
DR Sutikno Fibrilasi Atrium
DR Sutikno Fibrilasi Atrium
You might also like
- 9 - Internal Medicine Buzzwords Handout Oct 2023 John Michael RuizDocument8 pages9 - Internal Medicine Buzzwords Handout Oct 2023 John Michael RuizJohn Michael RuizNo ratings yet
- History of TonsillectomyDocument9 pagesHistory of TonsillectomyDr. T. Balasubramanian100% (1)
- KASP Package RateDocument502 pagesKASP Package RateAnoop VijayakumarNo ratings yet
- AFIB Cases For StudentsDocument72 pagesAFIB Cases For StudentsYam PiudikNo ratings yet
- AF Catheter AblationDocument37 pagesAF Catheter AblationSnehal JayaramNo ratings yet
- Ishemic Heart Disease-y-II-2011 (Student Version)Document51 pagesIshemic Heart Disease-y-II-2011 (Student Version)kays30002403No ratings yet
- Sao GuidelinesDocument46 pagesSao GuidelinesAlina SarbuNo ratings yet
- 9 Heart MuscleDocument31 pages9 Heart Muscleshoeb4uNo ratings yet
- 13• Peripheral Arterial Disease [Illustrations Key]Document2 pages13• Peripheral Arterial Disease [Illustrations Key]blazesj7796No ratings yet
- Severity Change in TBW Change in ECF CV S/S Cns S/S Other S/S LabsDocument2 pagesSeverity Change in TBW Change in ECF CV S/S Cns S/S Other S/S LabsGregNo ratings yet
- Disease of The Aorta: Dr. Edmond L. Jim, SPJP (K), FihaDocument40 pagesDisease of The Aorta: Dr. Edmond L. Jim, SPJP (K), FihaMark YangNo ratings yet
- Safe FESS To Avoid Complication: CT-scan InterpretationDocument33 pagesSafe FESS To Avoid Complication: CT-scan InterpretationBebekNo ratings yet
- DR Sutarmawan Acute Presentation of Valve SletnosisDocument33 pagesDR Sutarmawan Acute Presentation of Valve SletnosisArniNo ratings yet
- 10 - Aortic Diseases (Illustrations Key)Document2 pages10 - Aortic Diseases (Illustrations Key)Asingwire BelindaNo ratings yet
- COPD - Changing Concepts of Pathogenesis and New Ideas For Old TreatmentsDocument49 pagesCOPD - Changing Concepts of Pathogenesis and New Ideas For Old TreatmentsMikee MoganNo ratings yet
- Severe Aortic Stenosis and TavrDocument67 pagesSevere Aortic Stenosis and TavrnaimNo ratings yet
- Derrame - Pleural 20Document58 pagesDerrame - Pleural 20LIZBETH EMMA QUENTA LIMACHINo ratings yet
- CV 3 PHDocument15 pagesCV 3 PHaya najemNo ratings yet
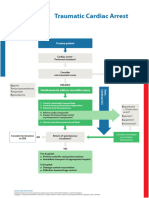
- Poster SpecCircs Traumatic Cardiac Arrest Algorithm SERB V20160714 HRESDocument1 pagePoster SpecCircs Traumatic Cardiac Arrest Algorithm SERB V20160714 HRESJelena TadićNo ratings yet
- Jantung - Acute Heart FailureDocument32 pagesJantung - Acute Heart FailurefaradibaNo ratings yet
- Partial Embolization of Splenic ArteryDocument2 pagesPartial Embolization of Splenic Arteryshamaamo19No ratings yet
- OHQ NewsLetter - Vol12 - Afib - 1112 - ENDocument5 pagesOHQ NewsLetter - Vol12 - Afib - 1112 - ENherryaptNo ratings yet
- Jenis ShockDocument6 pagesJenis ShockMuhamad Pathu RohmanNo ratings yet
- Atrial Flutter: The Lancet Carotid Sinus MassageDocument3 pagesAtrial Flutter: The Lancet Carotid Sinus Massageyosi rizalNo ratings yet
- Acute Limb Ischemia (Ali) : Tributed To: Ismoyo Sunu, MDDocument54 pagesAcute Limb Ischemia (Ali) : Tributed To: Ismoyo Sunu, MDMhd Ridho FahreziNo ratings yet
