Download as pptx, pdf, or txt
You might also like
- Case Study On MalariaDocument18 pagesCase Study On MalariaBie WeNna100% (4)
- PEDS Exam 2 - OutlineDocument67 pagesPEDS Exam 2 - OutlineBonquisha OrgamiNo ratings yet
- Obs Gynae Full Summary NotesDocument41 pagesObs Gynae Full Summary NotesJana Aldour100% (1)
- Maternal ATIDocument6 pagesMaternal ATIGeorgeNo ratings yet
- Tuberculosis QsenDocument22 pagesTuberculosis Qsenapi-534410130No ratings yet
- Chapter 09: Photo Atlas of Drug Administration Test Bank: Multiple ChoiceDocument8 pagesChapter 09: Photo Atlas of Drug Administration Test Bank: Multiple ChoicePrettygirl716No ratings yet
- Premature Rupture of MembranesDocument5 pagesPremature Rupture of MembranesAnonymous pYR4s37H6No ratings yet
- Antepartum 1Document3 pagesAntepartum 1Emily DavisNo ratings yet
- Hesi PracticeDocument1 pageHesi Practicejustjesko0lNo ratings yet
- Kaplan Focus ReviewDocument9 pagesKaplan Focus ReviewSaidel ElizondoNo ratings yet
- Abruptio Placentae Nursing Quiz: Start StartDocument6 pagesAbruptio Placentae Nursing Quiz: Start StartLot Rosit100% (1)
- VSim SARAH LIN For Nursing - Health Assessment POST QUIZDocument5 pagesVSim SARAH LIN For Nursing - Health Assessment POST QUIZWen RodsaNo ratings yet
- Urinary System DisordersDocument14 pagesUrinary System DisordersGideon P. CasasNo ratings yet
- Pediatric Pharmacology 07Document45 pagesPediatric Pharmacology 07Nadz CyNo ratings yet
- ATI RN Nursing Care of Children Online Practice 2019 ADocument4 pagesATI RN Nursing Care of Children Online Practice 2019 Aianshirow834No ratings yet
- MS Final 46 Blood or Lymphatic DisorderDocument4 pagesMS Final 46 Blood or Lymphatic DisorderZachary T Hall0% (1)
- Peds Exam 3Document61 pagesPeds Exam 3Katie Morgan EdwardsNo ratings yet
- HESI 2015 Maternal New Born Specialty AnswersDocument2 pagesHESI 2015 Maternal New Born Specialty AnswersAnaGranara100% (3)
- OB Exam 1 ComboDocument82 pagesOB Exam 1 ComboHope RobersonNo ratings yet
- Study - Blueprint P2Document26 pagesStudy - Blueprint P2Natasha Drummond100% (1)
- Hyperemesis Gravidarum: Bleeding Complications of PregnancyDocument6 pagesHyperemesis Gravidarum: Bleeding Complications of PregnancykirbsNo ratings yet
- Medical-Surgical Nursing: Perioperative OverviewDocument24 pagesMedical-Surgical Nursing: Perioperative OverviewSheena Ann L. LLarenasNo ratings yet
- NclexDocument4 pagesNclexihatetouNo ratings yet
- U World ReproductiveDocument5 pagesU World ReproductiveAce LabosNo ratings yet
- Intra PartumDocument7 pagesIntra PartumFreisanChenMandumotanNo ratings yet
- Argumentative Essay-Due Oct 22ndDocument4 pagesArgumentative Essay-Due Oct 22ndapi-624641638No ratings yet
- Gastric and Duodenal Disorders - Test 4Document21 pagesGastric and Duodenal Disorders - Test 4Vickie BuckerNo ratings yet
- NCLEX Quick FactsDocument7 pagesNCLEX Quick FactsMary Aurine FullanteNo ratings yet
- Drugs in The Neonatal Unit: 1 Julia PettyDocument5 pagesDrugs in The Neonatal Unit: 1 Julia PettyMarjoNo ratings yet
- UWorld Critical CareDocument14 pagesUWorld Critical CareJohnasse Sebastian NavalNo ratings yet
- HESIDocument2 pagesHESIElizabeth100% (1)
- Chapter 41: The Child With An Infectious Disease Test Bank: Multiple ChoiceDocument10 pagesChapter 41: The Child With An Infectious Disease Test Bank: Multiple ChoiceNurse UtopiaNo ratings yet
- Which Signs and Symptoms Would The Nurse Expect To Assess in A Newborn WithDocument1 pageWhich Signs and Symptoms Would The Nurse Expect To Assess in A Newborn WithjamesNo ratings yet
- Pedia Note1Document38 pagesPedia Note1FreeNursingNotes100% (1)
- Hurst Review CDC Infection Control ChartDocument44 pagesHurst Review CDC Infection Control ChartTerry Thun100% (2)
- Maternal Neonatal Facts, 2EDocument112 pagesMaternal Neonatal Facts, 2Earcci balinasNo ratings yet
- Asthma That Disappears Between Ages 6-8 - Bronchioles Grew & Resolved The AsthmaDocument27 pagesAsthma That Disappears Between Ages 6-8 - Bronchioles Grew & Resolved The Asthmasimonedarling100% (1)
- Respiratory Disorders of Pediatric Clients - NCLEX - HPMDocument35 pagesRespiratory Disorders of Pediatric Clients - NCLEX - HPMNadesNo ratings yet
- ATI Community Health Proctored Exam 2020Document7 pagesATI Community Health Proctored Exam 20204 u0% (1)
- Lippincott's REPRODUCTIVE PROBLEMSDocument14 pagesLippincott's REPRODUCTIVE PROBLEMSNursyNurseNo ratings yet
- Ladewig 8e TIF Ch04 PDFDocument12 pagesLadewig 8e TIF Ch04 PDFjames smithNo ratings yet
- UntitledDocument41 pagesUntitledvioletdeocaresNo ratings yet
- Med Surg 1 Exam 1Document23 pagesMed Surg 1 Exam 1Breeana MooreNo ratings yet
- FNP Final TestDocument10 pagesFNP Final TestNelson MandelaNo ratings yet
- 8 Essential Concepts 4 NCLEX RN-4Document6 pages8 Essential Concepts 4 NCLEX RN-4Jot grewalNo ratings yet
- Infection Control - NclexDocument4 pagesInfection Control - NclexTashaNo ratings yet
- ARDS (Acute Respiratory Distress Syndrome) : EarlyDocument1 pageARDS (Acute Respiratory Distress Syndrome) : EarlyDora Elena HurtadoNo ratings yet
- Brochure Cancer Bush PDFDocument2 pagesBrochure Cancer Bush PDFKaren SwanepoelNo ratings yet
- What Are Sexually Transmitted Diseases (STDS) ?Document24 pagesWhat Are Sexually Transmitted Diseases (STDS) ?Safiqah AinNo ratings yet
- Hematologic System2Document70 pagesHematologic System2Jesus Mario LopezNo ratings yet
- Exam ReviewDocument4 pagesExam ReviewMya Thomas100% (1)
- 52 Nclex ReviewDocument1 page52 Nclex ReviewedobleNo ratings yet
- Care of NewornDocument4 pagesCare of NewornArchana SahuNo ratings yet
- 1) CORRECT - Nurse Must Follow Chain of Command: DepressionDocument18 pages1) CORRECT - Nurse Must Follow Chain of Command: DepressionLily De Fiallo'sNo ratings yet
- Oncology NursingDocument21 pagesOncology NursingAqib SatarNo ratings yet
- Respi SystemDocument6 pagesRespi SystemKalichandren ArumugamNo ratings yet
- Immunity 1Document6 pagesImmunity 1Tori RolandNo ratings yet
- Roth 10e Nclex Chapter 11Document4 pagesRoth 10e Nclex Chapter 11jennaaahhhNo ratings yet
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Fatigue Weaknessdecreased Oral Intake Respiration ChangesDocument15 pagesFatigue Weaknessdecreased Oral Intake Respiration ChangesJane Ann AlolodNo ratings yet
- Genogram SymbolsDocument1 pageGenogram SymbolsJane Ann AlolodNo ratings yet
- Breast CancerDocument40 pagesBreast CancerJane Ann AlolodNo ratings yet
- Acute Glomerulonephritis 1Document19 pagesAcute Glomerulonephritis 1Jane Ann AlolodNo ratings yet
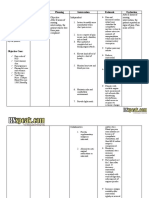
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective CueDocument3 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective CueJane Ann AlolodNo ratings yet
- Burns and InjuryDocument27 pagesBurns and InjuryJane Ann Alolod100% (1)
- Purposive Communication: Jane Ann C.AlolodDocument8 pagesPurposive Communication: Jane Ann C.AlolodJane Ann AlolodNo ratings yet
- Statement of The ProblemDocument1 pageStatement of The ProblemJane Ann AlolodNo ratings yet
- KIDNEY AND URINARY TRACT PROBLEMS Edited (Autosaved)Document29 pagesKIDNEY AND URINARY TRACT PROBLEMS Edited (Autosaved)Jane Ann AlolodNo ratings yet
- Mahabharata SummaryDocument24 pagesMahabharata SummaryJane Ann AlolodNo ratings yet
- Perioperative LectDocument134 pagesPerioperative LectJane Ann AlolodNo ratings yet
- Nursing Management of Cystic FibrosisDocument2 pagesNursing Management of Cystic FibrosisJane Ann AlolodNo ratings yet
- Pathophysiology of Chorioamnionitis: Predisposing FactorsDocument1 pagePathophysiology of Chorioamnionitis: Predisposing FactorsJane Ann AlolodNo ratings yet
