Download as ppt, pdf, or txt
You might also like
- Galler Spacing Technique (GST) ManualDocument44 pagesGaller Spacing Technique (GST) ManualDavid Galler100% (1)
- RecipeTin Eats - Fast Prep Big Flavors Cookbook PDFDocument38 pagesRecipeTin Eats - Fast Prep Big Flavors Cookbook PDFJaellah Matawa100% (2)
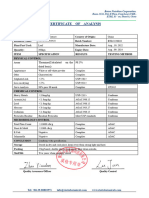
- Water Test ReportDocument1 pageWater Test ReportMollah Md NaimNo ratings yet
- UW Allergy + Immuno - Educational Objectives PDFDocument25 pagesUW Allergy + Immuno - Educational Objectives PDFDrbee10No ratings yet
- Immunology Flash CardsDocument46 pagesImmunology Flash CardsRickyNoviantoNo ratings yet
- Activity DesignDocument2 pagesActivity Designsanie50% (2)
- 08 ImmunopathologyDocument118 pages08 ImmunopathologySteven Mark MananguNo ratings yet
- How Do B Cells Produce Antibodies?Document165 pagesHow Do B Cells Produce Antibodies?Sharmaine TrangiaNo ratings yet
- HYPERSENSITIVITYDocument87 pagesHYPERSENSITIVITYinfo.foodbitNo ratings yet
- Chapter 6 - Diseases of The Immune SystemDocument12 pagesChapter 6 - Diseases of The Immune SystemAgnieszka WisniewskaNo ratings yet
- University of Santo Tomas: Faculty of Pharmacy - Department of Medical TechnologyDocument7 pagesUniversity of Santo Tomas: Faculty of Pharmacy - Department of Medical TechnologyWynlor AbarcaNo ratings yet
- Hypersensitivity: Erwin Taher FK Uisu 2011Document48 pagesHypersensitivity: Erwin Taher FK Uisu 2011rido rahmad saputraNo ratings yet
- Basic Immunology of Allergic Disease: Tutik Ida Rosanti Laboratorium ParasitologiDocument17 pagesBasic Immunology of Allergic Disease: Tutik Ida Rosanti Laboratorium ParasitologiFiqrotul UmamNo ratings yet
- Chapter 11 Undisarable and Alterd ImmunotyDocument81 pagesChapter 11 Undisarable and Alterd ImmunotyTofikNo ratings yet
- The Immune System: Disease Recovery No DiseaseDocument25 pagesThe Immune System: Disease Recovery No DiseaseKartika DwiNo ratings yet
- IMMUNOLOGYDocument48 pagesIMMUNOLOGYIqbalmia911No ratings yet
- 19 - Lecture - PPT Lymphatic ImmunityDocument191 pages19 - Lecture - PPT Lymphatic ImmunityGwyneth Adrienne Leigh VillapandoNo ratings yet
- Immunology: E. A. JalalDocument60 pagesImmunology: E. A. JalalazlinnursulianyNo ratings yet
- Hypersensitivity 2Document51 pagesHypersensitivity 2Ravi KoppoluNo ratings yet
- Immunology - BPT Drug AllergyDocument42 pagesImmunology - BPT Drug AllergyNaeman GoetzNo ratings yet
- HypersensitivityDocument12 pagesHypersensitivityDwi TyoNo ratings yet
- 12.hypersensitivity 2013Document58 pages12.hypersensitivity 2013lookmoo100% (1)
- 14 超敏反应Document32 pages14 超敏反应Jennifer DixonNo ratings yet
- Overview of The Immune System 2020Document31 pagesOverview of The Immune System 2020mehakNo ratings yet
- Immunology PDFDocument70 pagesImmunology PDFstancy thomasNo ratings yet
- Veterinary Immunology: Fuad Mohammed (DVM, MSC, Assist. Prof.)Document36 pagesVeterinary Immunology: Fuad Mohammed (DVM, MSC, Assist. Prof.)BEKUMA SHIBIRUNo ratings yet
- Human Autoimmune Diseases: Disease Autoantigen Symptoms ExtentDocument6 pagesHuman Autoimmune Diseases: Disease Autoantigen Symptoms ExtentsauravsarkarNo ratings yet
- Hypersensitive Reactions 2-4Document29 pagesHypersensitive Reactions 2-4Ammara ZulqarnainNo ratings yet
- 05 ImmunologyDocument66 pages05 Immunologytemesgen.girma0906No ratings yet
