Download as pptx, pdf, or txt
You might also like
- Interpretation: L63 - Ankit Jain Sagar Cc-3 I/F HDFC Bank Parkota Ward Goughat SAGAR-470002 M.PDocument2 pagesInterpretation: L63 - Ankit Jain Sagar Cc-3 I/F HDFC Bank Parkota Ward Goughat SAGAR-470002 M.PAviral SinghNo ratings yet
- Test Bank For Maternity Nursing 8th Edition, LowdermilkDocument26 pagesTest Bank For Maternity Nursing 8th Edition, LowdermilkILL101100% (3)
- London Med Student Neurology CasesDocument11 pagesLondon Med Student Neurology CasesAmmuNo ratings yet
- Catastrophic Neurologic Disorders in The Emergency Department 2nd Ed PDFDocument344 pagesCatastrophic Neurologic Disorders in The Emergency Department 2nd Ed PDFTarmidi MidziNo ratings yet
- Inflammatory and Autoimmune Disorders of the Nervous System in ChildrenFrom EverandInflammatory and Autoimmune Disorders of the Nervous System in ChildrenNo ratings yet
- Developmental NeurobiologyFrom EverandDevelopmental NeurobiologyGreg LemkeNo ratings yet
- Duus'Document344 pagesDuus'ulyaamaliaNo ratings yet
- Genzyme CaseDocument12 pagesGenzyme CaseJSheikh0% (3)
- PhysioTENS Digital UserGuideDocument19 pagesPhysioTENS Digital UserGuideJassiel SantivañezNo ratings yet
- Aicardi’s Diseases of the Nervous System in Childhood, 4th EditionFrom EverandAicardi’s Diseases of the Nervous System in Childhood, 4th EditionAlexis ArzimanoglouNo ratings yet
- Neurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesFrom EverandNeurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesNo ratings yet
- Blood Supply of The BrainDocument37 pagesBlood Supply of The BrainueumanaNo ratings yet
- Nervous System DiseasesDocument16 pagesNervous System DiseasesShahzad ShameemNo ratings yet
- Pediatric EpilepsyDocument6 pagesPediatric EpilepsyJosh RoshalNo ratings yet
- Ch28 CNSDocument184 pagesCh28 CNSdray2bigNo ratings yet
- Higher Mental Function Examination Dementia, Altered MentalDocument37 pagesHigher Mental Function Examination Dementia, Altered MentalCamille DoamanNo ratings yet
- Stroke (Brain Attack) : Frontal Lobe (Blue)Document6 pagesStroke (Brain Attack) : Frontal Lobe (Blue)Pauline ChanNo ratings yet
- Neurology: Q. What Are The Causes of CVD (Stroke) in A Young Patient? AnswerDocument9 pagesNeurology: Q. What Are The Causes of CVD (Stroke) in A Young Patient? Answerdrng48No ratings yet
- 55 Cases in NeurologyDocument419 pages55 Cases in NeurologykhawlahbintialazwarNo ratings yet
- Brain DeathDocument24 pagesBrain DeathKawaljit KaurNo ratings yet
- CP Angle TumorsDocument65 pagesCP Angle TumorsDiah VerawatiNo ratings yet
- Epilepsy: Bintang Senayudha Wirasakti 1610211132Document35 pagesEpilepsy: Bintang Senayudha Wirasakti 1610211132senaNo ratings yet
- Brainstem Syndromes: Karin Johnson, MDDocument28 pagesBrainstem Syndromes: Karin Johnson, MDSteve Biko OkothNo ratings yet
- Stroke FullDocument10 pagesStroke Fullshowkat3No ratings yet
- Prof BSP-Akinetic Rigid Synd - PDDocument139 pagesProf BSP-Akinetic Rigid Synd - PDSavitha BasriNo ratings yet
- Stroke School Brockville Part 3Document39 pagesStroke School Brockville Part 3Gautam KhannaNo ratings yet
- (Contemporary Neurology Series, 66) Jasper R. Daube - Clinical Neurophysiology (Contemporary Neurology Series, 66) - Oxford University Press, USA (2002)Document676 pages(Contemporary Neurology Series, 66) Jasper R. Daube - Clinical Neurophysiology (Contemporary Neurology Series, 66) - Oxford University Press, USA (2002)atif.araf.20No ratings yet
- Clinical Decision MakingDocument13 pagesClinical Decision MakingMark VialsNo ratings yet
- Wallenberg Syndrome: Publication DetailsDocument9 pagesWallenberg Syndrome: Publication DetailsHuang Jen Liang100% (1)
