Download as pptx, pdf, or txt
You might also like
- Final Case Study NCM 116Document60 pagesFinal Case Study NCM 116Marissa AsimNo ratings yet
- LIVERDocument18 pagesLIVERShivaniLeela100% (3)
- Anatomy of The Kidney & Ureter - NewDocument42 pagesAnatomy of The Kidney & Ureter - NewHaider Nadhem AL-rubai0% (1)
- Nephrologi: - PWM Olly Indrajani - 18-3-2015Document128 pagesNephrologi: - PWM Olly Indrajani - 18-3-2015NandatholoeNo ratings yet
- Kidney and UreterDocument9 pagesKidney and UreterDianne EstradaNo ratings yet
- Abdomen 5Document71 pagesAbdomen 5spitzmark2030No ratings yet
- KidneysDocument8 pagesKidneysmarlyxsukiNo ratings yet
- LiverDocument3 pagesLiverMamunNo ratings yet
- Pancreas 2017Document53 pagesPancreas 2017yasrul izadNo ratings yet
- The Urinary System: Muh - Iqbal Basri Anatomy Department Hasanuddin UniversityDocument44 pagesThe Urinary System: Muh - Iqbal Basri Anatomy Department Hasanuddin UniversityRahmawati HamudiNo ratings yet
- 13b.blood Vessels of AbdomenDocument71 pages13b.blood Vessels of AbdomenIshimwe TheotimeNo ratings yet
- UyzxcvDocument100 pagesUyzxcvValentin RotaruNo ratings yet
- Lect 4 Urinary SystemDocument42 pagesLect 4 Urinary Systemnightter4No ratings yet
- Human Anatomy,: Renal /urinary SystemDocument62 pagesHuman Anatomy,: Renal /urinary Systemsapana shresthaNo ratings yet
- 4.kidneys, Ureters and Suprarenal GlandsDocument57 pages4.kidneys, Ureters and Suprarenal GlandsIshimwe TheotimeNo ratings yet
- Renal Physiology 1 1aDocument88 pagesRenal Physiology 1 1afentaw melkieNo ratings yet
- Pancreas Eman 2020Document27 pagesPancreas Eman 2020Eman AbdulghaniNo ratings yet
- Anatomy RCR1 RenalDocument3 pagesAnatomy RCR1 RenaleamcrawleyNo ratings yet
- DR Laxman Khanal Bpkihs 07-06-2013Document86 pagesDR Laxman Khanal Bpkihs 07-06-2013Bilal YimamNo ratings yet
- 7.1 Urinary f2f s1b2-23Document47 pages7.1 Urinary f2f s1b2-23shlokNo ratings yet
- Kidney and Ureter For Paramedical StudentsDocument53 pagesKidney and Ureter For Paramedical Studentslakshmiraman1770No ratings yet
- Anatomy of The Renal SystemDocument67 pagesAnatomy of The Renal SystemRIUNGU PENINAH GATWIRINo ratings yet
- Clinical Oriented Anatomy of Urinary SystemDocument81 pagesClinical Oriented Anatomy of Urinary SystemRizcky Naldy Eka Putra100% (1)
- The Anatomy, Histology and Development of The Kidney PDFDocument14 pagesThe Anatomy, Histology and Development of The Kidney PDFredderdatNo ratings yet
- General Structure and Functions of Urinary System-Week 11Document49 pagesGeneral Structure and Functions of Urinary System-Week 11Reentsha EllyNo ratings yet
- The Renal SystemDocument50 pagesThe Renal SystemJoseph RishmawiNo ratings yet
- Retroperitonium: Yosef TadesseDocument94 pagesRetroperitonium: Yosef Tadessetesfaye mekonnenNo ratings yet
- Anatomy For The Gynecologic OncologistDocument70 pagesAnatomy For The Gynecologic OncologistjroshsperlingNo ratings yet
- Anatomy of Urinary SystemDocument43 pagesAnatomy of Urinary Systemandrea titus100% (1)
- Portocaval AnastomosisDocument42 pagesPortocaval AnastomosisAayush BhattaNo ratings yet
- Urinary SystemDocument37 pagesUrinary SystemNOELIE IBACARRANo ratings yet
