Download as pptx, pdf, or txt
You might also like
- Pediatrics NotesDocument100 pagesPediatrics Notessanflash100% (1)
- Feline Infectious Peritonitis .By SivaDocument20 pagesFeline Infectious Peritonitis .By SivaR SIVA RAMANNo ratings yet
- Gastroenteritis in ChildrenDocument48 pagesGastroenteritis in ChildrenKelsingra FitzChivalry FarseerNo ratings yet
- Diseases of Neonates in AnimalsDocument35 pagesDiseases of Neonates in AnimalshansmeetNo ratings yet
- PD 17 To 21Document148 pagesPD 17 To 21Loai Mohammed IssaNo ratings yet
- Step2 - PediatricsDocument18 pagesStep2 - PediatricsKiran Saini100% (1)
- Nephrotic SyndromeDocument49 pagesNephrotic SyndromeAMA237No ratings yet
- Pediatric Spot Diagnosis: Abdulrahman BashireDocument20 pagesPediatric Spot Diagnosis: Abdulrahman Bashireعبدالرحمن بشير100% (1)
- Lecture-4 Viral GastroenteritisDocument37 pagesLecture-4 Viral GastroenteritislolitlolatNo ratings yet
- By DR - Tosif Ahmad TMO-PediatricsDocument27 pagesBy DR - Tosif Ahmad TMO-PediatricskamalNo ratings yet
- Urinary Tract Infection: Mentor DR - SaralaDocument53 pagesUrinary Tract Infection: Mentor DR - SaralaMimi Suhaini SudinNo ratings yet
- Asculitis Syndromes: Emily B. Martin, MD Rheumatology Board Review April 9, 2008Document54 pagesAsculitis Syndromes: Emily B. Martin, MD Rheumatology Board Review April 9, 2008Miguel M. Melchor RodríguezNo ratings yet
- Oral RevalidaDocument3 pagesOral RevalidaJaye DangoNo ratings yet
- Acute Gastroenteritis in ChildrenDocument64 pagesAcute Gastroenteritis in ChildrenSteven William0% (1)
- Gastroenteritis in Children: Prepared by R. J. C. Manalo, BSN, RN, MNDocument45 pagesGastroenteritis in Children: Prepared by R. J. C. Manalo, BSN, RN, MNHui ChenNo ratings yet
- CMD DBDDocument11 pagesCMD DBDAnnisa Aulia AnandaNo ratings yet
- Altered Genitourinary/Renal FunctionDocument14 pagesAltered Genitourinary/Renal FunctionAshleyNo ratings yet
- Pediatric Osce Compiled by NoorUlAin.Document29 pagesPediatric Osce Compiled by NoorUlAin.amashooquekubarNo ratings yet
- Prof. Syarifuddin Rauf (Sindrome Nefrotik, UTI, GNAPS)Document75 pagesProf. Syarifuddin Rauf (Sindrome Nefrotik, UTI, GNAPS)Siti Fildzah NadhilahNo ratings yet
- Table 1. Diagnostic Criteria For Kawasaki DiseaseDocument2 pagesTable 1. Diagnostic Criteria For Kawasaki DiseasenasibdinNo ratings yet
- HematuriaDocument14 pagesHematuriahamidNo ratings yet
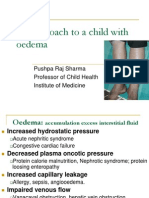
- An Approach To A Child With OedemaDocument14 pagesAn Approach To A Child With OedemaSajad AliNo ratings yet
- أسئلة أطفال دبلوم نهائي حمدان حجازيDocument6 pagesأسئلة أطفال دبلوم نهائي حمدان حجازيaslamNo ratings yet
- 7c.salivary Gland 3Document39 pages7c.salivary Gland 3bunny.boy6452No ratings yet
- CKDDocument48 pagesCKDJuniorNo ratings yet
- General Survey by DR ADBDocument34 pagesGeneral Survey by DR ADBRahul KumarNo ratings yet
- Dissect CPC CASE 2022Document8 pagesDissect CPC CASE 2022Kenneth NuñezNo ratings yet
- Viral Diseases of Alimentary Canal in CaninesDocument37 pagesViral Diseases of Alimentary Canal in CaninesNavneet BajwaNo ratings yet
- Hema Lesson ADocument31 pagesHema Lesson AEbiNo ratings yet
- SEI - INEP - 0137469 - Projeto BásicoDocument29 pagesSEI - INEP - 0137469 - Projeto BásicoMARLOMbran HERRNo ratings yet
- Acute GastroenteritisDocument48 pagesAcute Gastroenteritisansam kamalNo ratings yet
- Nephrology Best RDocument6 pagesNephrology Best Rfrabzi100% (1)
- Dr. Ery Olivianto, Sp.A: Division of Gastrohepatology, Child Health DepartmentDocument15 pagesDr. Ery Olivianto, Sp.A: Division of Gastrohepatology, Child Health DepartmentignasachyntiaNo ratings yet
- Viral Diarrheal Diseases CorrectDocument39 pagesViral Diarrheal Diseases Correctmehrshad Farahpour Gp5No ratings yet