- Acute MX of StrokeDocument23 pagesAcute MX of StrokeAshish GuragainNo ratings yet
- Approach To Ataxia: DR Jithesh R M6Document30 pagesApproach To Ataxia: DR Jithesh R M6jitheshNo ratings yet
- cEEG Monitoring in The ICU: Treating Subclinical Seizures Is Cost EffectiveDocument26 pagescEEG Monitoring in The ICU: Treating Subclinical Seizures Is Cost EffectiveVijay GadagiNo ratings yet
- Approach To Neurological DiseaseDocument27 pagesApproach To Neurological DiseaseNEuRoLoGisT CoFFeeCuP100% (9)
- Surgical Pathology - Diseases of The Central Nervous System 401 - Dr. Baby Lynne Asuncion - October 20-28, 2014Document10 pagesSurgical Pathology - Diseases of The Central Nervous System 401 - Dr. Baby Lynne Asuncion - October 20-28, 2014atb_phNo ratings yet
- Acute Ischaemic StrokeDocument40 pagesAcute Ischaemic StrokeDana Crusoveanu100% (1)
- Primary Mitochondrial Myopathies in Childhood 2021 Neuromuscular DisordersDocument10 pagesPrimary Mitochondrial Myopathies in Childhood 2021 Neuromuscular DisordersSuzie Simone Mardones SilvaNo ratings yet
- Neurology Update 2014Document56 pagesNeurology Update 2014lakshminivas PingaliNo ratings yet
- Basic Mechanism of Epilepsy N SeizuresDocument44 pagesBasic Mechanism of Epilepsy N SeizurestaniaNo ratings yet
- Textbook of NeuroimagingDocument403 pagesTextbook of NeuroimagingcelooshNo ratings yet
- Blood Suppy of BrainDocument54 pagesBlood Suppy of BrainZoya MoraniNo ratings yet
- The Cerebellopontine Angle and Posterior Fossa Cranial Nerves by TheDocument37 pagesThe Cerebellopontine Angle and Posterior Fossa Cranial Nerves by Thebodeadumitru9261100% (2)
- B5W1L9.Peripheral Neuropathy - Lecture Notes 12Document4 pagesB5W1L9.Peripheral Neuropathy - Lecture Notes 12mihalcea alinNo ratings yet
- Common Histories and Red Flags Presentation Noninteractive VersionDocument21 pagesCommon Histories and Red Flags Presentation Noninteractive VersionesmarNo ratings yet
- Ischaemic Stroke: Cerebrovascular DiseaseDocument39 pagesIschaemic Stroke: Cerebrovascular DiseaseA BenjaminNo ratings yet
- Approach To Neurological DiseaseDocument68 pagesApproach To Neurological DiseaseNEuRoLoGisT CoFFeeCuPNo ratings yet
- Neurology ConferenceDocument59 pagesNeurology ConferencePGHC100% (4)
- Headache: Rosen's Chapters 17 and 105 November 9, 2006 by George FiliadisDocument45 pagesHeadache: Rosen's Chapters 17 and 105 November 9, 2006 by George Filiadishemanthshah2801No ratings yet
- Approach To SyncopeDocument38 pagesApproach To SyncopeNurhafizah IbrahimNo ratings yet
- Insights Into Clinical Neurology 2023Document112 pagesInsights Into Clinical Neurology 2023Артем ПустовитNo ratings yet
- Neurology NotesDocument15 pagesNeurology NotesAshley Diane Henry100% (3)
- Epilepsy and Seizure DisordersDocument38 pagesEpilepsy and Seizure DisordersMalueth AnguiNo ratings yet
- Migraine in Childhood: And Other Non-Epileptic Paroxysmal DisordersFrom EverandMigraine in Childhood: And Other Non-Epileptic Paroxysmal DisordersJudith M. HockadayNo ratings yet
- Paediatrics Epileptiform DisordersDocument11 pagesPaediatrics Epileptiform DisordersayunisallehNo ratings yet
- Electrographic and Electroclinical Seizures BirdsDocument50 pagesElectrographic and Electroclinical Seizures BirdsNEUROMED NEURONo ratings yet
- DM and NeurologyDocument43 pagesDM and NeurologySurat TanprawateNo ratings yet
- AtaxiaDocument23 pagesAtaxiakara_korumNo ratings yet
- NM Neuropathies PDFDocument63 pagesNM Neuropathies PDFdr.bNo ratings yet
- A Summary of The Chemical Mediators Involve in The Acute Inflammatory Response Is Shown in The Table BelowDocument30 pagesA Summary of The Chemical Mediators Involve in The Acute Inflammatory Response Is Shown in The Table Belowinny100% (1)
