
EBM On Harm - Dentistry 2010
EBM On Harm - Dentistry 2010
You might also like
- Health Education: Evidenced Based PracticesDocument58 pagesHealth Education: Evidenced Based PracticesChantal Raymonds90% (41)
- Epi Exam 2 Q&aDocument13 pagesEpi Exam 2 Q&aeman100% (1)
- EBMDocument636 pagesEBMDaniel SalaNo ratings yet
- EBM On TherapyDocument34 pagesEBM On TherapyRahmah LatifahNo ratings yet
- Evidence-Based Medicine: TherapyDocument40 pagesEvidence-Based Medicine: TherapyJoe HendraNo ratings yet
- Evidence-Based Medicine in Clinical PracticeDocument42 pagesEvidence-Based Medicine in Clinical PracticeNur Rahmah KurniantiNo ratings yet
- Centralization Versus Decentralization ADocument5 pagesCentralization Versus Decentralization AArjit AgarwalNo ratings yet
- EBM Guidleine For CausationDocument15 pagesEBM Guidleine For CausationAYu MiFtakhunNo ratings yet
- Pico ToolDocument7 pagesPico Toolvincentyanuar19No ratings yet
- Critical Appraisal: Prof. Dr. Mohammad Hakimi, Spog (K), PHDDocument37 pagesCritical Appraisal: Prof. Dr. Mohammad Hakimi, Spog (K), PHDFebbty KuswantiNo ratings yet
- Chapter 2 PEY-Measurement of Outcomes - Pharma DostDocument50 pagesChapter 2 PEY-Measurement of Outcomes - Pharma DostKhadeer AG50% (2)
- Evidence Based Medicine!: The Objectives of This Tutorial AreDocument3 pagesEvidence Based Medicine!: The Objectives of This Tutorial AreWildan MentalisNo ratings yet
- Essential Element 1: Quiz Results: Score For This Question Group: 100%Document11 pagesEssential Element 1: Quiz Results: Score For This Question Group: 100%Jaime NaranjoNo ratings yet
- EBM Review: B.BarkerDocument86 pagesEBM Review: B.BarkerdioneeliefmanNo ratings yet
- EBM Worksheets (Therapy, Diagnosis, Prognosis, Economic, Guideline, Decision Making)Document15 pagesEBM Worksheets (Therapy, Diagnosis, Prognosis, Economic, Guideline, Decision Making)Soffatul AzizahNo ratings yet
- Outcome Measure Unit 3Document20 pagesOutcome Measure Unit 3Salini PatelNo ratings yet
- Acceptance and Commitment Therapy in Cancer: Review of Applications and FindingsDocument27 pagesAcceptance and Commitment Therapy in Cancer: Review of Applications and FindingsJuan Alberto GonzálezNo ratings yet
- EBP Presentation by Group 2Document25 pagesEBP Presentation by Group 2Dr-Muhammad QasimNo ratings yet
- Critical Appraisal 2017Document65 pagesCritical Appraisal 2017Fransiscus RivaldyNo ratings yet
- Evidence-Based Medicine MamanDocument79 pagesEvidence-Based Medicine MamanAlma WijayaNo ratings yet
- Declaration of Vienna ArticleDocument6 pagesDeclaration of Vienna ArticleDwi SurantoNo ratings yet
- Clinical Epidemiology - Critical Appraisal of EvidenceDocument49 pagesClinical Epidemiology - Critical Appraisal of EvidenceCristina BosincianuNo ratings yet
- CITATION: Antibiotic Prophylaxis and Recurrent Urinary Tract Infection in ChildrenDocument16 pagesCITATION: Antibiotic Prophylaxis and Recurrent Urinary Tract Infection in Childrenchristian_friztNo ratings yet
- Norcross Evidence-Based Therapy RelationshipsDocument33 pagesNorcross Evidence-Based Therapy Relationshipsttajmuch100% (1)
- Cigarrette Smoking and Lung CancerDocument14 pagesCigarrette Smoking and Lung CancerJaicé AlalunaNo ratings yet
- Pharmaceutical CareDocument22 pagesPharmaceutical CarefikebatuNo ratings yet
