Download as pptx, pdf, or txt
You might also like
- Comparison Between Api Standard 5L - 45TH & 46TH - Rev. 1Document17 pagesComparison Between Api Standard 5L - 45TH & 46TH - Rev. 1Rushabh Kapadia100% (2)
- OSTEORADIONECROSISDocument38 pagesOSTEORADIONECROSISAbel AbrahamNo ratings yet
- Denture Induced StomatitisDocument15 pagesDenture Induced StomatitisSaroash SadruddinNo ratings yet
- Ulcerative, Vesicular, andDocument117 pagesUlcerative, Vesicular, andvanshikaNo ratings yet
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- Denture Induced StomatitisDocument15 pagesDenture Induced StomatitisSaroash SadruddinNo ratings yet
- DR Meenakshi MDS Oral PathologyDocument29 pagesDR Meenakshi MDS Oral PathologyDr. Meenakshi SinghalNo ratings yet
- Oral Lichen PlanusDocument28 pagesOral Lichen PlanusParul SinghNo ratings yet
- Desquamative GingivitisDocument41 pagesDesquamative Gingivitislucents100% (1)
- Disease of The Oral CavityDocument86 pagesDisease of The Oral CavityAnonymous wqnuimNo ratings yet
- Ranula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandRanula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Dental Management of Diabetic PatientsDocument30 pagesDental Management of Diabetic PatientsChitrang KolawaleNo ratings yet
- 2020 Tongue Disorders Ods 210Document25 pages2020 Tongue Disorders Ods 210Farhaana ShaboodienNo ratings yet
- ErythroplakiaDocument20 pagesErythroplakiaEshan VermaNo ratings yet
- Median Rhomboid GlossitisDocument2 pagesMedian Rhomboid Glossitisdianzalerti9240No ratings yet
- Fungal Infections of The Oral CavityDocument56 pagesFungal Infections of The Oral CavityAkash Anilkumar Malini100% (1)
- Radicular CystDocument45 pagesRadicular CystPriyanka GanesanNo ratings yet
- Herpes Simplex Virus Recurrent Apthous Stomatitis Oral PathoDocument35 pagesHerpes Simplex Virus Recurrent Apthous Stomatitis Oral PathoFourthMolar.comNo ratings yet
- Long Case OSMFDocument17 pagesLong Case OSMFVidhi ParekhNo ratings yet
- Dry Mouth (Xerostomia)Document18 pagesDry Mouth (Xerostomia)dr_jamal1983No ratings yet
- Management of Geriatric PatientsDocument27 pagesManagement of Geriatric PatientsSuraj ShahNo ratings yet
- Vesiculobullous DiseasesDocument48 pagesVesiculobullous DiseasesAprilian PratamaNo ratings yet
- Periodontal Problems in KidsDocument49 pagesPeriodontal Problems in KidsRaksmey PhanNo ratings yet
- Premalignant Conditions of Oral CavityDocument18 pagesPremalignant Conditions of Oral CavityHaneen Masarwa AtamnaNo ratings yet
- Neville's Atlas of Oral Pathology - TEXTODocument488 pagesNeville's Atlas of Oral Pathology - TEXTOgagandeep singh100% (1)
- Ameloblastoma: Submitted byDocument9 pagesAmeloblastoma: Submitted byJana AliNo ratings yet
- Epidemiology of Oral Cancer PDFDocument6 pagesEpidemiology of Oral Cancer PDFمحمد عبدالهادي إسماعيلNo ratings yet
- By:-Surbhi Jaiswal Bds 4 Year. ROLL N0. - 90Document45 pagesBy:-Surbhi Jaiswal Bds 4 Year. ROLL N0. - 90Ranjit BarNo ratings yet
- AIDS and PeriodontiumDocument25 pagesAIDS and PeriodontiumPathivada LumbiniNo ratings yet
- Autoimmune Diseases of The Oral CavityDocument143 pagesAutoimmune Diseases of The Oral CavityMohammed ShaikhNo ratings yet
- Vesiculobullous DiseasesDocument40 pagesVesiculobullous Diseasessgoeldoc_550661200100% (1)
- Dev Disturbances of Gingiva and TongueDocument77 pagesDev Disturbances of Gingiva and TongueNavyy DentNo ratings yet
- Immunologic Diseases of Oral Cavity: - by Saurabh AhujaDocument34 pagesImmunologic Diseases of Oral Cavity: - by Saurabh AhujaSaurabh AhujaNo ratings yet
