Download as ppt, pdf, or txt
You might also like
- Wonka ScriptDocument9 pagesWonka ScriptCarlos Henrique Pinheiro33% (3)
- Marguerite Yourcenar - Oriental TalesDocument160 pagesMarguerite Yourcenar - Oriental TalesErnesto Che100% (3)
- Lesson Plan Types of Speech ActDocument5 pagesLesson Plan Types of Speech ActEDMAR PENUELA57% (7)
- The SepherDocument35 pagesThe SepherRabbi Luis100% (1)
- Growing With The Garden: A Curriculum For Practicing Horticulture With Incarcerated IndividualsDocument179 pagesGrowing With The Garden: A Curriculum For Practicing Horticulture With Incarcerated Individualscalderdavid35No ratings yet
- Oncology 101: Cancer BasicsDocument74 pagesOncology 101: Cancer BasicsMary Rose Jose GragasinNo ratings yet
- Lecture 11-Common Solid TumorsDocument57 pagesLecture 11-Common Solid TumorsAliArabiNo ratings yet
- An Introduction To CancerDocument42 pagesAn Introduction To CancerAmjadRashidNo ratings yet
- L13 OncologyDocument42 pagesL13 OncologyHengkai NeoNo ratings yet
- Cancer EpidemiologyDocument20 pagesCancer EpidemiologyRinothja RajaratnamNo ratings yet
- Uncontrolled Cell Division: CancerDocument35 pagesUncontrolled Cell Division: Cancerkingkola36No ratings yet
- Kanker Growtf Factor Dan Tirosin KinaseDocument142 pagesKanker Growtf Factor Dan Tirosin KinaseNovi KhamiliaNo ratings yet
- Neoplasia Part 7Document44 pagesNeoplasia Part 7Cwali MohamedNo ratings yet
- Kanker For BSMDocument31 pagesKanker For BSMIrni MadyartiNo ratings yet
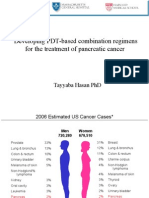
- Developing PDT-based Combination Regimens For The Treatment of Pancreatic CancerDocument33 pagesDeveloping PDT-based Combination Regimens For The Treatment of Pancreatic CancerFirdosh DekhaiyaNo ratings yet
- Kanker GinekologiDocument81 pagesKanker GinekologiSismi AtyNo ratings yet
- Healthy Choices Healthy Living: Talking About CancerDocument15 pagesHealthy Choices Healthy Living: Talking About CancerStarboyNo ratings yet
- Hereditary CancerDocument25 pagesHereditary Cancerlnana3291No ratings yet
- UnderstandingCancer5 15Document48 pagesUnderstandingCancer5 15soon.207193No ratings yet
- Endometrial Cancer An OverviewDocument47 pagesEndometrial Cancer An Overviewachala sahaiNo ratings yet
- IT 27 - Rujukan Pada Doga - EMDocument19 pagesIT 27 - Rujukan Pada Doga - EMRurie Awalia SuhardiNo ratings yet
- Kara CancerDocument45 pagesKara CancerLinux MintNo ratings yet
- Zia 2010Document88 pagesZia 2010Pinanto IrwandyNo ratings yet
- Kanker Pada Perempuan: DR - Hariadi, Spog - K.Onk Rsud Ulin / FK Unlam BanjarmasinDocument68 pagesKanker Pada Perempuan: DR - Hariadi, Spog - K.Onk Rsud Ulin / FK Unlam BanjarmasinNor AinaNo ratings yet
- Collector Oncology 3Document936 pagesCollector Oncology 3Sarhan AliNo ratings yet
- Pathology of Common Cancers 300l Nursing (Abu) 2019Document65 pagesPathology of Common Cancers 300l Nursing (Abu) 2019Hassana YakawuNo ratings yet
- Colorectal Carcinoma DR M.S. RajcoomarDocument19 pagesColorectal Carcinoma DR M.S. RajcoomarKishan NaiduNo ratings yet
- World Cancer DayDocument49 pagesWorld Cancer DayJoydip MitraNo ratings yet
- Ovca 11Document67 pagesOvca 11hop truongvanNo ratings yet
- Benign and Malignant Lesion of Lower GIDocument45 pagesBenign and Malignant Lesion of Lower GIAhmad Alzu3beNo ratings yet
- Breast CancerDocument21 pagesBreast CancerAhmed MansourNo ratings yet
- What Is CancerDocument16 pagesWhat Is CancerLee Teng LinNo ratings yet
