Download as pptx, pdf, or txt
You might also like
- Patient Counseling PresentationDocument30 pagesPatient Counseling PresentationBaguma Michael100% (1)
- Hematology Report:: Lahore: 07 Jail Road, Main Gulberg - Karachi: Al Khaleej Plaza, Shaheed-e-Millat RoadDocument2 pagesHematology Report:: Lahore: 07 Jail Road, Main Gulberg - Karachi: Al Khaleej Plaza, Shaheed-e-Millat RoadUmer FarooqNo ratings yet
- Dzinos MedicineDocument455 pagesDzinos MedicineCollen Lihaka100% (2)
- Communication Skills in MedicineDocument50 pagesCommunication Skills in Medicineicasan1289No ratings yet
- Try To Make Paraphrase Sentences No Original Sentence Paraphrase SentenceDocument3 pagesTry To Make Paraphrase Sentences No Original Sentence Paraphrase SentenceBrenda VenittaNo ratings yet
- Introduction To Clinical Techniques and Basic Life Support: DR Justine Jelagat Odionyi Consultant PaediatricianDocument31 pagesIntroduction To Clinical Techniques and Basic Life Support: DR Justine Jelagat Odionyi Consultant PaediatricianMalueth AnguiNo ratings yet
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- Adult Physical AssessmentDocument18 pagesAdult Physical AssessmentHa HahahahahaNo ratings yet
- PHB Lec 1 Phlebotomy and The Health Care Setting Part 1Document42 pagesPHB Lec 1 Phlebotomy and The Health Care Setting Part 1Jean KenNo ratings yet
- Clnical MedicineDocument42 pagesClnical Medicineahmed mokhtarNo ratings yet
- Interviewing and Respiratory HistoryDocument36 pagesInterviewing and Respiratory HistoryDharlyn MungcalNo ratings yet
- Interview Skills & HistoryDocument28 pagesInterview Skills & HistoryAsad MirajNo ratings yet
- Foundations of Clinical Medicine-1 Summer 2014 Semester: History TakingDocument63 pagesFoundations of Clinical Medicine-1 Summer 2014 Semester: History Takingparanoea911100% (1)
- K1 (Anamnesis & Pemeriksaan Fisis)Document42 pagesK1 (Anamnesis & Pemeriksaan Fisis)Esther Meyline XhypaNo ratings yet
- R. Gundo Medical/Surgical Nursing Department: History TakingDocument39 pagesR. Gundo Medical/Surgical Nursing Department: History Takingchifunndo charlesNo ratings yet
- Pom MidtermsDocument692 pagesPom MidtermsGwyneth MendozaNo ratings yet
- Propaedeutics of intеrnаl medicine as аn introduction to the clinic of internal medicine. Questioning and physical examination of the patient. Еthical and deontological aspectsDocument42 pagesPropaedeutics of intеrnаl medicine as аn introduction to the clinic of internal medicine. Questioning and physical examination of the patient. Еthical and deontological aspectsDonia HnainiaNo ratings yet
- Health HistoryDocument8 pagesHealth HistoryAhmed MohamedNo ratings yet
- Code of EthicsDocument10 pagesCode of Ethicsviswa chowdaryNo ratings yet
- History TakingDocument51 pagesHistory TakingJAMES TONNY OKINYINo ratings yet
- History TakingDocument51 pagesHistory TakingJAMES TONNY OKINYINo ratings yet
- Taking The Medical HistoryDocument2 pagesTaking The Medical HistoryPaf VenancioNo ratings yet
- History Taking2Document25 pagesHistory Taking2Capture UnseenNo ratings yet
- PAL Pack 2011 KI UpdateDocument41 pagesPAL Pack 2011 KI UpdateLuveon TangNo ratings yet
- Examination QuestionsDocument54 pagesExamination Questionspetertapiwamuchemwa6No ratings yet
- History Taking Physical ExamininationDocument41 pagesHistory Taking Physical ExamininationAya AmerNo ratings yet
- Asesment Conditional 06Document8 pagesAsesment Conditional 06Abdul WakhidNo ratings yet
- Definition (Tugas Terjemahan) Konsep Berpikir KritisDocument12 pagesDefinition (Tugas Terjemahan) Konsep Berpikir KritisNadira ThyoNo ratings yet
- Clinical Assessment of Older PeopleDocument72 pagesClinical Assessment of Older PeopleMimo HemadNo ratings yet
- Chapter One Introduction To Clinical MedicineDocument23 pagesChapter One Introduction To Clinical MedicinemulaewolloNo ratings yet
- Health HistoryDocument45 pagesHealth HistoryCatlyn Chatpman100% (1)
- Week 3 - Subjective DataDocument29 pagesWeek 3 - Subjective DataGLADYS MAY GUDELOS MEJIASNo ratings yet
- History TakingDocument4 pagesHistory Takingabdulmarwat88No ratings yet
- Introduction To History Taking Aims:: Summary of Procedure and NotesDocument6 pagesIntroduction To History Taking Aims:: Summary of Procedure and Notesmj.vinoth@gmail.comNo ratings yet
- Nursing Associate Mock ScenarioDocument14 pagesNursing Associate Mock ScenarioShobhaNo ratings yet
- Interviewing and The Health HistoryDocument18 pagesInterviewing and The Health HistoryWendz BouvierNo ratings yet
- Prof. Maria Susan Z. MaglaquiDocument24 pagesProf. Maria Susan Z. MaglaquiSusan MaglaquiNo ratings yet
- Venipuncture 2019Document88 pagesVenipuncture 2019alyszafranzinedhyNo ratings yet
- Patient SafetyDocument30 pagesPatient Safetyariffk10No ratings yet
- Card Adverse EventsDocument4 pagesCard Adverse EventsDanonino12No ratings yet
- 5-1 HX & Exam Handbook Final PDFDocument23 pages5-1 HX & Exam Handbook Final PDFPépé TechopathamNo ratings yet
- 2023 Introduction To Physical DiagnosisDocument37 pages2023 Introduction To Physical DiagnosisNejibMohe Abagisa100% (1)
- