Download as pptx, pdf, or txt
You might also like
- 2) ERC Pre Course MCQDocument5 pages2) ERC Pre Course MCQS Vaibhav100% (2)
- Key Questions in Cardiac SurgeryDocument522 pagesKey Questions in Cardiac SurgeryRenan Petinelli100% (3)
- Study Notes Family MedicineDocument49 pagesStudy Notes Family MedicineMedShare85% (27)
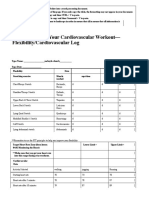
- 4.06 Recording Your Cardiovascular Workout - SchoologyDocument3 pages4.06 Recording Your Cardiovascular Workout - SchoologyMcKayla ChurchNo ratings yet
- All Uworld Notes 2019 Nclex Nursing ResourcesDocument152 pagesAll Uworld Notes 2019 Nclex Nursing Resourcesnene lewis100% (1)
- Braunwald: Chronic Coronary Artery DiseaseDocument122 pagesBraunwald: Chronic Coronary Artery Diseaseusfcards100% (1)
- Aortic Disease and ProceduresDocument58 pagesAortic Disease and ProceduresJ_SteinbergNo ratings yet
- Congenital Heart Disease: Kriti Puri, MD Hugh D. Allen, MD Athar M. Qureshi, MDDocument30 pagesCongenital Heart Disease: Kriti Puri, MD Hugh D. Allen, MD Athar M. Qureshi, MDhari ilman toniNo ratings yet
- Ebstein's AnomalyDocument7 pagesEbstein's AnomalyRJMNo ratings yet
- Cardiovasucular Problems in Children: Niranjana Shalini. M.SC (N) Assistant ProfessorDocument79 pagesCardiovasucular Problems in Children: Niranjana Shalini. M.SC (N) Assistant ProfessorNIRANJANA SHALININo ratings yet
- Clinical Questions Questions Till Nov2022Document17 pagesClinical Questions Questions Till Nov2022Sajol SarkerNo ratings yet
- Mitral Regurgitation Etiology and Pathophysiology: Physical ExaminationsDocument11 pagesMitral Regurgitation Etiology and Pathophysiology: Physical ExaminationsDelmy SanjayaNo ratings yet
- Cardiopulmonary Resuscitation, Oxygen Delivery and Shock - Surgical Critical Care and Emergency Surgery - Wiley Online LibraryDocument8 pagesCardiopulmonary Resuscitation, Oxygen Delivery and Shock - Surgical Critical Care and Emergency Surgery - Wiley Online LibraryValerie ZimmermannNo ratings yet
- Mechanical Complications of AMI-1Document33 pagesMechanical Complications of AMI-1Matthew BanksNo ratings yet
- Cardiopatii Congenitale 17-18 enDocument74 pagesCardiopatii Congenitale 17-18 enMatei PopescuNo ratings yet
- Acute Aortic SyndromeDocument62 pagesAcute Aortic Syndromedr_antonio81No ratings yet
- Intra-Cardiac Angiosarcoma: Case ReportDocument5 pagesIntra-Cardiac Angiosarcoma: Case ReportPeter Paul PascualNo ratings yet
- Surgical Restoration of Ventricular FunctionDocument40 pagesSurgical Restoration of Ventricular FunctionRezwanul Hoque BulbulNo ratings yet
- Oncologic EmergenciesDocument4 pagesOncologic EmergenciesJeffrey RamosNo ratings yet
- Coarctation of The Aorta: P. Syamasundar Rao, MDDocument10 pagesCoarctation of The Aorta: P. Syamasundar Rao, MDAustine OsaweNo ratings yet
- Case Report Missed Connections: Identification of Atrial Septal Defect by MRIDocument4 pagesCase Report Missed Connections: Identification of Atrial Septal Defect by MRIMuhammad Nur Ardhi LahabuNo ratings yet
- Dr. Satyam Rajvanshi Dr. Ram Manohar Lohia Hospital, New DelhiDocument124 pagesDr. Satyam Rajvanshi Dr. Ram Manohar Lohia Hospital, New DelhiazizhaNo ratings yet
- Cardio (1) - 240326 - 233643Document12 pagesCardio (1) - 240326 - 233643Taif SalimNo ratings yet
- Congenital Heart DiseaseDocument74 pagesCongenital Heart DiseaseKeith LajotNo ratings yet
- High Yield Internal Medicine Compatible VersionDocument100 pagesHigh Yield Internal Medicine Compatible VersionAhsan X Baig100% (5)