- Breast CancerDocument53 pagesBreast Cancersmbala100% (1)
- Kanker Urologi: Budi D Machsoos Div. Hematologi Onkologi Medik Dept. Ilmu Penyakit Dalam FKUB - RSSA MalangDocument32 pagesKanker Urologi: Budi D Machsoos Div. Hematologi Onkologi Medik Dept. Ilmu Penyakit Dalam FKUB - RSSA MalangRakhmiNo ratings yet
- Healthy Choices Healthy Living: Talking About CancerDocument15 pagesHealthy Choices Healthy Living: Talking About CancerMila MarkovskaNo ratings yet
- Colorectal Carcinoma: Colorectal Carcinoma (CRC) Is The Most Common Cancer of The Gastrointestinal Tract and TheDocument14 pagesColorectal Carcinoma: Colorectal Carcinoma (CRC) Is The Most Common Cancer of The Gastrointestinal Tract and TheYTNo ratings yet
- Ovarian Cancer: Vaishvi AgrawalDocument28 pagesOvarian Cancer: Vaishvi AgrawalVaishvi Agrawal RA1711014010084No ratings yet
- Early Detection Ovarian Cancer - gps2010 DR YudiDocument36 pagesEarly Detection Ovarian Cancer - gps2010 DR YudiRanni Fistri KhaisariNo ratings yet
- - - 640 - TM - ovcystsld (2) - نسخةDocument12 pages- - 640 - TM - ovcystsld (2) - نسخةHaider Nadhem AL-rubaiNo ratings yet
- Breast Cancer - PPTX 2013Document49 pagesBreast Cancer - PPTX 2013heba1997bshNo ratings yet
- Breast Cancer FinalDocument22 pagesBreast Cancer FinalSalman KhanNo ratings yet
- Pancreatic Cancer: by Moaz MehboobDocument18 pagesPancreatic Cancer: by Moaz MehboobMUHAMMAD HAMZA IRSHADNo ratings yet
- Epdiomology of CancerDocument19 pagesEpdiomology of CancerAyoub ZeinEddinNo ratings yet
- Cervical CancerDocument15 pagesCervical CancerMahen BoralessaNo ratings yet
- Cervical Cancer: By: Patricia MontoyaDocument15 pagesCervical Cancer: By: Patricia MontoyaSuci Rahayu EvashaNo ratings yet
- COLORECTAL CANCER FINAL PPT To Be PresentedDocument53 pagesCOLORECTAL CANCER FINAL PPT To Be Presentedamanuel100% (1)
- Introduction To Cancer GeneticsDocument16 pagesIntroduction To Cancer GeneticsYashraj SinghNo ratings yet
- Pancreatic TumorDocument89 pagesPancreatic Tumorrevathyrjndrn5No ratings yet
- Breast Cancer: by Eric Lee & Rikki HabernyDocument53 pagesBreast Cancer: by Eric Lee & Rikki HabernyNurul Ilmi UtamiNo ratings yet
- Breast CancerDocument7 pagesBreast CancerDeepankar Srigyan100% (1)
- Breast Cancer Screening and Early Detection: Dr. Mohammed Tarawneh Consultant Family PhysicianDocument69 pagesBreast Cancer Screening and Early Detection: Dr. Mohammed Tarawneh Consultant Family PhysicianDr-Firas Nayf Al-ThawabiaNo ratings yet
- Sainik School Kalikiri: Investigatory Project On "Cancer"Document17 pagesSainik School Kalikiri: Investigatory Project On "Cancer"C TejuNo ratings yet
- BreastCancer - Erasmus 2020Document53 pagesBreastCancer - Erasmus 2020Anonymous dKiLqVS3L5No ratings yet
- Cancer NursingDocument53 pagesCancer Nursingfairwoods100% (1)
- © 2010 Mcgraw-Hill Companies. All Rights ReservedDocument36 pages© 2010 Mcgraw-Hill Companies. All Rights ReservedThalia SandersNo ratings yet
- Malignant Ovarian TumourDocument42 pagesMalignant Ovarian TumourJones MarinaNo ratings yet
- Breast Cancer: Katherine Macgillivray & Melissa PoirierDocument62 pagesBreast Cancer: Katherine Macgillivray & Melissa PoirierJonathan Darell WijayaNo ratings yet
- Surgery 2 Revision Breast & Acute PancreatitisDocument50 pagesSurgery 2 Revision Breast & Acute PancreatitisAnass SaleemNo ratings yet
- Ovarian CancerDocument8 pagesOvarian Cancerthabetamal63No ratings yet