- Literature Review Medication Safety in AustraliaDocument5 pagesLiterature Review Medication Safety in Australiaea7gpeqm100% (1)
- CSH600 NotesDocument17 pagesCSH600 NotesSasperilla SummerNo ratings yet
- Research Reflection 3Document6 pagesResearch Reflection 3api-477982644No ratings yet
- Question of Prognosis - Advanced Critical AppraisalDocument2 pagesQuestion of Prognosis - Advanced Critical AppraisalLee ARyNo ratings yet
- Evidence-Based Medicine - UpToDateDocument30 pagesEvidence-Based Medicine - UpToDateSimonNo ratings yet
- Occup Environ Med 2003Document16 pagesOccup Environ Med 2003BM2062119PDPP Pang Kuok WeiNo ratings yet
- Journal Pone 0094207Document7 pagesJournal Pone 0094207JuanaNo ratings yet
- Seligman Consumer Reports StudyDocument16 pagesSeligman Consumer Reports StudyZara KhanNo ratings yet
- Research Final DefenseDocument67 pagesResearch Final DefenseNellyWataNo ratings yet
- Satisfaction Levels With Physical Therapy in Hospitalized PatientsDocument6 pagesSatisfaction Levels With Physical Therapy in Hospitalized PatientscarolciveNo ratings yet
- Saudi Center EBDocument130 pagesSaudi Center EBAnonymous hF5zAdvwCCNo ratings yet
- Menilai Jurnal (CAT)Document53 pagesMenilai Jurnal (CAT)Risya TheupstarNo ratings yet
- Development of The Stanford Expectations of Treatment Scale (SETS) : A Tool For Measuring Patient Outcome Expectancy in Clinical TrialsDocument10 pagesDevelopment of The Stanford Expectations of Treatment Scale (SETS) : A Tool For Measuring Patient Outcome Expectancy in Clinical TrialssoylahijadeunvampiroNo ratings yet
- Other (CD, NR, NA)Document6 pagesOther (CD, NR, NA)Carl JungNo ratings yet
- Approach To Developing GradingDocument8 pagesApproach To Developing GradingSalem RawashdahNo ratings yet
- Patients - Intervention - Comparison - Outcome(s)Document4 pagesPatients - Intervention - Comparison - Outcome(s)sahirbuleNo ratings yet
- A Level Psycology Unit 3 Exam Studies.173697407Document47 pagesA Level Psycology Unit 3 Exam Studies.173697407VF MariaNo ratings yet
- Epidemiology ReviewDocument10 pagesEpidemiology ReviewSaurabhNo ratings yet
- Therapy Worksheet Title of Article: Authors: Journal: BackgroundDocument3 pagesTherapy Worksheet Title of Article: Authors: Journal: BackgroundRandi Kosim SiregarNo ratings yet
- Chapter III - Thesis Breast CancerDocument5 pagesChapter III - Thesis Breast CancerroxannefourteenNo ratings yet
- Impact - Ijranss-1. Ijranss - Length of Stay Reporting in Forensic Secure Care Can Be Augmented by An Overarching Framework To Map Patient Journey in Mentally Disordered Offender Pathway ForDocument38 pagesImpact - Ijranss-1. Ijranss - Length of Stay Reporting in Forensic Secure Care Can Be Augmented by An Overarching Framework To Map Patient Journey in Mentally Disordered Offender Pathway ForImpact JournalsNo ratings yet
- Public Preferences For Prioritizing Preventive and Curative Health Care Interventions - A Discrete Choice ExperimentDocument10 pagesPublic Preferences For Prioritizing Preventive and Curative Health Care Interventions - A Discrete Choice ExperimentTheDevchoudharyNo ratings yet
- Jurnal TubectomyDocument6 pagesJurnal TubectomyAgustin LindaNo ratings yet
