
RSI Pada Pre Eklamsi
RSI Pada Pre Eklamsi
You might also like
- Surgical Cheat SheetDocument9 pagesSurgical Cheat SheetderekmiguelsmithNo ratings yet
- Hesi Maternity Ob PDFDocument32 pagesHesi Maternity Ob PDFcclaire197% (37)
- Post Op Case Studies StudentsDocument19 pagesPost Op Case Studies StudentsRenie SerranoNo ratings yet
- Patient-Centered Standards ChangesDocument61 pagesPatient-Centered Standards ChangesLenrok Adrian100% (3)
- A Anaesthesi Lscs For: Dr. Himanshu JangidDocument54 pagesA Anaesthesi Lscs For: Dr. Himanshu JangidHawsinNo ratings yet
- Anesthesia For Cesarean SectionDocument60 pagesAnesthesia For Cesarean Sectionmaheralrwimi100% (1)
- Labour Analgesia - Recent ConceptsDocument18 pagesLabour Analgesia - Recent ConceptsSuresh KumarNo ratings yet
- Anaesthetic Management of Pre-EclampsiaDocument28 pagesAnaesthetic Management of Pre-EclampsiaGeorge Junior AdomakoNo ratings yet
- 287 Paediatric Anaesthetic Emergencies Part 1Document6 pages287 Paediatric Anaesthetic Emergencies Part 1Maaida MuzaffarNo ratings yet
- Nclex 3 With RationaleDocument13 pagesNclex 3 With RationaleMsPocketbook HoarderNo ratings yet
- Journal ClubDocument39 pagesJournal ClubHassam ZulfiqarNo ratings yet
- Case Discussion - MombaelDocument29 pagesCase Discussion - MombaelLouije MombzNo ratings yet
- LMWH QML 06Document7 pagesLMWH QML 06pd7qmlNo ratings yet
- PCA in LabourDocument3 pagesPCA in LabourYwagar YwagarNo ratings yet
- GentDocument2 pagesGentOxford666No ratings yet
- Dev Roe 2015Document7 pagesDev Roe 2015nanang hidayatullohNo ratings yet
- Short Answer Questions AnaesthesiaDocument91 pagesShort Answer Questions AnaesthesiaMeena Ct100% (12)
- Journal Reading-Elsa Nur Rahma Diahnissa-2016730030Document11 pagesJournal Reading-Elsa Nur Rahma Diahnissa-2016730030Raka WibisonoNo ratings yet
- Analgesia For LabourDocument11 pagesAnalgesia For LabourAriefNo ratings yet
- COPDDocument20 pagesCOPDعزالدين الزوقريNo ratings yet
- 1.analgesia in ObstetricDocument25 pages1.analgesia in ObstetricSarvess MuniandyNo ratings yet
- OBG Latest DrugDocument71 pagesOBG Latest DrugT. Lamnunnem HaokipNo ratings yet
- Sedation and Analgesia in The Intubated Patient (Adult Critical Care)Document12 pagesSedation and Analgesia in The Intubated Patient (Adult Critical Care)Beatriz Maria Espinosa HernandezNo ratings yet
- DrugsDocument2 pagesDrugsgailannreyesNo ratings yet
- DrugsDocument2 pagesDrugsgailannreyesNo ratings yet
- Labor and Delivery NoteDocument26 pagesLabor and Delivery NoteyagyaNo ratings yet
- Fertility Surgery: Amy Hobbs, Sophie Kimber Craig and Patrick RossDocument9 pagesFertility Surgery: Amy Hobbs, Sophie Kimber Craig and Patrick RossdeswitrigintaNo ratings yet
- Pedi AnesthesiaDocument39 pagesPedi Anesthesiahailemichael chekolNo ratings yet
- Nifedipine in PregnancyDocument9 pagesNifedipine in PregnancyriskaNo ratings yet
- Drugstudy OrsdDocument10 pagesDrugstudy OrsdRafmar A. SalundaguitNo ratings yet
- Drugs Used in AneasthesiaDocument73 pagesDrugs Used in AneasthesiaCabdiladif Ahmed McrfNo ratings yet
- 4784 17639 1 PB PDFDocument6 pages4784 17639 1 PB PDFbaidyanath kumarNo ratings yet
- LovenoxDocument75 pagesLovenoxJayadi JaharmanNo ratings yet
- Use of LovenoxDocument13 pagesUse of LovenoxrosalinechirishianNo ratings yet
- Anesthetic ComplicationsDocument28 pagesAnesthetic ComplicationsSamuel RealesNo ratings yet
