings yet
- Journal Medicinus April 2021Document80 pagesJournal Medicinus April 2021Yuliastuti RahayuNo ratings yet
- Biliary Tract Dis Pancreatitis 2015Document143 pagesBiliary Tract Dis Pancreatitis 2015eiad-mahmoudNo ratings yet
- Weeek 1Document29 pagesWeeek 1Alvin De lunaNo ratings yet
- Pendekatan SOAP Farmasi KlinikDocument40 pagesPendekatan SOAP Farmasi KlinikmadeNo ratings yet
- Medication Error-Hisfarmasi PresentationDocument102 pagesMedication Error-Hisfarmasi PresentationLaura Khristiani MarbunNo ratings yet
- HYPERLIPIDEMIADocument11 pagesHYPERLIPIDEMIAFina Ahmad FitrianaNo ratings yet
- CV Tri Murti AndayaniDocument7 pagesCV Tri Murti AndayaniAmalia UlfaNo ratings yet
- Chrono Pharmaco LDocument46 pagesChrono Pharmaco LJaved AliNo ratings yet
- Mineral Homeostasis BoneDocument20 pagesMineral Homeostasis BoneSawsan Z. JwaiedNo ratings yet
- Drug Interaction Report PDFDocument111 pagesDrug Interaction Report PDFbaerbaNo ratings yet
- Case-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Document53 pagesCase-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Ditia RahimNo ratings yet
- Bioavailabilitas & BioekivalenDocument27 pagesBioavailabilitas & Bioekivalendonghaesayangela100% (1)
- Therapeutic Drug Monitoring: RVS Chaitanya KoppalaDocument33 pagesTherapeutic Drug Monitoring: RVS Chaitanya KoppalaDr. Raghavendra Kumar Gunda100% (1)
- Therapeutic Drug MonitoringDocument50 pagesTherapeutic Drug MonitoringKapusetti Vanaja0% (1)
- TDM ClassDocument26 pagesTDM Classsayan mandalNo ratings yet
- TDM ClassDocument30 pagesTDM ClassKettavan DaNo ratings yet
- Therapeutic Drug Monitoring: Saeed Alqahtani, Pharmd, PHDDocument78 pagesTherapeutic Drug Monitoring: Saeed Alqahtani, Pharmd, PHDAnonymous hF5zAdvwCC50% (2)
- Dr. Ruth NamyaloDocument62 pagesDr. Ruth NamyaloHarun MohamedNo ratings yet
- Nama (Diisi Dengan Nama Peserta) No - Identitas (Diisi Dengan NIP/NRP/NPP/NIK) Jenis - Kelamin (Pilih Satu)Document23 pagesNama (Diisi Dengan Nama Peserta) No - Identitas (Diisi Dengan NIP/NRP/NPP/NIK) Jenis - Kelamin (Pilih Satu)adelin ransunNo ratings yet
- OtodexDocument2 pagesOtodexadelin ransunNo ratings yet
- Lila Bintarizki Daftar PustakaDocument2 pagesLila Bintarizki Daftar Pustakaadelin ransunNo ratings yet
- Association of Pre-Antiretroviral Treatment Body Mass Index With Cd4 T-Lymphocyte Immune Reconstitution Among HIV-Infected Adults and AdolescentsDocument8 pagesAssociation of Pre-Antiretroviral Treatment Body Mass Index With Cd4 T-Lymphocyte Immune Reconstitution Among HIV-Infected Adults and Adolescentsadelin ransunNo ratings yet
- Ijphcs: A Comparison of Hiv/Aids Health Policy in Selected Developed and Developing CountriesDocument14 pagesIjphcs: A Comparison of Hiv/Aids Health Policy in Selected Developed and Developing Countriesadelin ransunNo ratings yet
- 13B Week 1 NRG 303 Trends and IssuesDocument7 pages13B Week 1 NRG 303 Trends and IssuesERAN MARK ROJASNo ratings yet
- Opium: Retail and Wholesale Prices and Purity Levels: Breakdown by Drug, Region and Country or TerritoryDocument19 pagesOpium: Retail and Wholesale Prices and Purity Levels: Breakdown by Drug, Region and Country or TerritoryboombaNo ratings yet
- Drug Desensitization PenicillinDocument19 pagesDrug Desensitization PenicillinpdahlianaNo ratings yet
- Audiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The LiteratureDocument12 pagesAudiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The Literaturericardorojas2403No ratings yet
- Medicaid Adult Dental Benefits Overview Appendix - 091519Document6 pagesMedicaid Adult Dental Benefits Overview Appendix - 091519carzhallNo ratings yet
- Module 5 Lec 3Document17 pagesModule 5 Lec 3Shivang DhoundiyalNo ratings yet
- Pro - Seks BebasDocument12 pagesPro - Seks BebasMOCH. FIKRI KHAUTALNo ratings yet
- Construction Safety and Health ProgramDocument63 pagesConstruction Safety and Health ProgramAlmher RemolloNo ratings yet
- Guidelines For Maternity Care 2016Document148 pagesGuidelines For Maternity Care 2016MjunjuNo ratings yet
- ZEBRA Pen SDS R 301Document6 pagesZEBRA Pen SDS R 301chusqueteNo ratings yet
- HMO Proposal For Individual Family Account REGULAR-UPDATED AS OF JULY 2...Document11 pagesHMO Proposal For Individual Family Account REGULAR-UPDATED AS OF JULY 2...Arron BuenavistaNo ratings yet
- Family TIES Resource Directory 2020Document218 pagesFamily TIES Resource Directory 2020juanmiguelperez20kNo ratings yet
- Medial Epicondylitis (Golfer's Elbow) - Shoulder & Elbow - OrthobulletsDocument8 pagesMedial Epicondylitis (Golfer's Elbow) - Shoulder & Elbow - OrthobulletsSylvia GraceNo ratings yet
- Material Safety Data Sheet Hyperplast ES901: 1: Product and Company IdentificationDocument4 pagesMaterial Safety Data Sheet Hyperplast ES901: 1: Product and Company IdentificationStewart CredoNo ratings yet
- Swimmer Syndrome in WildlifeDocument2 pagesSwimmer Syndrome in WildlifeALicjaNo ratings yet
- Talacogon - 4th Quarter PresentationDocument48 pagesTalacogon - 4th Quarter PresentationRomeo AbrigoNo ratings yet
- The Infant of An Addicted MotherDocument15 pagesThe Infant of An Addicted Mothernursereview100% (8)
- Health Education ProcessDocument25 pagesHealth Education Processdailygrind00011No ratings yet
- Abdominal Acupuncture For DepressionDocument35 pagesAbdominal Acupuncture For DepressionAGNESE YOLOTZIN OLIVERA TORO REYESNo ratings yet
- Eas 749 2010 Brown Sugar SpecificationDocument10 pagesEas 749 2010 Brown Sugar SpecificationFelix MwandukaNo ratings yet
- Student Stress ChecklistDocument2 pagesStudent Stress ChecklistAlaiza Maas LanonNo ratings yet
- Patient SatisfactionDocument6 pagesPatient SatisfactionDon Chiaw ManongdoNo ratings yet
- A Guide To The Safe Storage of Explosive MaterialsDocument27 pagesA Guide To The Safe Storage of Explosive MaterialsPrecision Blasting LLCNo ratings yet
- 2016practical Urinalysis in The Cat 1Document13 pages2016practical Urinalysis in The Cat 1Danahi Carrizo BarahonaNo ratings yet
- 07 One Missing StrokeDocument10 pages07 One Missing StrokeMiura AngNo ratings yet