- The Vascular System Doc TulaganDocument10 pagesThe Vascular System Doc Tulagankûrñï såñskrùthîNo ratings yet
- R.N. Kapoor Memorial Homoeopathic Hospital & Medical College, INDOREDocument12 pagesR.N. Kapoor Memorial Homoeopathic Hospital & Medical College, INDOREvinay patidar100% (1)
- Cerebral Aneurysm: Junchen ZhangDocument37 pagesCerebral Aneurysm: Junchen ZhangsanjivdasNo ratings yet
- Movement Disorders 4335Document28 pagesMovement Disorders 4335Fitri Amelia RizkiNo ratings yet
- Healing Yoga For Neck and Shoulder PainDocument110 pagesHealing Yoga For Neck and Shoulder Painjamalaasr94% (17)
- Expanded SkeletonsDocument25 pagesExpanded SkeletonsKristopher Garrett100% (3)
- Freaks and Marvels of Plant Life Or, Curiosities of VegetationDocument488 pagesFreaks and Marvels of Plant Life Or, Curiosities of VegetationTee SorensizzleNo ratings yet
- Ayurveda and Holistic MedicineDocument2 pagesAyurveda and Holistic Medicinemalini PatilNo ratings yet
- Set B PHC AnswerDocument11 pagesSet B PHC AnswerDiane100% (1)
- Gandhi - Collected Works Vol 12Document487 pagesGandhi - Collected Works Vol 12Nrusimha ( नृसिंह )No ratings yet
- Medicines Administration 1 Understanding Routes of AdministrationDocument3 pagesMedicines Administration 1 Understanding Routes of AdministrationJosa Camille BungayNo ratings yet
- Triangular Fibrocartilage Complex Injury in Professional CricketersDocument5 pagesTriangular Fibrocartilage Complex Injury in Professional Cricketersrima rizky nourliaNo ratings yet
- Excessive Genu Valgum FINALDocument13 pagesExcessive Genu Valgum FINALMeeraNo ratings yet
- Nhis Ghana - Overview Reforms Achievements Version 3Document29 pagesNhis Ghana - Overview Reforms Achievements Version 3Nana Virtuoso EsselNo ratings yet
- HIV and Sex Workers 3: SeriesDocument15 pagesHIV and Sex Workers 3: SeriesBebaskita GintingNo ratings yet
- d100 Demon LordsDocument10 pagesd100 Demon LordsStephan ChiariniNo ratings yet
- The Blue People of Troublesome CreekDocument9 pagesThe Blue People of Troublesome Creekapi-3173246110% (1)
- Annex Basic Education Enrollment FormDocument2 pagesAnnex Basic Education Enrollment FormEmbrace GraceNo ratings yet
- Reviews: Fracture Healing: Mechanisms and InterventionsDocument10 pagesReviews: Fracture Healing: Mechanisms and InterventionsFatrika DewiNo ratings yet
- 11.03.21 COVID-19 Vaccine Information - IDPHDocument5 pages11.03.21 COVID-19 Vaccine Information - IDPHLocal 5 News (WOI-TV)No ratings yet
- Biochemistry and Cell Biology of Ageing: Part III Biomedical ScienceDocument424 pagesBiochemistry and Cell Biology of Ageing: Part III Biomedical ScienceAureliano BuendiaNo ratings yet
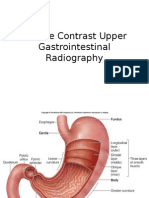
- Jurnal Double Kontras FIXDocument33 pagesJurnal Double Kontras FIXWisnuHeriPurwantoNo ratings yet
- Chromosomal AberrationsDocument17 pagesChromosomal AberrationsHajiRab NawazNo ratings yet
- 1st Periodic Test Grade Five W/ TosDocument19 pages1st Periodic Test Grade Five W/ TosReynaldo B. Lapak100% (7)
- Health, Stress, and CopingDocument49 pagesHealth, Stress, and CopingMarissa BrionesNo ratings yet
- Case Study On: Lyceum of The Philippines UniversityDocument4 pagesCase Study On: Lyceum of The Philippines UniversityarturogarcesjrNo ratings yet
- Rockefeller Annual ReportDocument66 pagesRockefeller Annual ReportIrvan GarutNo ratings yet
- Apraxia ScreeningDocument9 pagesApraxia Screeningceci MOLARONo ratings yet
- The Breast - Comprehensive Management of Benign and Malignant Diseases 5e WWW Bookbaz IrDocument1,435 pagesThe Breast - Comprehensive Management of Benign and Malignant Diseases 5e WWW Bookbaz Irzahra m100% (1)
- Vertu Resident GuideDocument68 pagesVertu Resident Guideliyana1810No ratings yet