- Anaesthetic of Choice During Pregnancy and LactationDocument5 pagesAnaesthetic of Choice During Pregnancy and LactationDegefu TadesseNo ratings yet
- MX of EclampsiaDocument5 pagesMX of EclampsiaYwagar YwagarNo ratings yet
- Magnesium Sulfate - Management of Hypertensive Disorders of PregnancyDocument7 pagesMagnesium Sulfate - Management of Hypertensive Disorders of PregnancySylvester J DakaNo ratings yet
- WNHS - og.HypertensionPregnancy MagnesiumAnticonvulsantDocument13 pagesWNHS - og.HypertensionPregnancy MagnesiumAnticonvulsantNisa UlfaturrosyidaNo ratings yet
- High Alert MedicationsDocument17 pagesHigh Alert MedicationsJoanna Marie Datahan EstomoNo ratings yet
- PharmDocument67 pagesPharmElisabeth Permatasari SidabutarNo ratings yet
- Translate Morgan SecsioDocument4 pagesTranslate Morgan SecsioYolanda KasiNo ratings yet
- Anaesthesia For Casarean DeliveryDocument109 pagesAnaesthesia For Casarean DeliveryMohammed Shahnawaz HussainNo ratings yet
- Analgesia and Anesthesia in Labor and DeliveryDocument52 pagesAnalgesia and Anesthesia in Labor and DeliveryAnggri Septyan100% (1)
- Presentation 2Document43 pagesPresentation 2tadeleNo ratings yet
- Envarsus Epar Product Information enDocument51 pagesEnvarsus Epar Product Information enEnam HaqNo ratings yet
- CH 21 Obstetric AnaesthesiaDocument39 pagesCH 21 Obstetric AnaesthesiaChristian LeepoNo ratings yet
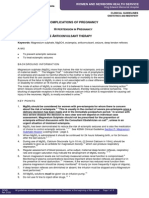
- Complications of Pregnancy H P: Agnesium Ulphate Nticonvulsant TherapyDocument8 pagesComplications of Pregnancy H P: Agnesium Ulphate Nticonvulsant TherapysucyasyifaNo ratings yet
- Sedation and Analgesia in PicuDocument37 pagesSedation and Analgesia in PicubhoopendraNo ratings yet
- Friedman VTE Bundle PDFDocument24 pagesFriedman VTE Bundle PDFGerman Parra CNo ratings yet
- LMWH Vs FondaparinuxDocument4 pagesLMWH Vs FondaparinuxMuzakhir AsrulNo ratings yet
- Acute Severe Asthma (Status Asthmaticus)Document20 pagesAcute Severe Asthma (Status Asthmaticus)blok etikakedokteranNo ratings yet
- Caeserean DeliveryDocument5 pagesCaeserean Deliveryapi-142637023No ratings yet
- Anesthesia and Procedural MonitoringDocument5 pagesAnesthesia and Procedural MonitoringVanesa Michelle Estrella ObregonNo ratings yet
- Acog HtaDocument7 pagesAcog HtaLaura María Salamanca TerneraNo ratings yet
- Endoscopy and Sedation: DR - Malavan Habeeb Internist & GI Endoscopist Lecturer - College of Medicine University of DuhokDocument37 pagesEndoscopy and Sedation: DR - Malavan Habeeb Internist & GI Endoscopist Lecturer - College of Medicine University of DuhokMalavan MohammedNo ratings yet
- P2010/0509-001 Management of EclampsiaDocument7 pagesP2010/0509-001 Management of EclampsiaYwagar YwagarNo ratings yet
- Acute Exacerbation of AsthmaDocument31 pagesAcute Exacerbation of AsthmaMuneeb YounisNo ratings yet
- Drugs StudyDocument6 pagesDrugs StudyMark_Rebibis_8528No ratings yet
- Admin,+perioperative 2 2-6-9.uk - enDocument4 pagesAdmin,+perioperative 2 2-6-9.uk - enYolanda FitrianiNo ratings yet
- Oajtmr 02 00054Document3 pagesOajtmr 02 00054MorindaNo ratings yet
- En Web Insert Cefaz NLDocument3 pagesEn Web Insert Cefaz NLAbdul AzizNo ratings yet
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYFrom EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNo ratings yet
- 1 s2.0 S240585722030067X MainDocument8 pages1 s2.0 S240585722030067X MainYader Enrique Altamirano RamirezNo ratings yet
- Anesthesia Pocket Guide 2020 PDFDocument2 pagesAnesthesia Pocket Guide 2020 PDFMaksym DemianchukNo ratings yet