- Advanced Cardiopulmonary Support For Pulmonary EmbolismDocument6 pagesAdvanced Cardiopulmonary Support For Pulmonary EmbolismJavier Enrique Barrera PachecoNo ratings yet
- Adult Congenital Heart Disease Board ReviewDocument76 pagesAdult Congenital Heart Disease Board ReviewOQAB13No ratings yet
- Tte and Tee Assessment For Asd Closure 2Document88 pagesTte and Tee Assessment For Asd Closure 2Avinash GutheNo ratings yet
- Epicardial ArrythmiasDocument9 pagesEpicardial ArrythmiasTor JaNo ratings yet
- Multimodality Imaging in Sepsis Related Myocardial CalcificationDocument5 pagesMultimodality Imaging in Sepsis Related Myocardial CalcificationRakhmat RamadhaniNo ratings yet
- Imagingofduralarteriovenous Fistula: Jonathan M. MorrisDocument17 pagesImagingofduralarteriovenous Fistula: Jonathan M. MorrisnessimNo ratings yet
- Adult Congenital Heart Disease Board ReviewDocument79 pagesAdult Congenital Heart Disease Board ReviewKhajornsak Som-UnNo ratings yet
- 2nd Case PresentationDocument32 pages2nd Case PresentationMichael PuenteNo ratings yet
- AR Yang Komplikasi Menjadi Gagal Jantung PDFDocument5 pagesAR Yang Komplikasi Menjadi Gagal Jantung PDFFitriani AlawiyahNo ratings yet
- ASD Device ClosureDocument46 pagesASD Device Closuresruthimeena6891No ratings yet
- (Mayo Clinic Proceedings, Dec 2022) - 82 Year Old Man With Chest Pain and Shortness of BreathDocument5 pages(Mayo Clinic Proceedings, Dec 2022) - 82 Year Old Man With Chest Pain and Shortness of BreathNigelyulNo ratings yet
- JZareh Coarctation Aorta Case PresDocument13 pagesJZareh Coarctation Aorta Case PresJesse Helmut Hansen-BartelNo ratings yet
- Chapter 42Document6 pagesChapter 42senjamartiaNo ratings yet
- CHD BookDocument13 pagesCHD BookSanskruthi KurniNo ratings yet
- Caso Clinico Clinica Mayo 2Document5 pagesCaso Clinico Clinica Mayo 2Francisco HernandezNo ratings yet
- (Radiology) RADIOLOGIDocument82 pages(Radiology) RADIOLOGIIrham KhairiNo ratings yet
- Abdominal Aortic AneurysmDocument10 pagesAbdominal Aortic AneurysmPrince K. TaileyNo ratings yet
- Pulmonary Embolism: Here Is Where Your Presentation BeginsDocument39 pagesPulmonary Embolism: Here Is Where Your Presentation BeginsAsmaa ahmedNo ratings yet
- Chronic Mesenteric IschemiaDocument8 pagesChronic Mesenteric IschemiaKrina ShahNo ratings yet
- Ailoaei Et Al 2021 Zero Fluoroscopy Ablation For Atrial Re Entry Via A Vein of Marshall Connection Using A VisibleDocument5 pagesAiloaei Et Al 2021 Zero Fluoroscopy Ablation For Atrial Re Entry Via A Vein of Marshall Connection Using A VisibleAndrés AllaucaNo ratings yet
- Pantent Ductus ArteriosusDocument26 pagesPantent Ductus ArteriosusAmmar AlnajjarNo ratings yet
- CazuriDocument4 pagesCazuriIbănescu Iulia AndreeaNo ratings yet
- Emergency Radiology - Dr. YantoDocument93 pagesEmergency Radiology - Dr. YantoLeonardus William KuswaraNo ratings yet
- Journal of ElectrocardiologyDocument3 pagesJournal of ElectrocardiologyFederico FalsettiNo ratings yet
- Mitral Valve RepairDocument109 pagesMitral Valve RepairheldhiNo ratings yet
- Hemodynamically Stable Left Ventricular Pseudoaneurysm: Who Should Manage - Surgeon or Cardiologist?Document4 pagesHemodynamically Stable Left Ventricular Pseudoaneurysm: Who Should Manage - Surgeon or Cardiologist?asclepiuspdfsNo ratings yet
- Current Readings On Surgery For The Neonate With Hypoplastic Aortic ArchDocument7 pagesCurrent Readings On Surgery For The Neonate With Hypoplastic Aortic Archbm1No ratings yet
- Pi Is 0003497500014818Document7 pagesPi Is 0003497500014818GKNo ratings yet
- Valvular Heart DiseaseDocument36 pagesValvular Heart DiseaselaekemariamyismawNo ratings yet