- Effects of The Tailored Activity ProgramDocument14 pagesEffects of The Tailored Activity ProgramBarbara Aguilar MaulenNo ratings yet
- 3.1A-Bolton 2007Document10 pages3.1A-Bolton 2007Michael SamaniegoNo ratings yet
- Cross-Sectional Study ExerciseDocument2 pagesCross-Sectional Study ExerciseApril FloresNo ratings yet
- Critical Appraisal of Cohort Studies EBMP 1000e108Document2 pagesCritical Appraisal of Cohort Studies EBMP 1000e108thetaggerung100% (1)
- Critical Appraisal Worksheet - Therapy Evidence (Systematic Review) CitationDocument2 pagesCritical Appraisal Worksheet - Therapy Evidence (Systematic Review) CitationMerlin MariandariNo ratings yet
- Tutorial Epidemiologi 7 (KMPK2016)Document7 pagesTutorial Epidemiologi 7 (KMPK2016)Yudith AnindyaNo ratings yet
- Week 7 AssignmentDocument6 pagesWeek 7 AssignmentJack JungmanNo ratings yet
- Hourly Rounding and The Effects On Patient Safety and Satisfaction ArtifactDocument29 pagesHourly Rounding and The Effects On Patient Safety and Satisfaction Artifactapi-310375757No ratings yet
- Essential Elements Ethics Addressing Relevant QuestionDocument4 pagesEssential Elements Ethics Addressing Relevant QuestionJulius Caesar ColladoNo ratings yet
- The Slim Book of Health Pearls: The Complete Medical ExaminationFrom EverandThe Slim Book of Health Pearls: The Complete Medical ExaminationNo ratings yet
- RONE NCM112BSN3C PhosphorusImbalanceDocument27 pagesRONE NCM112BSN3C PhosphorusImbalanceChezer KiethNo ratings yet
- Case Study 5 Dengue Fever CorrectedDocument13 pagesCase Study 5 Dengue Fever CorrectedyounggirldavidNo ratings yet
- Abstracts From The 6th International Conference On Prevention & Infection Control (ICPIC 2021)Document140 pagesAbstracts From The 6th International Conference On Prevention & Infection Control (ICPIC 2021)Karen RodriguezNo ratings yet
- Schedule of Benefits (Core Silver Without Dental)Document5 pagesSchedule of Benefits (Core Silver Without Dental)Nael SwedanNo ratings yet
- 042 Home Remedies For Common AilmentsDocument230 pages042 Home Remedies For Common AilmentsMunish Chandel75% (4)
- Liver Failure: Lyn CrellinDocument39 pagesLiver Failure: Lyn CrellinTran Ngoc Hoang PhapNo ratings yet
- AFES FINAL Announcement As of 14 SepDocument16 pagesAFES FINAL Announcement As of 14 Sepvanhau24No ratings yet
- Clorazepate Dipotassium (Drug Study)Document2 pagesClorazepate Dipotassium (Drug Study)Franz.thenurse6888No ratings yet
- Medical Spanish II SyllabusDocument3 pagesMedical Spanish II SyllabusTony Lǎo Hǔ ChenNo ratings yet
- Guideline For Medical Internship ProgramDocument41 pagesGuideline For Medical Internship ProgramMufaddal Madraswala50% (2)
- Dip 2Document129 pagesDip 2Raju Teach KapsNo ratings yet
- Congenital Cytomegalovirus Infection Clinical Features and DiagnosisDocument21 pagesCongenital Cytomegalovirus Infection Clinical Features and Diagnosisgomitas21No ratings yet
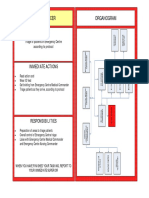
- Triage Officer Organogram: MissionDocument14 pagesTriage Officer Organogram: Missionsnow fazliNo ratings yet
- Gallstone Ileus PDFDocument4 pagesGallstone Ileus PDFmonika100% (1)
- Indwelling CatheterDocument6 pagesIndwelling Cathetereloiza custodioNo ratings yet
- AddisonsDocument2 pagesAddisonsapi-241716715No ratings yet