- Artikel PenelitianDocument9 pagesArtikel Penelitian18 056 Nigita ZahraNo ratings yet
- Cerebrovascular Accident Under Anesthesia During Dental SurgeryDocument5 pagesCerebrovascular Accident Under Anesthesia During Dental Surgerygaluhakbar30No ratings yet
- Ot PDFDocument27 pagesOt PDFZain ShariffNo ratings yet
- MCQ MRCSDocument181 pagesMCQ MRCSAmr Sameer100% (16)
- Situation 2Document8 pagesSituation 2Rodessa Mandac TarolNo ratings yet
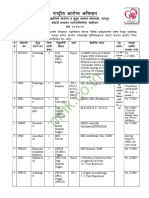
- NHM Nagpur Recruitment 2022Document5 pagesNHM Nagpur Recruitment 2022Bappasaheb PanditNo ratings yet
- Severity Assessment and Scoring For Neurosurgical Models in RodentsDocument11 pagesSeverity Assessment and Scoring For Neurosurgical Models in RodentsKazhi SujudNo ratings yet
- The Efficacy of Non-Narcotic Analgesics On Post Operative Endodontic PainDocument22 pagesThe Efficacy of Non-Narcotic Analgesics On Post Operative Endodontic PainArturo Trejo VeraNo ratings yet
- Advantages of Dexmedetomidine in Traumatic Brain Injury - A ReviewDocument5 pagesAdvantages of Dexmedetomidine in Traumatic Brain Injury - A ReviewMuhammad Arif Nur SyahidNo ratings yet
- Designing An Ideal Operating Room Complex: Indian Journal of Anaesthesia 2007 51 (3) : 193-199 Special ArticleDocument7 pagesDesigning An Ideal Operating Room Complex: Indian Journal of Anaesthesia 2007 51 (3) : 193-199 Special ArticleTejaswiniNo ratings yet
- ACEP Ketamine Guideline 2011Document13 pagesACEP Ketamine Guideline 2011Daniel Crook100% (1)
- Cesarean SectionDocument3 pagesCesarean SectionJohnmark DubdubanNo ratings yet
- 5.2024 Tattoo and PMU Anaesthetic, Repair CreamDocument6 pages5.2024 Tattoo and PMU Anaesthetic, Repair CreamVicente Rogelio Anido RamilNo ratings yet
- Anesthesia For Emergency AppendectomyDocument44 pagesAnesthesia For Emergency AppendectomyPrincess Lorenzo MiguelNo ratings yet
- Drug Study - Anesthestics....Document43 pagesDrug Study - Anesthestics....Edward Baes67% (3)
- Mansoura University. Faculty of Medicine. Thesis Branch: M.Sc. AnesthesiaDocument67 pagesMansoura University. Faculty of Medicine. Thesis Branch: M.Sc. AnesthesiaAhmed Salah HadaraNo ratings yet
- Gabapentina 300 MG Frente A 450 MG Como Premedicación Anestésica para La Hipertensión Reactiva, La Ansiedad y La AnalgesiaDocument7 pagesGabapentina 300 MG Frente A 450 MG Como Premedicación Anestésica para La Hipertensión Reactiva, La Ansiedad y La AnalgesiaNELSON DUVAN GOMEZ ROBLESNo ratings yet
- Hospital Self Assement ToolkitDocument28 pagesHospital Self Assement ToolkitNidhi VijanNo ratings yet
- Medical AnesthesticsDocument39 pagesMedical AnesthesticsAL - 12LJ 682103 Lincoln Alexander SSNo ratings yet
- Edmark 2014Document9 pagesEdmark 2014Juampi FerrariNo ratings yet
- Purity and Salaah For Muslim Patients Ebook - FINALDocument67 pagesPurity and Salaah For Muslim Patients Ebook - FINALbergville.igNo ratings yet
- SKRIPTA IZ HIRURGIJE Eng PDFDocument2,971 pagesSKRIPTA IZ HIRURGIJE Eng PDFlillyanjdeoNo ratings yet
- Synopsis SanskritiDocument22 pagesSynopsis Sanskritisanskriti_14No ratings yet
- PROGRAM 10th Annual Spring Scientific Symposium in Anaesthesiology and IntesniveCareDocument14 pagesPROGRAM 10th Annual Spring Scientific Symposium in Anaesthesiology and IntesniveCareDobrila SimonovicNo ratings yet
- Gingivectomy Case PresentationDocument20 pagesGingivectomy Case PresentationDarryl VillarNo ratings yet
























































