- Echophonocardiographic Study of The Initial Low Frequency Component of The First Heart SoundDocument7 pagesEchophonocardiographic Study of The Initial Low Frequency Component of The First Heart SoundMi-liz RamirezNo ratings yet
- Obstruc (Ve Sleep Apnea: An Overview: Clinical Commi8ee Society of Anesthesia and Sleep MedicineDocument41 pagesObstruc (Ve Sleep Apnea: An Overview: Clinical Commi8ee Society of Anesthesia and Sleep MedicinepuneetNo ratings yet
- Safe FESS To Avoid Complication: CT-scan InterpretationDocument33 pagesSafe FESS To Avoid Complication: CT-scan InterpretationBebekNo ratings yet
- Jenis ShockDocument6 pagesJenis ShockMUHAMAD PATHU ROHMANNo ratings yet
- Cardio CostanzoDocument71 pagesCardio CostanzoShellz2428No ratings yet
- Anatomy Physiology of The CV SystemDocument29 pagesAnatomy Physiology of The CV SystemMaedehNo ratings yet
- Surgery Ospe 322Document322 pagesSurgery Ospe 322fbf50269No ratings yet
- Critical Care Cheat Sheet FreebieDocument2 pagesCritical Care Cheat Sheet FreebieJeshan Yanong Beltran100% (1)
- Emphysema IEDocument22 pagesEmphysema IEFrnz RiveraNo ratings yet
- Cardiac CycleDocument7 pagesCardiac CycleKrishnakanth NNo ratings yet
- Case 1: Peripheral Vascular Disease: An OverviewDocument11 pagesCase 1: Peripheral Vascular Disease: An OverviewAmita PatelNo ratings yet
- Operative SummaryDocument1 pageOperative SummarynasimNo ratings yet
- Aurigemma Haemodynamics 2021 SlidesDocument67 pagesAurigemma Haemodynamics 2021 SlidesSajjad HussainNo ratings yet
- Congenital Heart Defects: Part Ii-Duct Dependent ChdsDocument28 pagesCongenital Heart Defects: Part Ii-Duct Dependent ChdslindaNo ratings yet
- Secdocument - 89download Echocardiography A Practical Guide For Reporting and Interpretation 4E John Chambers Full ChapterDocument67 pagesSecdocument - 89download Echocardiography A Practical Guide For Reporting and Interpretation 4E John Chambers Full Chapterjeremy.west757100% (12)
- Stroke: Problem Dan PenatalaksanaanyaDocument40 pagesStroke: Problem Dan PenatalaksanaanyakhatabNo ratings yet
- Poster SpecCircs Traumatic Cardiac Arrest Algorithm ENG V20151005 HRES SiteDocument1 pagePoster SpecCircs Traumatic Cardiac Arrest Algorithm ENG V20151005 HRES SiteangelologrilloNo ratings yet
- AP 2 PCW #2 - Cardiovascular - Module 3.3-3.6Document4 pagesAP 2 PCW #2 - Cardiovascular - Module 3.3-3.6eemma.pokemonNo ratings yet
- Vats Bullectomy: Initial Shillong ExperienceDocument21 pagesVats Bullectomy: Initial Shillong ExperiencelmdarlongNo ratings yet
- Leaflet-Fast en WebDocument2 pagesLeaflet-Fast en WebASHUTOSH MOHANTYNo ratings yet
- Osce AnasDocument62 pagesOsce AnasMohammad FuadNo ratings yet
- Diastole and AnesthesiaDocument16 pagesDiastole and AnesthesiadrsubramanianNo ratings yet
- Peter Hudson Blood TransfusionDocument29 pagesPeter Hudson Blood TransfusionMorris KiioNo ratings yet
- Arteriovenous Malformation 1001Document19 pagesArteriovenous Malformation 1001housic1No ratings yet
- Persiapan Osce Nasional: Dept. Obstetri Dan Ginekologi FK UnairDocument5 pagesPersiapan Osce Nasional: Dept. Obstetri Dan Ginekologi FK UnairYanis Widhiya NingrumNo ratings yet