- Abortion and MiscarriageDocument38 pagesAbortion and MiscarriageJane Ann AlolodNo ratings yet
- " I Am Sam": Just A Home, Not A Baby, This Is Not My Life". and That Makes Mr. Sam Dawson A Single Father, Despite HisDocument3 pages" I Am Sam": Just A Home, Not A Baby, This Is Not My Life". and That Makes Mr. Sam Dawson A Single Father, Despite HisJane Ann AlolodNo ratings yet
- Muscarinic Agonist: (Bethanechol)Document2 pagesMuscarinic Agonist: (Bethanechol)Jane Ann AlolodNo ratings yet
- Muscarinic Agonist (Bethanechol) : By: Jane Ann C. AlolodDocument15 pagesMuscarinic Agonist (Bethanechol) : By: Jane Ann C. AlolodJane Ann AlolodNo ratings yet
- JANE Ward ClassDocument9 pagesJANE Ward ClassJane Ann AlolodNo ratings yet
- Pre Audiometry QuestioniareDocument1 pagePre Audiometry QuestioniareNtainda KantalambaNo ratings yet
- DNA VaccinesDocument2 pagesDNA VaccinesAmeena AimenNo ratings yet
- Orchitis (Eng)Document15 pagesOrchitis (Eng)Ferzy Awwali FadhilaNo ratings yet
- E.O Sereis of 2020 Bhert ReactivationDocument2 pagesE.O Sereis of 2020 Bhert ReactivationQUeen Dai SY RamirezNo ratings yet
- Gram Positive RodsDocument15 pagesGram Positive RodsMarc Imhotep Cray, M.D.No ratings yet
- Antifungal DrugsDocument66 pagesAntifungal DrugsMalueth AnguiNo ratings yet
- 1) Serology - IntroductionDocument5 pages1) Serology - IntroductionAssem AlmoughrabiNo ratings yet
- KHADIJAHDocument35 pagesKHADIJAHshintya sebayangNo ratings yet
- 10 TBDocument33 pages10 TBamal nassarNo ratings yet
- Chapter 12 Test and Answer KeyDocument3 pagesChapter 12 Test and Answer Keyapi-255802331No ratings yet
- Proponent: Hon. Geralyn C. Baliling: Hon. Junnie P. GabucanDocument6 pagesProponent: Hon. Geralyn C. Baliling: Hon. Junnie P. GabucanBarangay San CarlosNo ratings yet
- 4th Shifting Micro Lab ReviewerDocument154 pages4th Shifting Micro Lab ReviewerJade MonrealNo ratings yet
- Preliminary Checklist - Covid 19 - MolmiDocument2 pagesPreliminary Checklist - Covid 19 - MolmiRohit PatelNo ratings yet
- COVID 19 Vaccine or Death VaccineDocument10 pagesCOVID 19 Vaccine or Death VaccinejanzafarNo ratings yet
- Literature Review of ChickenpoxDocument8 pagesLiterature Review of Chickenpoxfv55wmg4100% (1)
- Malaysian DiseaseDocument16 pagesMalaysian Diseasesofea1121No ratings yet
- Unit 4 Infectious Disease - Modes of TransmissionDocument26 pagesUnit 4 Infectious Disease - Modes of TransmissionEvet Vaxbm100% (1)
- Black Death - Causes, Symptoms & Impact HISTORYDocument1 pageBlack Death - Causes, Symptoms & Impact HISTORYn82fthrmy4No ratings yet
- Community Health Nursing: Instructor MR - Bashar Qasho'o St. Name: Bassam N. Hariri ID: 20710486Document12 pagesCommunity Health Nursing: Instructor MR - Bashar Qasho'o St. Name: Bassam N. Hariri ID: 20710486Bassam Naif HaririNo ratings yet
- Intensified Pulse Polio ImmunisationDocument30 pagesIntensified Pulse Polio ImmunisationAdrishyaNo ratings yet
- BIOS 115 Video 9 VaccinesDocument2 pagesBIOS 115 Video 9 VaccinesShawn EllwoodNo ratings yet
- Blood Bank and Blood TransfusionDocument11 pagesBlood Bank and Blood TransfusionMostafa Adel Ahmd100% (1)
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsPrayagNo ratings yet
- Vaccination IndiaDocument1 pageVaccination IndiaMadhuri AggarwalNo ratings yet
- History Human Parasitology PDFDocument18 pagesHistory Human Parasitology PDFmarianNo ratings yet
- Covid-19 Dashboard - Cases, Deaths and Vaccinations - New ScientistDocument5 pagesCovid-19 Dashboard - Cases, Deaths and Vaccinations - New Scientistchau chiNo ratings yet
- CHN Combined WordDocument88 pagesCHN Combined WordRayne BonifacioNo ratings yet
- DR - Inayati Habib PPRA Peran Manajemen RSDocument43 pagesDR - Inayati Habib PPRA Peran Manajemen RSBudi IstriawanNo ratings yet
- Viral Skin InfectionsDocument28 pagesViral Skin Infectionstolesadereje73No ratings yet