Download as pptx, pdf, or txt
You might also like
- Surgical Cheat SheetDocument9 pagesSurgical Cheat SheetderekmiguelsmithNo ratings yet
- Hesi Maternity Ob PDFDocument32 pagesHesi Maternity Ob PDFcclaire197% (37)
- Post Op Case Studies StudentsDocument19 pagesPost Op Case Studies StudentsRenie SerranoNo ratings yet
- Patient-Centered Standards ChangesDocument61 pagesPatient-Centered Standards ChangesLenrok Adrian100% (3)
- A Anaesthesi Lscs For: Dr. Himanshu JangidDocument54 pagesA Anaesthesi Lscs For: Dr. Himanshu JangidHawsinNo ratings yet
- Anesthesia For Cesarean SectionDocument60 pagesAnesthesia For Cesarean Sectionmaheralrwimi100% (1)
- Labour Analgesia - Recent ConceptsDocument18 pagesLabour Analgesia - Recent ConceptsSuresh KumarNo ratings yet
- Anaesthetic Management of Pre-EclampsiaDocument28 pagesAnaesthetic Management of Pre-EclampsiaGeorge Junior AdomakoNo ratings yet
- 287 Paediatric Anaesthetic Emergencies Part 1Document6 pages287 Paediatric Anaesthetic Emergencies Part 1Maaida MuzaffarNo ratings yet
- Nclex 3 With RationaleDocument13 pagesNclex 3 With RationaleMsPocketbook HoarderNo ratings yet
- Journal ClubDocument39 pagesJournal ClubHassam ZulfiqarNo ratings yet
- Case Discussion - MombaelDocument29 pagesCase Discussion - MombaelLouije MombzNo ratings yet
- LMWH QML 06Document7 pagesLMWH QML 06pd7qmlNo ratings yet
- PCA in LabourDocument3 pagesPCA in LabourYwagar YwagarNo ratings yet
- GentDocument2 pagesGentOxford666No ratings yet
- Dev Roe 2015Document7 pagesDev Roe 2015nanang hidayatullohNo ratings yet
- Short Answer Questions AnaesthesiaDocument91 pagesShort Answer Questions AnaesthesiaMeena Ct100% (12)
- Journal Reading-Elsa Nur Rahma Diahnissa-2016730030Document11 pagesJournal Reading-Elsa Nur Rahma Diahnissa-2016730030Raka WibisonoNo ratings yet
- Analgesia For LabourDocument11 pagesAnalgesia For LabourAriefNo ratings yet
- COPDDocument20 pagesCOPDعزالدين الزوقريNo ratings yet
- 1.analgesia in ObstetricDocument25 pages1.analgesia in ObstetricSarvess MuniandyNo ratings yet
- OBG Latest DrugDocument71 pagesOBG Latest DrugT. Lamnunnem HaokipNo ratings yet
- Sedation and Analgesia in The Intubated Patient (Adult Critical Care)Document12 pagesSedation and Analgesia in The Intubated Patient (Adult Critical Care)Beatriz Maria Espinosa HernandezNo ratings yet
- DrugsDocument2 pagesDrugsgailannreyesNo ratings yet
- DrugsDocument2 pagesDrugsgailannreyesNo ratings yet
- Labor and Delivery NoteDocument26 pagesLabor and Delivery NoteyagyaNo ratings yet
- Fertility Surgery: Amy Hobbs, Sophie Kimber Craig and Patrick RossDocument9 pagesFertility Surgery: Amy Hobbs, Sophie Kimber Craig and Patrick RossdeswitrigintaNo ratings yet
- Pedi AnesthesiaDocument39 pagesPedi Anesthesiahailemichael chekolNo ratings yet
- Nifedipine in PregnancyDocument9 pagesNifedipine in PregnancyriskaNo ratings yet
- Drugstudy OrsdDocument10 pagesDrugstudy OrsdRafmar A. SalundaguitNo ratings yet
- Drugs Used in AneasthesiaDocument73 pagesDrugs Used in AneasthesiaCabdiladif Ahmed McrfNo ratings yet
- 4784 17639 1 PB PDFDocument6 pages4784 17639 1 PB PDFbaidyanath kumarNo ratings yet
- LovenoxDocument75 pagesLovenoxJayadi JaharmanNo ratings yet
- Use of LovenoxDocument13 pagesUse of LovenoxrosalinechirishianNo ratings yet
- Anesthetic ComplicationsDocument28 pagesAnesthetic ComplicationsSamuel RealesNo ratings yet