- KawasakiDocument31 pagesKawasakirhazamNo ratings yet
- HematuriaDocument28 pagesHematuriaEmily EresumaNo ratings yet
- Plabable-Gems-14. Paediatrics Plabable GemsDocument50 pagesPlabable-Gems-14. Paediatrics Plabable GemsKhalid HabibNo ratings yet
- 1.3 Demam Tifoid Dan Kelainan HeparDocument145 pages1.3 Demam Tifoid Dan Kelainan HeparajikwaNo ratings yet
- Kawasaki DiseaseDocument58 pagesKawasaki DiseaseLei OhNo ratings yet
- Kawasaki Disease What Is Kawasaki Disease?Document6 pagesKawasaki Disease What Is Kawasaki Disease?Arafat Masud NiloyNo ratings yet
- PowerpointDocument29 pagesPowerpointpisces200910No ratings yet
- Approach To A Child With HepatosplenomegalyDocument14 pagesApproach To A Child With HepatosplenomegalyDr.P.NatarajanNo ratings yet
- Part 2 Communicable DiseaseDocument19 pagesPart 2 Communicable DiseaseKystrel Delos SantosNo ratings yet
- Aphthous Ulcer: Syarifah Nazira 1610211050Document17 pagesAphthous Ulcer: Syarifah Nazira 1610211050Zuhud Zinedine PangindraNo ratings yet
- Approach To PallorDocument25 pagesApproach To PallorlaibaNo ratings yet
- The Newborn ExaminationDocument132 pagesThe Newborn ExaminationdevilstNo ratings yet
- Approach To A Child With Hematuria:: Sunil Agrawal 1 Year MD Pediatrics, IOMDocument42 pagesApproach To A Child With Hematuria:: Sunil Agrawal 1 Year MD Pediatrics, IOMAnthony Salazar RodríguezNo ratings yet
- Kawasaki Disease FDNEDocument23 pagesKawasaki Disease FDNERonit KumarNo ratings yet
- Nephrotic Syndrome - PPTX 3Document56 pagesNephrotic Syndrome - PPTX 3diadilshad04No ratings yet
- Nephrotic Syndrome - PPTX 2Document92 pagesNephrotic Syndrome - PPTX 2diadilshad04No ratings yet
- Acute GlomerulonephritisDocument32 pagesAcute GlomerulonephritisEzekiel moraraNo ratings yet
- A Very Pale Three-Year-Old: Case 2 Diagnosis: Transient Erythroblastopenia of ChildhoodDocument3 pagesA Very Pale Three-Year-Old: Case 2 Diagnosis: Transient Erythroblastopenia of ChildhoodYukii Triby-a AnniimesztNo ratings yet
- Sunday Journal - LYMDocument23 pagesSunday Journal - LYMAlon GoldfainerNo ratings yet
- Acute Gastro Enteritis Case StudyDocument71 pagesAcute Gastro Enteritis Case Studygiadda100% (2)
- RupaDocument65 pagesRupaabrarbashir40No ratings yet
- The Reye Syndrome Sourcebook: A Concise Guide for Parents and PatientsFrom EverandThe Reye Syndrome Sourcebook: A Concise Guide for Parents and PatientsNo ratings yet
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- North Carolina Children’s Global Health Handbook: A Pediatrician’s Guide to Integrating IMCI Guidelines in Sub-Saharan AfricaFrom EverandNorth Carolina Children’s Global Health Handbook: A Pediatrician’s Guide to Integrating IMCI Guidelines in Sub-Saharan AfricaErica C. BjornstadNo ratings yet
- Coeliac Disease: DR Lei Lei WinDocument14 pagesCoeliac Disease: DR Lei Lei WinSivakumar Kathuu KarthikeyanNo ratings yet
- Ultimate Surgery MCQDocument104 pagesUltimate Surgery MCQSivakumar Kathuu KarthikeyanNo ratings yet
- Antepartum Haemorrhage - Placenta Previa, Abruption 2Document78 pagesAntepartum Haemorrhage - Placenta Previa, Abruption 2Sivakumar Kathuu KarthikeyanNo ratings yet
- A-@Elective Posting-Hospital Supervisor - S GuidenewDocument15 pagesA-@Elective Posting-Hospital Supervisor - S GuidenewSivakumar Kathuu KarthikeyanNo ratings yet
- L11 - Anatomy of The SkullDocument36 pagesL11 - Anatomy of The SkullSivakumar Kathuu KarthikeyanNo ratings yet
- Anatomy and Physiology: AUCMS MD Programme Year 1 (SY 2013-2014) Allianze University College of Medical Sciences (AUCMS)Document46 pagesAnatomy and Physiology: AUCMS MD Programme Year 1 (SY 2013-2014) Allianze University College of Medical Sciences (AUCMS)Sivakumar Kathuu KarthikeyanNo ratings yet