- Textbook of Plastic, Reconstructive, and Aesthetic SurgeryDocument2 pagesTextbook of Plastic, Reconstructive, and Aesthetic SurgeryEVELYN EZEKWENo ratings yet
- Immunoelectrophoresis (IEP), Serum Protein Electrophoresis (SPE) & Immunofixation (IFX)Document42 pagesImmunoelectrophoresis (IEP), Serum Protein Electrophoresis (SPE) & Immunofixation (IFX)kiedd_04100% (6)
- 1 Prismaflexcrrtintro Seg12007 110326040426 Phpapp02Document38 pages1 Prismaflexcrrtintro Seg12007 110326040426 Phpapp02Sami Maghrebi100% (1)
- Sept 4, 2015Document8 pagesSept 4, 2015Deity CelleNo ratings yet
- History of Pharmaceutical IndustryDocument2 pagesHistory of Pharmaceutical IndustryEswar Gupta Maddi67% (6)
- 10Document28 pages10IndhumathiNo ratings yet
- Max Life Insurance Company LimitedDocument1 pageMax Life Insurance Company LimitedRavindranathNo ratings yet
- Psychiatry Operational Policy PDFDocument124 pagesPsychiatry Operational Policy PDFZaida NorNo ratings yet
- AnaesthesiaDocument5 pagesAnaesthesiaMagesh G Kshathriyan CheyyurNo ratings yet
- Queer Diagnoses RevisitedDocument10 pagesQueer Diagnoses Revisitedsergi pascualNo ratings yet
- Neonatal Intensive Care Unit (NICU) RSUD WangayaDocument5 pagesNeonatal Intensive Care Unit (NICU) RSUD Wangaya201702011 Desy ayu apriliaNo ratings yet
- Esophageal Varices Week 4 T2T3Document37 pagesEsophageal Varices Week 4 T2T3liewhuilianNo ratings yet
- Physical Assessment Kelompok 9Document13 pagesPhysical Assessment Kelompok 9Putri KinantiNo ratings yet
- American Trypanosomiasis: Causative Agent: TrypanosomaDocument32 pagesAmerican Trypanosomiasis: Causative Agent: TrypanosomaMasali MacdonaNo ratings yet
























































































Download as ppt, pdf, or txt
You might also like
- Health Education: Evidenced Based PracticesDocument58 pagesHealth Education: Evidenced Based PracticesChantal Raymonds90% (41)
- Epi Exam 2 Q&aDocument13 pagesEpi Exam 2 Q&aeman100% (1)
- EBMDocument636 pagesEBMDaniel SalaNo ratings yet
- EBM On TherapyDocument34 pagesEBM On TherapyRahmah LatifahNo ratings yet
- Evidence-Based Medicine: TherapyDocument40 pagesEvidence-Based Medicine: TherapyJoe HendraNo ratings yet
- Evidence-Based Medicine in Clinical PracticeDocument42 pagesEvidence-Based Medicine in Clinical PracticeNur Rahmah KurniantiNo ratings yet
- Centralization Versus Decentralization ADocument5 pagesCentralization Versus Decentralization AArjit AgarwalNo ratings yet
- EBM Guidleine For CausationDocument15 pagesEBM Guidleine For CausationAYu MiFtakhunNo ratings yet
- Pico ToolDocument7 pagesPico Toolvincentyanuar19No ratings yet
- Critical Appraisal: Prof. Dr. Mohammad Hakimi, Spog (K), PHDDocument37 pagesCritical Appraisal: Prof. Dr. Mohammad Hakimi, Spog (K), PHDFebbty KuswantiNo ratings yet
- Chapter 2 PEY-Measurement of Outcomes - Pharma DostDocument50 pagesChapter 2 PEY-Measurement of Outcomes - Pharma DostKhadeer AG50% (2)
- Evidence Based Medicine!: The Objectives of This Tutorial AreDocument3 pagesEvidence Based Medicine!: The Objectives of This Tutorial AreWildan MentalisNo ratings yet
- Essential Element 1: Quiz Results: Score For This Question Group: 100%Document11 pagesEssential Element 1: Quiz Results: Score For This Question Group: 100%Jaime NaranjoNo ratings yet