- Anaesthetic of Choice During Pregnancy and LactationDocument5 pagesAnaesthetic of Choice During Pregnancy and LactationDegefu TadesseNo ratings yet
- MX of EclampsiaDocument5 pagesMX of EclampsiaYwagar YwagarNo ratings yet
- Magnesium Sulfate - Management of Hypertensive Disorders of PregnancyDocument7 pagesMagnesium Sulfate - Management of Hypertensive Disorders of PregnancySylvester J DakaNo ratings yet
- WNHS - og.HypertensionPregnancy MagnesiumAnticonvulsantDocument13 pagesWNHS - og.HypertensionPregnancy MagnesiumAnticonvulsantNisa UlfaturrosyidaNo ratings yet
- High Alert MedicationsDocument17 pagesHigh Alert MedicationsJoanna Marie Datahan EstomoNo ratings yet
- PharmDocument67 pagesPharmElisabeth Permatasari SidabutarNo ratings yet
- Translate Morgan SecsioDocument4 pagesTranslate Morgan SecsioYolanda KasiNo ratings yet
- Anaesthesia For Casarean DeliveryDocument109 pagesAnaesthesia For Casarean DeliveryMohammed Shahnawaz HussainNo ratings yet
- Analgesia and Anesthesia in Labor and DeliveryDocument52 pagesAnalgesia and Anesthesia in Labor and DeliveryAnggri Septyan100% (1)
- Presentation 2Document43 pagesPresentation 2tadeleNo ratings yet
- Envarsus Epar Product Information enDocument51 pagesEnvarsus Epar Product Information enEnam HaqNo ratings yet
- CH 21 Obstetric AnaesthesiaDocument39 pagesCH 21 Obstetric AnaesthesiaChristian LeepoNo ratings yet
- Complications of Pregnancy H P: Agnesium Ulphate Nticonvulsant TherapyDocument8 pagesComplications of Pregnancy H P: Agnesium Ulphate Nticonvulsant TherapysucyasyifaNo ratings yet
- Sedation and Analgesia in PicuDocument37 pagesSedation and Analgesia in PicubhoopendraNo ratings yet
- Friedman VTE Bundle PDFDocument24 pagesFriedman VTE Bundle PDFGerman Parra CNo ratings yet
- LMWH Vs FondaparinuxDocument4 pagesLMWH Vs FondaparinuxMuzakhir AsrulNo ratings yet
- Acute Severe Asthma (Status Asthmaticus)Document20 pagesAcute Severe Asthma (Status Asthmaticus)blok etikakedokteranNo ratings yet
- Caeserean DeliveryDocument5 pagesCaeserean Deliveryapi-142637023No ratings yet
- Anesthesia and Procedural MonitoringDocument5 pagesAnesthesia and Procedural MonitoringVanesa Michelle Estrella ObregonNo ratings yet
- Acog HtaDocument7 pagesAcog HtaLaura María Salamanca TerneraNo ratings yet
- Endoscopy and Sedation: DR - Malavan Habeeb Internist & GI Endoscopist Lecturer - College of Medicine University of DuhokDocument37 pagesEndoscopy and Sedation: DR - Malavan Habeeb Internist & GI Endoscopist Lecturer - College of Medicine University of DuhokMalavan MohammedNo ratings yet
- P2010/0509-001 Management of EclampsiaDocument7 pagesP2010/0509-001 Management of EclampsiaYwagar YwagarNo ratings yet
- Acute Exacerbation of AsthmaDocument31 pagesAcute Exacerbation of AsthmaMuneeb YounisNo ratings yet
- Drugs StudyDocument6 pagesDrugs StudyMark_Rebibis_8528No ratings yet
- Admin,+perioperative 2 2-6-9.uk - enDocument4 pagesAdmin,+perioperative 2 2-6-9.uk - enYolanda FitrianiNo ratings yet
- Oajtmr 02 00054Document3 pagesOajtmr 02 00054MorindaNo ratings yet
- En Web Insert Cefaz NLDocument3 pagesEn Web Insert Cefaz NLAbdul AzizNo ratings yet
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYFrom EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNo ratings yet
- 1 s2.0 S240585722030067X MainDocument8 pages1 s2.0 S240585722030067X MainYader Enrique Altamirano RamirezNo ratings yet