- Classification System For Oral Submucous FibrosisDocument26 pagesClassification System For Oral Submucous FibrosisDR.YASIR SHAFEEQ MohiyuddinNo ratings yet
- Spread of Oral Infections in Fascial SpacesDocument69 pagesSpread of Oral Infections in Fascial SpacesMoola Bharath Reddy100% (7)
- Dr. Lakshmi Narayana Malabar Cancer CentreDocument81 pagesDr. Lakshmi Narayana Malabar Cancer Centresherani999No ratings yet
- Histopathology of Dental Dental Caries 1Document39 pagesHistopathology of Dental Dental Caries 1Diana SuhartiNo ratings yet
- Cyclic NeutropeniaDocument9 pagesCyclic Neutropeniawafae moutanaNo ratings yet
- XEROSTOMIADocument34 pagesXEROSTOMIAJaya PrabhaNo ratings yet
- Bacterial Infections of Oral CavityDocument63 pagesBacterial Infections of Oral CavityAkash Anilkumar Malini67% (6)
- Investigations in Oral MedicineDocument18 pagesInvestigations in Oral Medicinedr_jamal1983100% (2)
- Oral Cavity PathologyDocument1 pageOral Cavity PathologyJayNo ratings yet
- ThyrotoxicosisDocument42 pagesThyrotoxicosisShaw Khan100% (7)
- Developmental Disturbances of TeethDocument45 pagesDevelopmental Disturbances of TeethAmritha JamesNo ratings yet
- Oral Manifestations of Hematological DisordersDocument6 pagesOral Manifestations of Hematological DisordersPoem AroraNo ratings yet
- Good Morning: by Ibrahim GBRDocument34 pagesGood Morning: by Ibrahim GBRDento - PhilicNo ratings yet
- Developmental Anamolies of Soft Tissues of Oral CavityDocument73 pagesDevelopmental Anamolies of Soft Tissues of Oral Cavityvellingiriramesh53040% (1)
- Diagnosis of Dental CariesDocument35 pagesDiagnosis of Dental CariesKanika MalikNo ratings yet
- Introduction Cysts of JawsDocument62 pagesIntroduction Cysts of JawsEnass Alhadi50% (2)
- AggressiveDocument55 pagesAggressiveSaima KhanNo ratings yet
- Gingival EnlargementDocument74 pagesGingival EnlargementSarita Diwakar100% (2)
- ORAL MANIFESTATIONS OF SYSTEMIC DISEASES Part 1Document97 pagesORAL MANIFESTATIONS OF SYSTEMIC DISEASES Part 1Shreya singhNo ratings yet
- Clinical Features of PeriodontitisDocument36 pagesClinical Features of Periodontitislenami_91No ratings yet
- Sialolithiasis: Vi Ugboko Fmcds FwacsDocument47 pagesSialolithiasis: Vi Ugboko Fmcds FwacsAkeem Alawode50% (2)
- Assoc. Prof. G. Tomov, PHD: Division of Oral Pathology, Faculty of Dental Medicine Mu - PlovdivDocument106 pagesAssoc. Prof. G. Tomov, PHD: Division of Oral Pathology, Faculty of Dental Medicine Mu - PlovdivAustine OsaweNo ratings yet
- Slide 14 Diseases of Salivary Glands IDocument67 pagesSlide 14 Diseases of Salivary Glands IJustDen09No ratings yet
- PHY and CHEM InjuriesDocument58 pagesPHY and CHEM InjuriesDR. H. DIANA J.HENRY CHRISTOPHERNo ratings yet
- Dentine HypersensitivityDocument32 pagesDentine Hypersensitivityitdoc100% (2)
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionFrom EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNo ratings yet
- Lowe Syndrome (Oculocerebrorenal syndrome) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLowe Syndrome (Oculocerebrorenal syndrome) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Contemporary Orthodontic Appliances: PREPARED BY DR - Tahira KulsoomDocument93 pagesContemporary Orthodontic Appliances: PREPARED BY DR - Tahira KulsoomSaroash Sadruddin100% (2)
- Tooth Discoloration (Causes) Internal Bleaching (Indications & Procedures)Document37 pagesTooth Discoloration (Causes) Internal Bleaching (Indications & Procedures)Saroash SadruddinNo ratings yet