- Coronary Vasomotion AbnormalitiesFrom EverandCoronary Vasomotion AbnormalitiesHiroaki ShimokawaNo ratings yet
- PheochromocytomaDocument74 pagesPheochromocytomamichaelNo ratings yet
- Practical 2 - Health - Assessment - Prac - 2023Document5 pagesPractical 2 - Health - Assessment - Prac - 2023Sreya PNo ratings yet
- Chest Pain, Palpitations, and SyncopeDocument15 pagesChest Pain, Palpitations, and SyncopeRomán Wagner Thomas Esteli ChávezNo ratings yet
- Principles of HaemodynamicsDocument15 pagesPrinciples of HaemodynamicsKELECHI ELEJENo ratings yet
- Jupiter TrialDocument40 pagesJupiter TrialSaad KhanNo ratings yet
- Lab7 Circulatory DisturbancesDocument13 pagesLab7 Circulatory DisturbancesSoon SheedNo ratings yet
- Bureau of Fire Protection First AidDocument7 pagesBureau of Fire Protection First AidRexelle RamosNo ratings yet
- Overview of Cardiovascular DisordersDocument10 pagesOverview of Cardiovascular DisordersPrincewill SeiyefaNo ratings yet
- Handbook of Contrast Echocardiography 1Document47 pagesHandbook of Contrast Echocardiography 1Ghofran i. Hassan NaniNo ratings yet
- Camoeflo-Trac& PiccoDocument15 pagesCamoeflo-Trac& Piccofirdaus che daudNo ratings yet
- PDF Test Bank For Understanding The Essentials of Critical Care Nursing 3Rd Edition Kathleen Perrin Carrie Macleod Online Ebook Full ChapterDocument45 pagesPDF Test Bank For Understanding The Essentials of Critical Care Nursing 3Rd Edition Kathleen Perrin Carrie Macleod Online Ebook Full Chaptertroy.morado744100% (3)
- Cardiovascular Pathology IDocument37 pagesCardiovascular Pathology IOyuka OyukNo ratings yet
- How To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionDocument9 pagesHow To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionnaveenNo ratings yet
- 3636 1 7556 1 10 20230505Document8 pages3636 1 7556 1 10 20230505WellemNo ratings yet
- Fibrion-Tetagam DXMDocument33 pagesFibrion-Tetagam DXMDella Puspita SariNo ratings yet
- 2021 International Consensus On CardiopulmonaryDocument77 pages2021 International Consensus On CardiopulmonaryMateo GómezNo ratings yet
- Nursing Responsibilities After CCDocument5 pagesNursing Responsibilities After CCSofia P. PanlilioNo ratings yet
- The Artificial Heart: A Design Example: BIOE 1000 October 18, 2001Document17 pagesThe Artificial Heart: A Design Example: BIOE 1000 October 18, 2001Paspulati Leelaram100% (1)
- Review Jurnal 2Document10 pagesReview Jurnal 2UlfahNo ratings yet
- 1.1 Scope of ServicesDocument6 pages1.1 Scope of ServicesSwati BajpaiNo ratings yet
- Cardiac Condition NCM 112Document10 pagesCardiac Condition NCM 112Irish Eunice FelixNo ratings yet
- ZUG MMP12 DetailedSpecsBrochureDocument9 pagesZUG MMP12 DetailedSpecsBrochureasokanenNo ratings yet
- 24 Periop Hemodynamic Instability, Consensus, APSFDocument12 pages24 Periop Hemodynamic Instability, Consensus, APSFabsenrifkyjamalNo ratings yet
- The Physiology of Cardiopulmonary Resuscitation (CPR) - ECG & ECHODocument9 pagesThe Physiology of Cardiopulmonary Resuscitation (CPR) - ECG & ECHOUrgencias La RazaNo ratings yet
- Practical Cardiovascular PDFDocument462 pagesPractical Cardiovascular PDFbunawanNo ratings yet
- Assessment of Six Cardiovascular Risk Calculators...Document7 pagesAssessment of Six Cardiovascular Risk Calculators...Ale VillarNo ratings yet
- Pulseless Ventricular Tachycardia/Ventricular Fibrillation Algorithm (Figure 8-5)Document1 pagePulseless Ventricular Tachycardia/Ventricular Fibrillation Algorithm (Figure 8-5)Dyan IslamiNo ratings yet