- Valvular Heart Diseases Part 2 - Dr. BartolomeDocument9 pagesValvular Heart Diseases Part 2 - Dr. BartolomeMedisina101No ratings yet
- Physiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Document62 pagesPhysiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Akshay ChaudharyNo ratings yet
- Lung Function Tests: Yazeed Abed El KhaleqDocument35 pagesLung Function Tests: Yazeed Abed El KhaleqYazeedNo ratings yet
- Aortic StenosisDocument8 pagesAortic Stenosisdr.moni.co.ukNo ratings yet
- CIRCULAȚIE FeTALĂDocument2 pagesCIRCULAȚIE FeTALĂAurelia AlexandraNo ratings yet
- Shock AtfDocument23 pagesShock Atfyahomed519No ratings yet
- Physiology Lab Final 4Document10 pagesPhysiology Lab Final 4Era NewNo ratings yet
- The Echo Exam: Echo Findings in EndocarditisDocument1 pageThe Echo Exam: Echo Findings in EndocarditisYanNo ratings yet
- Sistema Cardiovascular IiDocument20 pagesSistema Cardiovascular Iipark Hyo HyeNo ratings yet
- Acute Management of Pelvic Ring Injuries: Kyle F. Dickson, MDDocument121 pagesAcute Management of Pelvic Ring Injuries: Kyle F. Dickson, MDSatrio Bangun NegoroNo ratings yet
- Case Study 102 Ob NCP Labs DrugsDocument15 pagesCase Study 102 Ob NCP Labs DrugsZena TerresNo ratings yet
- Advances in Treatments for Aortic Valve and Root DiseasesFrom EverandAdvances in Treatments for Aortic Valve and Root DiseasesKhalil FattouchNo ratings yet
- Analgesia and Anesthesia in ObstetricsDocument5 pagesAnalgesia and Anesthesia in ObstetricsĶHwola ƏľsHokryNo ratings yet
- Mesenteric LymphadenopathyDocument5 pagesMesenteric LymphadenopathyManorama KusalakarNo ratings yet
- Assessment and Management of Preoperative AnxietyDocument6 pagesAssessment and Management of Preoperative AnxietyFiorel Loves EveryoneNo ratings yet
- Liceo de Cagayan University: College of Medical Laboratory ScienceDocument5 pagesLiceo de Cagayan University: College of Medical Laboratory ScienceBianca Cielo BalabagNo ratings yet
- Ontent Reviewers: ContributorsDocument14 pagesOntent Reviewers: ContributorsAgnes TanicNo ratings yet
- Dr. Ahlam Al-Kharabsheh: Assistant Professor, OBS & GYN Department Mu'tah UniversityDocument36 pagesDr. Ahlam Al-Kharabsheh: Assistant Professor, OBS & GYN Department Mu'tah Universityraed faisalNo ratings yet
- Systematic Review - Cardiac LipomaDocument7 pagesSystematic Review - Cardiac LipomaEspecialização EcocardiografiaNo ratings yet
- Guiding Catheter 2Document3 pagesGuiding Catheter 2Sara MartínezNo ratings yet
- Le Fort FracturesDocument8 pagesLe Fort FracturesSeiska RbNo ratings yet
- Interdisciplinary Seminar - CLPDocument80 pagesInterdisciplinary Seminar - CLPSharanya Bose100% (1)
- Applied Sciences: 3D Soft-Tissue Prediction Methodologies For Orthognathic Surgery-A Literature ReviewDocument23 pagesApplied Sciences: 3D Soft-Tissue Prediction Methodologies For Orthognathic Surgery-A Literature ReviewMairen RamirezNo ratings yet
- EpicHospitalAhmedabad BrochureDocument32 pagesEpicHospitalAhmedabad Brochurerakesh jayal100% (1)
- Nursing Workload Icu 2017Document5 pagesNursing Workload Icu 2017Meiriele TavaresNo ratings yet
- Jude's Quadriceps Plasty For Stiff KneeDocument6 pagesJude's Quadriceps Plasty For Stiff KneeRaviNo ratings yet
- Pronto ProcedureDocument6 pagesPronto ProcedurewarmanlicyNo ratings yet
- CARDIO Lab ManualDocument15 pagesCARDIO Lab ManualApril Joy de LimaNo ratings yet
- Neurocritical Care Management of The Neurosurgical Patient 1St Edition Edition Monisha Kumar Full ChapterDocument67 pagesNeurocritical Care Management of The Neurosurgical Patient 1St Edition Edition Monisha Kumar Full Chapteramelia.bradham272100% (13)
- UrinaryDocument3 pagesUrinarySeaNo ratings yet
- Robotic Technology in Foot and Ankle Surgery: A Comprehensive ReviewDocument15 pagesRobotic Technology in Foot and Ankle Surgery: A Comprehensive Reviewzainaalhashimi101No ratings yet
- Bubble CPAP Vs Ventilatory CPAPDocument9 pagesBubble CPAP Vs Ventilatory CPAPRyan Rahman OesmanNo ratings yet
- ECG - ACLS 2020 ModuleDocument68 pagesECG - ACLS 2020 ModuleRasheedAladdinNGuiomala100% (1)
- Whole Spine MriDocument2 pagesWhole Spine MriImg UsmleNo ratings yet
- Hospital Rate ChartDocument3 pagesHospital Rate ChartSuhana ParvinNo ratings yet
- MD MDCG 2019 14 MDR Codes enDocument23 pagesMD MDCG 2019 14 MDR Codes enLeilNo ratings yet
- Hydrocele - PILDocument3 pagesHydrocele - PILBrama Trisna WasessaNo ratings yet
- Elektrokardiograf: Prof. Dr. Peter KaboDocument56 pagesElektrokardiograf: Prof. Dr. Peter KaboAchmad DamnhuriNo ratings yet
- Genital ProlapseDocument9 pagesGenital Prolapsesher singhNo ratings yet
- VESICULAR NEW Lession PlanDocument18 pagesVESICULAR NEW Lession PlanRaj JadhavNo ratings yet








![13• Peripheral Arterial Disease [Illustrations Key]](https://imgv2-2-f.scribdassets.com/img/document/747818519/149x198/cdb21609ca/1720079270?v=1)













































































Download as ppt, pdf, or txt
You might also like
- 9 - Internal Medicine Buzzwords Handout Oct 2023 John Michael RuizDocument8 pages9 - Internal Medicine Buzzwords Handout Oct 2023 John Michael RuizJohn Michael RuizNo ratings yet
- History of TonsillectomyDocument9 pagesHistory of TonsillectomyDr. T. Balasubramanian100% (1)
- KASP Package RateDocument502 pagesKASP Package RateAnoop VijayakumarNo ratings yet
- AFIB Cases For StudentsDocument72 pagesAFIB Cases For StudentsYam PiudikNo ratings yet
- AF Catheter AblationDocument37 pagesAF Catheter AblationSnehal JayaramNo ratings yet
- Ishemic Heart Disease-y-II-2011 (Student Version)Document51 pagesIshemic Heart Disease-y-II-2011 (Student Version)kays30002403No ratings yet
- Sao GuidelinesDocument46 pagesSao GuidelinesAlina SarbuNo ratings yet
- 9 Heart MuscleDocument31 pages9 Heart Muscleshoeb4uNo ratings yet
- 13• Peripheral Arterial Disease [Illustrations Key]Document2 pages13• Peripheral Arterial Disease [Illustrations Key]blazesj7796No ratings yet
- Severity Change in TBW Change in ECF CV S/S Cns S/S Other S/S LabsDocument2 pagesSeverity Change in TBW Change in ECF CV S/S Cns S/S Other S/S LabsGregNo ratings yet
- Disease of The Aorta: Dr. Edmond L. Jim, SPJP (K), FihaDocument40 pagesDisease of The Aorta: Dr. Edmond L. Jim, SPJP (K), FihaMark YangNo ratings yet
- Safe FESS To Avoid Complication: CT-scan InterpretationDocument33 pagesSafe FESS To Avoid Complication: CT-scan InterpretationBebekNo ratings yet
- DR Sutarmawan Acute Presentation of Valve SletnosisDocument33 pagesDR Sutarmawan Acute Presentation of Valve SletnosisArniNo ratings yet
- 10 - Aortic Diseases (Illustrations Key)Document2 pages10 - Aortic Diseases (Illustrations Key)Asingwire BelindaNo ratings yet
- COPD - Changing Concepts of Pathogenesis and New Ideas For Old TreatmentsDocument49 pagesCOPD - Changing Concepts of Pathogenesis and New Ideas For Old TreatmentsMikee MoganNo ratings yet
- Severe Aortic Stenosis and TavrDocument67 pagesSevere Aortic Stenosis and TavrnaimNo ratings yet
- Derrame - Pleural 20Document58 pagesDerrame - Pleural 20LIZBETH EMMA QUENTA LIMACHINo ratings yet
- CV 3 PHDocument15 pagesCV 3 PHaya najemNo ratings yet
- Poster SpecCircs Traumatic Cardiac Arrest Algorithm SERB V20160714 HRESDocument1 pagePoster SpecCircs Traumatic Cardiac Arrest Algorithm SERB V20160714 HRESJelena TadićNo ratings yet
- Jantung - Acute Heart FailureDocument32 pagesJantung - Acute Heart FailurefaradibaNo ratings yet
- Partial Embolization of Splenic ArteryDocument2 pagesPartial Embolization of Splenic Arteryshamaamo19No ratings yet
- OHQ NewsLetter - Vol12 - Afib - 1112 - ENDocument5 pagesOHQ NewsLetter - Vol12 - Afib - 1112 - ENherryaptNo ratings yet
- Jenis ShockDocument6 pagesJenis ShockMuhamad Pathu RohmanNo ratings yet
- Atrial Flutter: The Lancet Carotid Sinus MassageDocument3 pagesAtrial Flutter: The Lancet Carotid Sinus Massageyosi rizalNo ratings yet
- Acute Limb Ischemia (Ali) : Tributed To: Ismoyo Sunu, MDDocument54 pagesAcute Limb Ischemia (Ali) : Tributed To: Ismoyo Sunu, MDMhd Ridho FahreziNo ratings yet
- Echophonocardiographic Study of The Initial Low Frequency Component of The First Heart SoundDocument7 pagesEchophonocardiographic Study of The Initial Low Frequency Component of The First Heart SoundMi-liz RamirezNo ratings yet
- Obstruc (Ve Sleep Apnea: An Overview: Clinical Commi8ee Society of Anesthesia and Sleep MedicineDocument41 pagesObstruc (Ve Sleep Apnea: An Overview: Clinical Commi8ee Society of Anesthesia and Sleep MedicinepuneetNo ratings yet
- Safe FESS To Avoid Complication: CT-scan InterpretationDocument33 pagesSafe FESS To Avoid Complication: CT-scan InterpretationBebekNo ratings yet
- Jenis ShockDocument6 pagesJenis ShockMUHAMAD PATHU ROHMANNo ratings yet
- Cardio CostanzoDocument71 pagesCardio CostanzoShellz2428No ratings yet
- Anatomy Physiology of The CV SystemDocument29 pagesAnatomy Physiology of The CV SystemMaedehNo ratings yet
- Surgery Ospe 322Document322 pagesSurgery Ospe 322fbf50269No ratings yet
- Critical Care Cheat Sheet FreebieDocument2 pagesCritical Care Cheat Sheet FreebieJeshan Yanong Beltran100% (1)
- Emphysema IEDocument22 pagesEmphysema IEFrnz RiveraNo ratings yet
- Cardiac CycleDocument7 pagesCardiac CycleKrishnakanth NNo ratings yet
- Case 1: Peripheral Vascular Disease: An OverviewDocument11 pagesCase 1: Peripheral Vascular Disease: An OverviewAmita PatelNo ratings yet
- Operative SummaryDocument1 pageOperative SummarynasimNo ratings yet
- Aurigemma Haemodynamics 2021 SlidesDocument67 pagesAurigemma Haemodynamics 2021 SlidesSajjad HussainNo ratings yet
- Congenital Heart Defects: Part Ii-Duct Dependent ChdsDocument28 pagesCongenital Heart Defects: Part Ii-Duct Dependent ChdslindaNo ratings yet
- Secdocument - 89download Echocardiography A Practical Guide For Reporting and Interpretation 4E John Chambers Full ChapterDocument67 pagesSecdocument - 89download Echocardiography A Practical Guide For Reporting and Interpretation 4E John Chambers Full Chapterjeremy.west757100% (12)
- Stroke: Problem Dan PenatalaksanaanyaDocument40 pagesStroke: Problem Dan PenatalaksanaanyakhatabNo ratings yet
- Poster SpecCircs Traumatic Cardiac Arrest Algorithm ENG V20151005 HRES SiteDocument1 pagePoster SpecCircs Traumatic Cardiac Arrest Algorithm ENG V20151005 HRES SiteangelologrilloNo ratings yet
- AP 2 PCW #2 - Cardiovascular - Module 3.3-3.6Document4 pagesAP 2 PCW #2 - Cardiovascular - Module 3.3-3.6eemma.pokemonNo ratings yet
- Vats Bullectomy: Initial Shillong ExperienceDocument21 pagesVats Bullectomy: Initial Shillong ExperiencelmdarlongNo ratings yet
- Leaflet-Fast en WebDocument2 pagesLeaflet-Fast en WebASHUTOSH MOHANTYNo ratings yet
- Osce AnasDocument62 pagesOsce AnasMohammad FuadNo ratings yet
- Diastole and AnesthesiaDocument16 pagesDiastole and AnesthesiadrsubramanianNo ratings yet
- Peter Hudson Blood TransfusionDocument29 pagesPeter Hudson Blood TransfusionMorris KiioNo ratings yet
- Arteriovenous Malformation 1001Document19 pagesArteriovenous Malformation 1001housic1No ratings yet
- Persiapan Osce Nasional: Dept. Obstetri Dan Ginekologi FK UnairDocument5 pagesPersiapan Osce Nasional: Dept. Obstetri Dan Ginekologi FK UnairYanis Widhiya NingrumNo ratings yet
- Valvular Heart Diseases Part 2 - Dr. BartolomeDocument9 pagesValvular Heart Diseases Part 2 - Dr. BartolomeMedisina101No ratings yet
- Physiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Document62 pagesPhysiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Akshay ChaudharyNo ratings yet
- Lung Function Tests: Yazeed Abed El KhaleqDocument35 pagesLung Function Tests: Yazeed Abed El KhaleqYazeedNo ratings yet
- Aortic StenosisDocument8 pagesAortic Stenosisdr.moni.co.ukNo ratings yet
- CIRCULAȚIE FeTALĂDocument2 pagesCIRCULAȚIE FeTALĂAurelia AlexandraNo ratings yet
- Shock AtfDocument23 pagesShock Atfyahomed519No ratings yet
- Physiology Lab Final 4Document10 pagesPhysiology Lab Final 4Era NewNo ratings yet
- The Echo Exam: Echo Findings in EndocarditisDocument1 pageThe Echo Exam: Echo Findings in EndocarditisYanNo ratings yet
- Sistema Cardiovascular IiDocument20 pagesSistema Cardiovascular Iipark Hyo HyeNo ratings yet
- Acute Management of Pelvic Ring Injuries: Kyle F. Dickson, MDDocument121 pagesAcute Management of Pelvic Ring Injuries: Kyle F. Dickson, MDSatrio Bangun NegoroNo ratings yet
- Case Study 102 Ob NCP Labs DrugsDocument15 pagesCase Study 102 Ob NCP Labs DrugsZena TerresNo ratings yet
- Advances in Treatments for Aortic Valve and Root DiseasesFrom EverandAdvances in Treatments for Aortic Valve and Root DiseasesKhalil FattouchNo ratings yet
- Analgesia and Anesthesia in ObstetricsDocument5 pagesAnalgesia and Anesthesia in ObstetricsĶHwola ƏľsHokryNo ratings yet