- Hypersensitivity ReactionsDocument66 pagesHypersensitivity ReactionsA. PathakNo ratings yet
- Immuno PathologyDocument71 pagesImmuno Pathologyb9p6vmfnc4No ratings yet
- Name: Urwa Hafeez Roll No.: BZOF17M037 Topic:: Hypersensitivity Type-IIIDocument30 pagesName: Urwa Hafeez Roll No.: BZOF17M037 Topic:: Hypersensitivity Type-IIIurwa hafeezNo ratings yet
- Immunology. 10. Allergy-1Document40 pagesImmunology. 10. Allergy-1safildhaNo ratings yet
- Hypersensitivity: M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM UniversityDocument87 pagesHypersensitivity: M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM UniversityJulienne Sanchez-SalazarNo ratings yet
- General Features of Immune System Immune System: DefinitionDocument17 pagesGeneral Features of Immune System Immune System: Definitionمحمد نعیم اقبالNo ratings yet
- Innate and Adaptive Immunity: - Innate Is FIRST LINE OF DEFENCE: No Prior Exposure Needed - Comprised OfDocument31 pagesInnate and Adaptive Immunity: - Innate Is FIRST LINE OF DEFENCE: No Prior Exposure Needed - Comprised OfBegumHazinNo ratings yet
- Lecture 19, Ch. 43Document21 pagesLecture 19, Ch. 43S. SpencerNo ratings yet
- Sesi 1 - DR - Umi - Imunologi Transfusi DarahDocument46 pagesSesi 1 - DR - Umi - Imunologi Transfusi DarahWanda RyNo ratings yet
- Hypersensitivity: Robert Beatty MCB150Document48 pagesHypersensitivity: Robert Beatty MCB150Lop LlorinNo ratings yet
- Management of Clients With Immune DisordersDocument75 pagesManagement of Clients With Immune DisordersRatih Purnamasari Nu AmooreaNo ratings yet
- Immuno 4Document34 pagesImmuno 4SedqamNo ratings yet
- Lecture 13-Immunodefficiency in Elderly-Dr. Eko Aribowo, M.Kes, SpPD-KGer (2019)Document30 pagesLecture 13-Immunodefficiency in Elderly-Dr. Eko Aribowo, M.Kes, SpPD-KGer (2019)stefany huangNo ratings yet
- 7.1 ImmunityDocument28 pages7.1 ImmunitymegjaNo ratings yet
- Basic Immunology: Presented By: Aarya.H.Nair First Year Mds Department of Oral Medicine & RadiologyDocument62 pagesBasic Immunology: Presented By: Aarya.H.Nair First Year Mds Department of Oral Medicine & RadiologyAARYANo ratings yet
- HypersensitivityDocument85 pagesHypersensitivityasad bashir94% (16)
- AutoimmunityDocument29 pagesAutoimmunitywissam salimNo ratings yet
- Goljan RR - ImmunopathologyDocument13 pagesGoljan RR - ImmunopathologyShaz ChindhyNo ratings yet
- DR - Tjok. Istri Anom Saturti, Sppd. MarsDocument16 pagesDR - Tjok. Istri Anom Saturti, Sppd. MarsYogiswara KarangNo ratings yet
- Immunological Aspects of Parasitic Diseases in Immunocompromised IndividualsDocument34 pagesImmunological Aspects of Parasitic Diseases in Immunocompromised IndividualsKade SilabanNo ratings yet
- Hipersensitivit AS: Dr. Safari Wahyu JatmikoDocument22 pagesHipersensitivit AS: Dr. Safari Wahyu JatmikoXarisma DafaNo ratings yet
- Auto ImmunityDocument23 pagesAuto Immunitymuneera salimNo ratings yet
- Hypersensitivity IV & VDocument3 pagesHypersensitivity IV & VVaishali PathakNo ratings yet
- Acute and Chronic InflammationDocument31 pagesAcute and Chronic InflammationaqilaNo ratings yet
- BBS2-MB-K26 RX Hypersensitivity 1-4Document36 pagesBBS2-MB-K26 RX Hypersensitivity 1-4Paul Behring ManurungNo ratings yet
- Hypersensitivity ReactionsDocument48 pagesHypersensitivity ReactionsRIMI SALOUMNo ratings yet
- Immunology NotesDocument64 pagesImmunology Notestanishkachaurasia7095No ratings yet