- EBM Review: B.BarkerDocument86 pagesEBM Review: B.BarkerdioneeliefmanNo ratings yet
- EBM Worksheets (Therapy, Diagnosis, Prognosis, Economic, Guideline, Decision Making)Document15 pagesEBM Worksheets (Therapy, Diagnosis, Prognosis, Economic, Guideline, Decision Making)Soffatul AzizahNo ratings yet
- Outcome Measure Unit 3Document20 pagesOutcome Measure Unit 3Salini PatelNo ratings yet
- Acceptance and Commitment Therapy in Cancer: Review of Applications and FindingsDocument27 pagesAcceptance and Commitment Therapy in Cancer: Review of Applications and FindingsJuan Alberto GonzálezNo ratings yet
- EBP Presentation by Group 2Document25 pagesEBP Presentation by Group 2Dr-Muhammad QasimNo ratings yet
- Critical Appraisal 2017Document65 pagesCritical Appraisal 2017Fransiscus RivaldyNo ratings yet
- Evidence-Based Medicine MamanDocument79 pagesEvidence-Based Medicine MamanAlma WijayaNo ratings yet
- Declaration of Vienna ArticleDocument6 pagesDeclaration of Vienna ArticleDwi SurantoNo ratings yet
- Clinical Epidemiology - Critical Appraisal of EvidenceDocument49 pagesClinical Epidemiology - Critical Appraisal of EvidenceCristina BosincianuNo ratings yet
- CITATION: Antibiotic Prophylaxis and Recurrent Urinary Tract Infection in ChildrenDocument16 pagesCITATION: Antibiotic Prophylaxis and Recurrent Urinary Tract Infection in Childrenchristian_friztNo ratings yet
- Norcross Evidence-Based Therapy RelationshipsDocument33 pagesNorcross Evidence-Based Therapy Relationshipsttajmuch100% (1)
- Cigarrette Smoking and Lung CancerDocument14 pagesCigarrette Smoking and Lung CancerJaicé AlalunaNo ratings yet
- Pharmaceutical CareDocument22 pagesPharmaceutical CarefikebatuNo ratings yet
- Literature Review Medication Safety in AustraliaDocument5 pagesLiterature Review Medication Safety in Australiaea7gpeqm100% (1)
- CSH600 NotesDocument17 pagesCSH600 NotesSasperilla SummerNo ratings yet
- Research Reflection 3Document6 pagesResearch Reflection 3api-477982644No ratings yet
- Question of Prognosis - Advanced Critical AppraisalDocument2 pagesQuestion of Prognosis - Advanced Critical AppraisalLee ARyNo ratings yet
- Evidence-Based Medicine - UpToDateDocument30 pagesEvidence-Based Medicine - UpToDateSimonNo ratings yet
- Occup Environ Med 2003Document16 pagesOccup Environ Med 2003BM2062119PDPP Pang Kuok WeiNo ratings yet
- Journal Pone 0094207Document7 pagesJournal Pone 0094207JuanaNo ratings yet
- Seligman Consumer Reports StudyDocument16 pagesSeligman Consumer Reports StudyZara KhanNo ratings yet
- Research Final DefenseDocument67 pagesResearch Final DefenseNellyWataNo ratings yet
- Satisfaction Levels With Physical Therapy in Hospitalized PatientsDocument6 pagesSatisfaction Levels With Physical Therapy in Hospitalized PatientscarolciveNo ratings yet
- Saudi Center EBDocument130 pagesSaudi Center EBAnonymous hF5zAdvwCCNo ratings yet
- Menilai Jurnal (CAT)Document53 pagesMenilai Jurnal (CAT)Risya TheupstarNo ratings yet
- Development of The Stanford Expectations of Treatment Scale (SETS) : A Tool For Measuring Patient Outcome Expectancy in Clinical TrialsDocument10 pagesDevelopment of The Stanford Expectations of Treatment Scale (SETS) : A Tool For Measuring Patient Outcome Expectancy in Clinical TrialssoylahijadeunvampiroNo ratings yet