- Anesthesia Pocket Guide 2020 PDFDocument2 pagesAnesthesia Pocket Guide 2020 PDFMaksym DemianchukNo ratings yet
- Artikel PenelitianDocument9 pagesArtikel Penelitian18 056 Nigita ZahraNo ratings yet
- Cerebrovascular Accident Under Anesthesia During Dental SurgeryDocument5 pagesCerebrovascular Accident Under Anesthesia During Dental Surgerygaluhakbar30No ratings yet
- Ot PDFDocument27 pagesOt PDFZain ShariffNo ratings yet
- MCQ MRCSDocument181 pagesMCQ MRCSAmr Sameer100% (16)
- Situation 2Document8 pagesSituation 2Rodessa Mandac TarolNo ratings yet
- NHM Nagpur Recruitment 2022Document5 pagesNHM Nagpur Recruitment 2022Bappasaheb PanditNo ratings yet
- Severity Assessment and Scoring For Neurosurgical Models in RodentsDocument11 pagesSeverity Assessment and Scoring For Neurosurgical Models in RodentsKazhi SujudNo ratings yet
- The Efficacy of Non-Narcotic Analgesics On Post Operative Endodontic PainDocument22 pagesThe Efficacy of Non-Narcotic Analgesics On Post Operative Endodontic PainArturo Trejo VeraNo ratings yet
- Advantages of Dexmedetomidine in Traumatic Brain Injury - A ReviewDocument5 pagesAdvantages of Dexmedetomidine in Traumatic Brain Injury - A ReviewMuhammad Arif Nur SyahidNo ratings yet
- Designing An Ideal Operating Room Complex: Indian Journal of Anaesthesia 2007 51 (3) : 193-199 Special ArticleDocument7 pagesDesigning An Ideal Operating Room Complex: Indian Journal of Anaesthesia 2007 51 (3) : 193-199 Special ArticleTejaswiniNo ratings yet
- ACEP Ketamine Guideline 2011Document13 pagesACEP Ketamine Guideline 2011Daniel Crook100% (1)
- Cesarean SectionDocument3 pagesCesarean SectionJohnmark DubdubanNo ratings yet
- 5.2024 Tattoo and PMU Anaesthetic, Repair CreamDocument6 pages5.2024 Tattoo and PMU Anaesthetic, Repair CreamVicente Rogelio Anido RamilNo ratings yet
- Anesthesia For Emergency AppendectomyDocument44 pagesAnesthesia For Emergency AppendectomyPrincess Lorenzo MiguelNo ratings yet
- Drug Study - Anesthestics....Document43 pagesDrug Study - Anesthestics....Edward Baes67% (3)
- Mansoura University. Faculty of Medicine. Thesis Branch: M.Sc. AnesthesiaDocument67 pagesMansoura University. Faculty of Medicine. Thesis Branch: M.Sc. AnesthesiaAhmed Salah HadaraNo ratings yet
- Gabapentina 300 MG Frente A 450 MG Como Premedicación Anestésica para La Hipertensión Reactiva, La Ansiedad y La AnalgesiaDocument7 pagesGabapentina 300 MG Frente A 450 MG Como Premedicación Anestésica para La Hipertensión Reactiva, La Ansiedad y La AnalgesiaNELSON DUVAN GOMEZ ROBLESNo ratings yet
- Hospital Self Assement ToolkitDocument28 pagesHospital Self Assement ToolkitNidhi VijanNo ratings yet
- Medical AnesthesticsDocument39 pagesMedical AnesthesticsAL - 12LJ 682103 Lincoln Alexander SSNo ratings yet
- Edmark 2014Document9 pagesEdmark 2014Juampi FerrariNo ratings yet
- Purity and Salaah For Muslim Patients Ebook - FINALDocument67 pagesPurity and Salaah For Muslim Patients Ebook - FINALbergville.igNo ratings yet
- SKRIPTA IZ HIRURGIJE Eng PDFDocument2,971 pagesSKRIPTA IZ HIRURGIJE Eng PDFlillyanjdeoNo ratings yet
- Synopsis SanskritiDocument22 pagesSynopsis Sanskritisanskriti_14No ratings yet
- PROGRAM 10th Annual Spring Scientific Symposium in Anaesthesiology and IntesniveCareDocument14 pagesPROGRAM 10th Annual Spring Scientific Symposium in Anaesthesiology and IntesniveCareDobrila SimonovicNo ratings yet
- Gingivectomy Case PresentationDocument20 pagesGingivectomy Case PresentationDarryl VillarNo ratings yet