- Urinary SystemDocument55 pagesUrinary SystemChristian UdaundoNo ratings yet
- Anatomyofrectum 110521140034 Phpapp02Document62 pagesAnatomyofrectum 110521140034 Phpapp02Emmanuel AdemoNo ratings yet
- Curs 11. Sistemul ExcretorDocument66 pagesCurs 11. Sistemul ExcretorDobrincu MirelaNo ratings yet
- The Kidney: Hemanth P Dialysis Tutor B N Patel Institute of Paramedical & SciencesDocument46 pagesThe Kidney: Hemanth P Dialysis Tutor B N Patel Institute of Paramedical & SciencesHemanth PrakashNo ratings yet
- LiverDocument45 pagesLiversiddharth.roy26587No ratings yet
- Functional Anatomy of Renal System: by DR Amber IlyasDocument51 pagesFunctional Anatomy of Renal System: by DR Amber IlyasAlexah BanuagNo ratings yet
- Anatomy - Kidney'sDocument18 pagesAnatomy - Kidney'sOlivia MorrisonNo ratings yet
- L31 - Renal SystemDocument30 pagesL31 - Renal SystemsairahhannahNo ratings yet
- Nephron CompressDocument91 pagesNephron CompressAlligator ZNo ratings yet
- Pancreas FinalDocument31 pagesPancreas FinalBonzowoNo ratings yet
- PancreasDocument11 pagesPancreasCheng XinvennNo ratings yet
- The Urinary System: Muh - Iqbal Basri Anatomy Department Hasanuddin UniversityDocument41 pagesThe Urinary System: Muh - Iqbal Basri Anatomy Department Hasanuddin Universityraynhard b. fandresNo ratings yet
- Anatomy and Physiology of The Urinary System: Dipali HarkhaniDocument43 pagesAnatomy and Physiology of The Urinary System: Dipali HarkhaniZala KarmitNo ratings yet
- Urinary SystemDocument30 pagesUrinary SystemTamiru KetemaNo ratings yet
- RENALDocument29 pagesRENALJenica SorianoNo ratings yet
- Anatomy of LiverDocument86 pagesAnatomy of Liverchandana pallavaNo ratings yet
- The Urinary SystemDocument66 pagesThe Urinary Systemapi-26587879No ratings yet
- Liver: DR Kiran ShahidDocument21 pagesLiver: DR Kiran ShahidYashfa Yasin100% (1)
- The PancreasDocument31 pagesThe PancreasAryan DesaiNo ratings yet
- Anatomy of Liver and Pancreas by Kazim AliDocument32 pagesAnatomy of Liver and Pancreas by Kazim AliAhmad KhanNo ratings yet
- Anatomy of KidneyDocument19 pagesAnatomy of KidneydrsooryasridharNo ratings yet
- Anatomy of Urinary Tract BaruDocument68 pagesAnatomy of Urinary Tract BaruAdya ArradikhaNo ratings yet
- Lect-Urinary Syst - 21Document75 pagesLect-Urinary Syst - 21f20231186No ratings yet
- Alvin B. Vibar, M.D.Document49 pagesAlvin B. Vibar, M.D.Ditas ChuNo ratings yet
- HemodialysisDocument23 pagesHemodialysisKrishnaBihariShuklaNo ratings yet
- Liver: Dr. Sudhanshu Raut Anatomy PG 1 YearDocument16 pagesLiver: Dr. Sudhanshu Raut Anatomy PG 1 YearDr. Sudhanshu RautNo ratings yet
- Anatomy and Physiology of Urinary SystemDocument53 pagesAnatomy and Physiology of Urinary SystemArathy KalathingalNo ratings yet
- 7 Osteomyelitis of JawsDocument38 pages7 Osteomyelitis of JawsDan 04No ratings yet
- Drug Study PantoprazoleDocument2 pagesDrug Study PantoprazoleFlauros Ryu Jabien100% (3)
- GIT Viral Hepatitis in Children - PPT 93Document22 pagesGIT Viral Hepatitis in Children - PPT 93Dr.P.NatarajanNo ratings yet
- Testicular Examination OSCE GuideDocument9 pagesTesticular Examination OSCE Guidecharlyn206No ratings yet
- ICD For OncologyDocument337 pagesICD For OncologytphivuongNo ratings yet