- Other (CD, NR, NA)Document6 pagesOther (CD, NR, NA)Carl JungNo ratings yet
- Approach To Developing GradingDocument8 pagesApproach To Developing GradingSalem RawashdahNo ratings yet
- Patients - Intervention - Comparison - Outcome(s)Document4 pagesPatients - Intervention - Comparison - Outcome(s)sahirbuleNo ratings yet
- A Level Psycology Unit 3 Exam Studies.173697407Document47 pagesA Level Psycology Unit 3 Exam Studies.173697407VF MariaNo ratings yet
- Epidemiology ReviewDocument10 pagesEpidemiology ReviewSaurabhNo ratings yet
- Therapy Worksheet Title of Article: Authors: Journal: BackgroundDocument3 pagesTherapy Worksheet Title of Article: Authors: Journal: BackgroundRandi Kosim SiregarNo ratings yet
- Chapter III - Thesis Breast CancerDocument5 pagesChapter III - Thesis Breast CancerroxannefourteenNo ratings yet
- Impact - Ijranss-1. Ijranss - Length of Stay Reporting in Forensic Secure Care Can Be Augmented by An Overarching Framework To Map Patient Journey in Mentally Disordered Offender Pathway ForDocument38 pagesImpact - Ijranss-1. Ijranss - Length of Stay Reporting in Forensic Secure Care Can Be Augmented by An Overarching Framework To Map Patient Journey in Mentally Disordered Offender Pathway ForImpact JournalsNo ratings yet
- Public Preferences For Prioritizing Preventive and Curative Health Care Interventions - A Discrete Choice ExperimentDocument10 pagesPublic Preferences For Prioritizing Preventive and Curative Health Care Interventions - A Discrete Choice ExperimentTheDevchoudharyNo ratings yet
- Jurnal TubectomyDocument6 pagesJurnal TubectomyAgustin LindaNo ratings yet
- Effects of The Tailored Activity ProgramDocument14 pagesEffects of The Tailored Activity ProgramBarbara Aguilar MaulenNo ratings yet
- 3.1A-Bolton 2007Document10 pages3.1A-Bolton 2007Michael SamaniegoNo ratings yet
- Cross-Sectional Study ExerciseDocument2 pagesCross-Sectional Study ExerciseApril FloresNo ratings yet
- Critical Appraisal of Cohort Studies EBMP 1000e108Document2 pagesCritical Appraisal of Cohort Studies EBMP 1000e108thetaggerung100% (1)
- Critical Appraisal Worksheet - Therapy Evidence (Systematic Review) CitationDocument2 pagesCritical Appraisal Worksheet - Therapy Evidence (Systematic Review) CitationMerlin MariandariNo ratings yet
- Tutorial Epidemiologi 7 (KMPK2016)Document7 pagesTutorial Epidemiologi 7 (KMPK2016)Yudith AnindyaNo ratings yet
- Week 7 AssignmentDocument6 pagesWeek 7 AssignmentJack JungmanNo ratings yet
- Hourly Rounding and The Effects On Patient Safety and Satisfaction ArtifactDocument29 pagesHourly Rounding and The Effects On Patient Safety and Satisfaction Artifactapi-310375757No ratings yet
- Essential Elements Ethics Addressing Relevant QuestionDocument4 pagesEssential Elements Ethics Addressing Relevant QuestionJulius Caesar ColladoNo ratings yet
- The Slim Book of Health Pearls: The Complete Medical ExaminationFrom EverandThe Slim Book of Health Pearls: The Complete Medical ExaminationNo ratings yet
- RONE NCM112BSN3C PhosphorusImbalanceDocument27 pagesRONE NCM112BSN3C PhosphorusImbalanceChezer KiethNo ratings yet
- Case Study 5 Dengue Fever CorrectedDocument13 pagesCase Study 5 Dengue Fever CorrectedyounggirldavidNo ratings yet