- Cervical Cancer Church PresentationDocument48 pagesCervical Cancer Church Presentationbande_adegboyegaNo ratings yet
- 17 Educating Youth Presentation 1Document15 pages17 Educating Youth Presentation 1genellemaarteNo ratings yet
- Endometrial NeoplasiaDocument48 pagesEndometrial NeoplasiaBONI M.WoyessaNo ratings yet
- Types of Ovarian CancerDocument5 pagesTypes of Ovarian Cancerوسام وميض عبدالله CNo ratings yet
- 1203.staying Full of GodDocument5 pages1203.staying Full of GodnigelNo ratings yet
- King Charles IDocument349 pagesKing Charles Ipatel_musicmsncomNo ratings yet
- ASAStyle Guide PrintoutDocument8 pagesASAStyle Guide PrintoutAnsyf10No ratings yet
- Brand Management: Assignment - 2Document8 pagesBrand Management: Assignment - 2POOJA AGARWAL BMS2019No ratings yet
- Differences Between British and American EnglishDocument6 pagesDifferences Between British and American EnglishDana Barwal100% (1)
- Theoretical Modelling of Ultrasonic Non-Destructive TestingDocument5 pagesTheoretical Modelling of Ultrasonic Non-Destructive TestingAmir JoonNo ratings yet
- Love & Sex AddictionsDocument50 pagesLove & Sex AddictionsJordan Strawser100% (4)
- RD100 Party Pack AmericanDocument20 pagesRD100 Party Pack AmericanHari Bathula100% (1)
- Purposive Communication Unit 1 Chapter 5Document23 pagesPurposive Communication Unit 1 Chapter 5Fiolia Erlle Bela-ong EspinozaNo ratings yet
- Partnership REPORTDocument4 pagesPartnership REPORTAiza A. CayananNo ratings yet
- 10 - Đề Thi Tham Khảo Ts10 - 2020Document4 pages10 - Đề Thi Tham Khảo Ts10 - 2020Duyen MyNo ratings yet
- Historical ReviewDocument2 pagesHistorical ReviewKimber Lee BaldozNo ratings yet
- Manila Pavilion v. DeladaDocument2 pagesManila Pavilion v. Deladasitsee watchNo ratings yet
- Key Aspects of Paycheck Protection Program (PPP) Loan DataDocument2 pagesKey Aspects of Paycheck Protection Program (PPP) Loan DataJennifer WeaverNo ratings yet
- A Coptic Narrative in Egypt A Biography of The Boutros Ghali Family (Youssef Boutros Ghali (Editor) ) (Z-Library)Document256 pagesA Coptic Narrative in Egypt A Biography of The Boutros Ghali Family (Youssef Boutros Ghali (Editor) ) (Z-Library)Ibrahim AmadouNo ratings yet
- Tulpa's DIY Guide To Tulpamancy v4Document193 pagesTulpa's DIY Guide To Tulpamancy v4wylder100% (1)
- Self Made Managerial EconomicsDocument14 pagesSelf Made Managerial EconomicsSameel Ur RehmanNo ratings yet
- Literary Criticism - 21st CDocument2 pagesLiterary Criticism - 21st CGabrielle mari BulawanNo ratings yet
- Copy of Famous Educator Infographic Template ExampleDocument1 pageCopy of Famous Educator Infographic Template Exampleapi-643989450No ratings yet
- Beamex MC6 Multifunction Calibrator NATA CertifiedDocument28 pagesBeamex MC6 Multifunction Calibrator NATA CertifiedEliyanto E BudiartoNo ratings yet
- Heikin Ashi - BegginerDocument11 pagesHeikin Ashi - BegginerEko Aji WahyudinNo ratings yet
- Sample Test Hkimo Grade 3 (Vòng Sơ Lo I) : Part I: Logical ThinkingDocument7 pagesSample Test Hkimo Grade 3 (Vòng Sơ Lo I) : Part I: Logical ThinkingThu Thủy NguyễnNo ratings yet
- Windows 10 - The Beginner's Guid - Matthew Sanderson PDFDocument46 pagesWindows 10 - The Beginner's Guid - Matthew Sanderson PDFmichelleNo ratings yet
- p1 SummativeDocument3 pagesp1 Summativeapi-346594405No ratings yet
- Physics SeaDocument464 pagesPhysics SeaMaheshwar Kumar100% (1)