- AitoimunDocument42 pagesAitoimunEva WulanNo ratings yet
- Toleranceautoimmunity2011 Manchcopy 120412164818 Phpapp01Document35 pagesToleranceautoimmunity2011 Manchcopy 120412164818 Phpapp01Hira.S Faisal (Hiradr)No ratings yet
- Chapter 19 - Immune Disorder, Aids, CancerDocument55 pagesChapter 19 - Immune Disorder, Aids, Cancertheodoraelle olannaNo ratings yet
- Seminar On Immunology-HypersensitivityDocument45 pagesSeminar On Immunology-HypersensitivitySalman KhanNo ratings yet
- Hypersensitivity PDFDocument9 pagesHypersensitivity PDFAisyahNo ratings yet
- Hypersensitivity ReactionsDocument71 pagesHypersensitivity Reactionslianefheldelrosario20No ratings yet
- Micro Lecture 1 Introduction To Medical Microbiology: Ma. Jennifer R. TiburcioDocument22 pagesMicro Lecture 1 Introduction To Medical Microbiology: Ma. Jennifer R. TiburcioJaellah MatawaNo ratings yet
- Questions: Questions All Things Pa-C - Free Practice QuizDocument12 pagesQuestions: Questions All Things Pa-C - Free Practice QuizJaellah MatawaNo ratings yet
- Program For February 6, 2022 Program For February 13, 2022Document2 pagesProgram For February 6, 2022 Program For February 13, 2022Jaellah MatawaNo ratings yet
- Attendance Sheet: Conductor ViolinsDocument3 pagesAttendance Sheet: Conductor ViolinsJaellah MatawaNo ratings yet
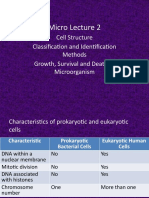
- Micro Lecture 2: Cell Structure Classification and Identification Methods Growth, Survival and Death of MicroorganismDocument78 pagesMicro Lecture 2: Cell Structure Classification and Identification Methods Growth, Survival and Death of MicroorganismJaellah MatawaNo ratings yet
- Pathogenesis of Bacterial InfectionDocument75 pagesPathogenesis of Bacterial InfectionJaellah MatawaNo ratings yet
- Visible Response To Infection by Neutrophils (Toxic Changes)Document37 pagesVisible Response To Infection by Neutrophils (Toxic Changes)Jaellah Matawa100% (1)
- Basic Mycology: Russell G. Panem, RMT School of Medical Technology Chinese General Hospital CollegesDocument47 pagesBasic Mycology: Russell G. Panem, RMT School of Medical Technology Chinese General Hospital CollegesJaellah MatawaNo ratings yet
- Cerebrospinal Fluid: By: Raynhier G. Constantino, RMTDocument53 pagesCerebrospinal Fluid: By: Raynhier G. Constantino, RMTJaellah MatawaNo ratings yet
- S. Typhi: General Characteristics: Clinical SignificanceDocument8 pagesS. Typhi: General Characteristics: Clinical SignificanceJaellah MatawaNo ratings yet
- Immune Response 02Document55 pagesImmune Response 02Jaellah MatawaNo ratings yet
- Assoc. Prof. Ma. Jennifer R. Tiburcio, MSMT Department of Med Tech UST Faculty of PharmacyDocument27 pagesAssoc. Prof. Ma. Jennifer R. Tiburcio, MSMT Department of Med Tech UST Faculty of PharmacyJaellah MatawaNo ratings yet
- Transplantation Immunology: Russell G. Panem, RMT School of Medical Technology Chinese General Hospital CollegesDocument27 pagesTransplantation Immunology: Russell G. Panem, RMT School of Medical Technology Chinese General Hospital CollegesJaellah Matawa100% (1)
- Gastric FluidDocument33 pagesGastric FluidJaellah MatawaNo ratings yet
- Leptospires General Characteristics:: Bacteriology: SpirochetesDocument5 pagesLeptospires General Characteristics:: Bacteriology: SpirochetesJaellah MatawaNo ratings yet