- Mesenteric LymphadenopathyDocument5 pagesMesenteric LymphadenopathyManorama KusalakarNo ratings yet
- Assessment and Management of Preoperative AnxietyDocument6 pagesAssessment and Management of Preoperative AnxietyFiorel Loves EveryoneNo ratings yet
- Liceo de Cagayan University: College of Medical Laboratory ScienceDocument5 pagesLiceo de Cagayan University: College of Medical Laboratory ScienceBianca Cielo BalabagNo ratings yet
- Ontent Reviewers: ContributorsDocument14 pagesOntent Reviewers: ContributorsAgnes TanicNo ratings yet
- Dr. Ahlam Al-Kharabsheh: Assistant Professor, OBS & GYN Department Mu'tah UniversityDocument36 pagesDr. Ahlam Al-Kharabsheh: Assistant Professor, OBS & GYN Department Mu'tah Universityraed faisalNo ratings yet
- Systematic Review - Cardiac LipomaDocument7 pagesSystematic Review - Cardiac LipomaEspecialização EcocardiografiaNo ratings yet
- Guiding Catheter 2Document3 pagesGuiding Catheter 2Sara MartínezNo ratings yet
- Le Fort FracturesDocument8 pagesLe Fort FracturesSeiska RbNo ratings yet
- Interdisciplinary Seminar - CLPDocument80 pagesInterdisciplinary Seminar - CLPSharanya Bose100% (1)
- Applied Sciences: 3D Soft-Tissue Prediction Methodologies For Orthognathic Surgery-A Literature ReviewDocument23 pagesApplied Sciences: 3D Soft-Tissue Prediction Methodologies For Orthognathic Surgery-A Literature ReviewMairen RamirezNo ratings yet
- EpicHospitalAhmedabad BrochureDocument32 pagesEpicHospitalAhmedabad Brochurerakesh jayal100% (1)
- Nursing Workload Icu 2017Document5 pagesNursing Workload Icu 2017Meiriele TavaresNo ratings yet
- Jude's Quadriceps Plasty For Stiff KneeDocument6 pagesJude's Quadriceps Plasty For Stiff KneeRaviNo ratings yet
- Pronto ProcedureDocument6 pagesPronto ProcedurewarmanlicyNo ratings yet
- CARDIO Lab ManualDocument15 pagesCARDIO Lab ManualApril Joy de LimaNo ratings yet
- Neurocritical Care Management of The Neurosurgical Patient 1St Edition Edition Monisha Kumar Full ChapterDocument67 pagesNeurocritical Care Management of The Neurosurgical Patient 1St Edition Edition Monisha Kumar Full Chapteramelia.bradham272100% (13)
- UrinaryDocument3 pagesUrinarySeaNo ratings yet
- Robotic Technology in Foot and Ankle Surgery: A Comprehensive ReviewDocument15 pagesRobotic Technology in Foot and Ankle Surgery: A Comprehensive Reviewzainaalhashimi101No ratings yet
- Bubble CPAP Vs Ventilatory CPAPDocument9 pagesBubble CPAP Vs Ventilatory CPAPRyan Rahman OesmanNo ratings yet
- ECG - ACLS 2020 ModuleDocument68 pagesECG - ACLS 2020 ModuleRasheedAladdinNGuiomala100% (1)
- Whole Spine MriDocument2 pagesWhole Spine MriImg UsmleNo ratings yet
- Hospital Rate ChartDocument3 pagesHospital Rate ChartSuhana ParvinNo ratings yet
- MD MDCG 2019 14 MDR Codes enDocument23 pagesMD MDCG 2019 14 MDR Codes enLeilNo ratings yet
- Hydrocele - PILDocument3 pagesHydrocele - PILBrama Trisna WasessaNo ratings yet
- Elektrokardiograf: Prof. Dr. Peter KaboDocument56 pagesElektrokardiograf: Prof. Dr. Peter KaboAchmad DamnhuriNo ratings yet
- Genital ProlapseDocument9 pagesGenital Prolapsesher singhNo ratings yet
- VESICULAR NEW Lession PlanDocument18 pagesVESICULAR NEW Lession PlanRaj JadhavNo ratings yet