- Lycopeptides: Jagir R. Patel Asst Prof Dept. Pharmacology Anand Pharmacy CollegeDocument12 pagesLycopeptides: Jagir R. Patel Asst Prof Dept. Pharmacology Anand Pharmacy CollegeJagirNo ratings yet
- Trusted Medical Answers-In Seconds.: GonorrheaDocument7 pagesTrusted Medical Answers-In Seconds.: GonorrheantnquynhproNo ratings yet
- تجميعات اسئلة للنظام الجديدDocument12 pagesتجميعات اسئلة للنظام الجديدMohamed.A. KudaihNo ratings yet
- Valpros PediaDocument2 pagesValpros PediaAnnsh Hadji EliasNo ratings yet
- Functional Cognitive Disorder: Dementia's Blind Spot: UpdateDocument9 pagesFunctional Cognitive Disorder: Dementia's Blind Spot: UpdatePriscila Lorencini SelingardiNo ratings yet
- Harmacology: (Trans) Autonomic Pharmacology Topic OutlineDocument7 pagesHarmacology: (Trans) Autonomic Pharmacology Topic OutlineMa. Mil Adrianne PamaNo ratings yet
- Journal of The Neurological Sciences: SciencedirectDocument12 pagesJournal of The Neurological Sciences: SciencedirectBotez MartaNo ratings yet
- A Case of Ulcerative Livedoid Vasculopathy Treated Successfully With Pentoxifylline and ColchicineDocument4 pagesA Case of Ulcerative Livedoid Vasculopathy Treated Successfully With Pentoxifylline and Colchicinekahkashanahmed065No ratings yet
- Evidence-Based Medicine: Wound ManagementDocument16 pagesEvidence-Based Medicine: Wound ManagementRafael FerreiraNo ratings yet
- History - CushingDocument6 pagesHistory - CushingNur FadzreenaNo ratings yet
- PulmCrit - Understanding Happy Hypoxemia PhysiologyDocument13 pagesPulmCrit - Understanding Happy Hypoxemia PhysiologyhardianNo ratings yet
- 12 Pathology of The Head and Neck 2016 PDFDocument851 pages12 Pathology of The Head and Neck 2016 PDFManuel Mardones Torres100% (1)
- A Study On Clinical, Radiological and Electrophysiological Profile in Patients Presenting With First Unprovoked SeizureDocument8 pagesA Study On Clinical, Radiological and Electrophysiological Profile in Patients Presenting With First Unprovoked Seizureindex PubNo ratings yet
- Medical Management Packages Updated 20 July 2023Document11 pagesMedical Management Packages Updated 20 July 2023mukesh kumawatNo ratings yet
- Benign Ovarian TumorsDocument5 pagesBenign Ovarian Tumorsraissametasari100% (1)
- A Lecture Schedule, July 2015-June 2016Document12 pagesA Lecture Schedule, July 2015-June 2016Shahriar Kabir DaneNo ratings yet
- Who Classificação TO 2022 PDFDocument13 pagesWho Classificação TO 2022 PDFGrasieli RamosNo ratings yet
- IDEXX CBC Chem ExplainedDocument38 pagesIDEXX CBC Chem Explainedmmatthew74No ratings yet
- Kawasaki Disease CaseDocument64 pagesKawasaki Disease CaseRon Christian Neil RodriguezNo ratings yet
- Laboratory AnalysisDocument6 pagesLaboratory AnalysisJm CoguincoNo ratings yet
- StrabismusDocument27 pagesStrabismuspason1988No ratings yet
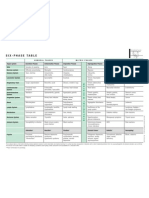
- Six-Phase Table: International Society of HomotoxicologyDocument1 pageSix-Phase Table: International Society of HomotoxicologyPablo Matas SoriaNo ratings yet
- WJG 23 6137Document16 pagesWJG 23 6137MUHAMMAD09No ratings yet
- Genetic Disorders SourcebookDocument748 pagesGenetic Disorders Sourcebookpaconscribd100% (1)