- Pregnancy Testing: By: Raynhier G. Constantino, RMTDocument21 pagesPregnancy Testing: By: Raynhier G. Constantino, RMTJaellah MatawaNo ratings yet
- Ra 8981Document2 pagesRa 8981Jaellah MatawaNo ratings yet
- Imslp186502 Wima.0d59 Trp2 SoloDocument1 pageImslp186502 Wima.0d59 Trp2 SoloJaellah MatawaNo ratings yet
- 16 MLT PDFDocument148 pages16 MLT PDFTanveer100% (1)
- Modalità Di Utilizzo nell'U.O. Di Oncoematologia dell'IRCC Di Candiolo e Conseguenti Implicazioni InfermieristicheDocument3 pagesModalità Di Utilizzo nell'U.O. Di Oncoematologia dell'IRCC Di Candiolo e Conseguenti Implicazioni InfermieristicheginoNo ratings yet
- Diagnosis and Management of Tremor.11Document16 pagesDiagnosis and Management of Tremor.11Stephanie Queiroz Dos SantosNo ratings yet
- MicroorganismsDocument17 pagesMicroorganismsLindzhy LimNo ratings yet
- Green Tea ExtractDocument1 pageGreen Tea Extractajitbadboy2No ratings yet
- DMSCO Log Book Vol.50 1972Document57 pagesDMSCO Log Book Vol.50 1972Des Moines University Archives and Rare Book RoomNo ratings yet
- Try Out 2 UIDocument1 pageTry Out 2 UIIto Hatma NandhitoNo ratings yet
- Inventory Scales AlphabeticallyDocument8 pagesInventory Scales Alphabeticallyserena_blue.moonNo ratings yet
- Parse's Theory of Human BecomingDocument16 pagesParse's Theory of Human Becomingprincess anneNo ratings yet
- Case 5 - (Salimbagat) Diagnostic and Laboratory ProceduresDocument12 pagesCase 5 - (Salimbagat) Diagnostic and Laboratory ProceduresChristine Pialan SalimbagatNo ratings yet
- ITFAS Ambassador Presentation 2Document27 pagesITFAS Ambassador Presentation 2Sugeng WahyudiNo ratings yet
- 2-Physiotherapy For FracturesDocument17 pages2-Physiotherapy For FracturesJuanitoCabatañaLimIIINo ratings yet
- SUMMATIVE TEST QUARTER 3 Week 3Document2 pagesSUMMATIVE TEST QUARTER 3 Week 3Mary CrisNo ratings yet
- Republic of The Philippines Regional Trial Court Branch 26Document5 pagesRepublic of The Philippines Regional Trial Court Branch 26JenMarlon Corpuz AquinoNo ratings yet
- Invitation Letter For The Students SeminarDocument1 pageInvitation Letter For The Students SeminarFelix John Paul BarquerosNo ratings yet
- OutliningDocument6 pagesOutliningOREJOLA, IRISH VAN C.No ratings yet
- Jyotish K.P. Medical AstrologyDocument239 pagesJyotish K.P. Medical AstrologyNitin Patil67% (3)
- HAZOP Case Study ExampleDocument4 pagesHAZOP Case Study ExampleanushaNo ratings yet
- Restoration of Occlusal Plane and Esthetics in Severely Worn DentitionDocument4 pagesRestoration of Occlusal Plane and Esthetics in Severely Worn DentitionUJ CommunicationNo ratings yet
- Anatomy Lab Safety Contract 1Document3 pagesAnatomy Lab Safety Contract 1api-291794000No ratings yet
- World Rankings ReportDocument5 pagesWorld Rankings Reporto3596989No ratings yet
- Subacromial Impingement Syndrome E Book 1Document28 pagesSubacromial Impingement Syndrome E Book 1niko.zaroNo ratings yet
- 3 - Updated Undertaking For EmployerDocument1 page3 - Updated Undertaking For EmployerRamnuj Orecul SoralcNo ratings yet
- Fibroid UterusDocument6 pagesFibroid UterusLucky CiniNo ratings yet
- Prevention of Candida Albicans Oral ThrushDocument8 pagesPrevention of Candida Albicans Oral ThrushZkdlin SpaceNo ratings yet
- BacteriophageDocument16 pagesBacteriophageJames FranklinNo ratings yet
- HDP COVER, FOREWORD and TABLE OF CONTENTSDocument7 pagesHDP COVER, FOREWORD and TABLE OF CONTENTSMiko MiguelNo ratings yet