- Prostho AssignmentDocument4 pagesProstho AssignmentSaroash SadruddinNo ratings yet
- EZ-212 ManualDocument32 pagesEZ-212 ManualapiadmbrNo ratings yet
- BC 30s (2P)Document2 pagesBC 30s (2P)PT Bintang Baru MedikaNo ratings yet
- My Hell Vol.4 - Janez DrnovšekDocument6 pagesMy Hell Vol.4 - Janez DrnovšekAleksandar JankuloskiNo ratings yet
- At MCQ Salogsacol Auditing Theory Multiple ChoiceDocument32 pagesAt MCQ Salogsacol Auditing Theory Multiple ChoiceJannaviel MirandillaNo ratings yet
- Lesson Plan in Handicraft EmbroideryDocument5 pagesLesson Plan in Handicraft EmbroideryGeraldine Cariño BangugNo ratings yet
- Capr II En6282Document42 pagesCapr II En6282mssonuneNo ratings yet
- Ivory Standalone (PC) User GuideDocument5 pagesIvory Standalone (PC) User GuideToshiro NakagauaNo ratings yet
- BỘ ĐỀ IELTS SPEAKING QUÝ 1-2023Document14 pagesBỘ ĐỀ IELTS SPEAKING QUÝ 1-2023phuongNo ratings yet
- FRP Parameter Optimization Settings: Wilfried Baumgartner / Hans Georg Kloep, SAP July 6, 2016Document36 pagesFRP Parameter Optimization Settings: Wilfried Baumgartner / Hans Georg Kloep, SAP July 6, 2016atungmuNo ratings yet
- Algebra 2005Document40 pagesAlgebra 2005Yb Andik Adi CahyonoNo ratings yet
- Index Properties of SoilDocument27 pagesIndex Properties of Soilahmed yehiaNo ratings yet
- Calcul Ating T He Co ST O F CapitalDocument50 pagesCalcul Ating T He Co ST O F CapitalSyrell NaborNo ratings yet
- Chapter 2-Computer Security Attacks and ThreatsDocument40 pagesChapter 2-Computer Security Attacks and ThreatsYohannes DerejeNo ratings yet
- Windows Server ChecklistDocument116 pagesWindows Server Checklistravichandran_mcpNo ratings yet
- Structure of Nursing KnowledgeDocument18 pagesStructure of Nursing KnowledgeMelany naritoNo ratings yet
- Pensamento Do Design Urbano Contemporâneo - Roggema RobDocument340 pagesPensamento Do Design Urbano Contemporâneo - Roggema RobLuana LuNo ratings yet
- Exam SolutionDocument11 pagesExam SolutionasmaaNo ratings yet
- T40 Series: Technical Data Electronic Hour Meter, DC Hour MeterDocument2 pagesT40 Series: Technical Data Electronic Hour Meter, DC Hour MeterMMM-MMMNo ratings yet
- T650/T650M Treadmill Repair Manual: Sports Art Industrial Co., LTDDocument112 pagesT650/T650M Treadmill Repair Manual: Sports Art Industrial Co., LTDTiago SantosNo ratings yet
- Chapter 8 Supplemental Questions: E8-1 (Inventoriable Costs)Document7 pagesChapter 8 Supplemental Questions: E8-1 (Inventoriable Costs)Dyan NoviaNo ratings yet
- MB0050 - Research MethodologyDocument8 pagesMB0050 - Research MethodologyAnish NairNo ratings yet
- An Assessment of The InternshipDocument1 pageAn Assessment of The InternshipRaj GuruNo ratings yet
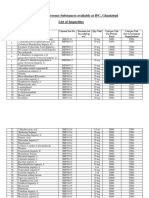
- List of IP Reference Substances Available at IPC, Ghaziabad List of ImpuritiesDocument4 pagesList of IP Reference Substances Available at IPC, Ghaziabad List of ImpuritiesUrva VasavadaNo ratings yet
- Basics of Deep LearningDocument17 pagesBasics of Deep LearningHoor FatimaNo ratings yet
- Marketing Management Course OutlineDocument6 pagesMarketing Management Course OutlineChandrakant VadluruNo ratings yet
- Neuromuscular DisordersDocument3 pagesNeuromuscular Disordersapi-321778954No ratings yet
- Bagga ProfileDocument3 pagesBagga Profileengineeringwatch100% (1)
- Csec Chemistry Notes 7Document2 pagesCsec Chemistry Notes 7debestieNo ratings yet
- Account Name BSB Account Number Account Type Date OpenedDocument6 pagesAccount Name BSB Account Number Account Type Date OpenedAbdul HaseebNo ratings yet