- Abstracts From The 6th International Conference On Prevention & Infection Control (ICPIC 2021)Document140 pagesAbstracts From The 6th International Conference On Prevention & Infection Control (ICPIC 2021)Karen RodriguezNo ratings yet
- Schedule of Benefits (Core Silver Without Dental)Document5 pagesSchedule of Benefits (Core Silver Without Dental)Nael SwedanNo ratings yet
- 042 Home Remedies For Common AilmentsDocument230 pages042 Home Remedies For Common AilmentsMunish Chandel75% (4)
- Liver Failure: Lyn CrellinDocument39 pagesLiver Failure: Lyn CrellinTran Ngoc Hoang PhapNo ratings yet
- AFES FINAL Announcement As of 14 SepDocument16 pagesAFES FINAL Announcement As of 14 Sepvanhau24No ratings yet
- Clorazepate Dipotassium (Drug Study)Document2 pagesClorazepate Dipotassium (Drug Study)Franz.thenurse6888No ratings yet
- Medical Spanish II SyllabusDocument3 pagesMedical Spanish II SyllabusTony Lǎo Hǔ ChenNo ratings yet
- Guideline For Medical Internship ProgramDocument41 pagesGuideline For Medical Internship ProgramMufaddal Madraswala50% (2)
- Dip 2Document129 pagesDip 2Raju Teach KapsNo ratings yet
- Congenital Cytomegalovirus Infection Clinical Features and DiagnosisDocument21 pagesCongenital Cytomegalovirus Infection Clinical Features and Diagnosisgomitas21No ratings yet
- Triage Officer Organogram: MissionDocument14 pagesTriage Officer Organogram: Missionsnow fazliNo ratings yet
- Gallstone Ileus PDFDocument4 pagesGallstone Ileus PDFmonika100% (1)
- Indwelling CatheterDocument6 pagesIndwelling Cathetereloiza custodioNo ratings yet
- AddisonsDocument2 pagesAddisonsapi-241716715No ratings yet
- Textbook of Plastic, Reconstructive, and Aesthetic SurgeryDocument2 pagesTextbook of Plastic, Reconstructive, and Aesthetic SurgeryEVELYN EZEKWENo ratings yet
- Immunoelectrophoresis (IEP), Serum Protein Electrophoresis (SPE) & Immunofixation (IFX)Document42 pagesImmunoelectrophoresis (IEP), Serum Protein Electrophoresis (SPE) & Immunofixation (IFX)kiedd_04100% (6)
- 1 Prismaflexcrrtintro Seg12007 110326040426 Phpapp02Document38 pages1 Prismaflexcrrtintro Seg12007 110326040426 Phpapp02Sami Maghrebi100% (1)
- Sept 4, 2015Document8 pagesSept 4, 2015Deity CelleNo ratings yet
- History of Pharmaceutical IndustryDocument2 pagesHistory of Pharmaceutical IndustryEswar Gupta Maddi67% (6)
- 10Document28 pages10IndhumathiNo ratings yet
- Max Life Insurance Company LimitedDocument1 pageMax Life Insurance Company LimitedRavindranathNo ratings yet
- Psychiatry Operational Policy PDFDocument124 pagesPsychiatry Operational Policy PDFZaida NorNo ratings yet
- AnaesthesiaDocument5 pagesAnaesthesiaMagesh G Kshathriyan CheyyurNo ratings yet
- Queer Diagnoses RevisitedDocument10 pagesQueer Diagnoses Revisitedsergi pascualNo ratings yet
- Neonatal Intensive Care Unit (NICU) RSUD WangayaDocument5 pagesNeonatal Intensive Care Unit (NICU) RSUD Wangaya201702011 Desy ayu apriliaNo ratings yet
- Esophageal Varices Week 4 T2T3Document37 pagesEsophageal Varices Week 4 T2T3liewhuilianNo ratings yet
- Physical Assessment Kelompok 9Document13 pagesPhysical Assessment Kelompok 9Putri KinantiNo ratings yet
- American Trypanosomiasis: Causative Agent: TrypanosomaDocument32 pagesAmerican Trypanosomiasis: Causative Agent: TrypanosomaMasali MacdonaNo ratings yet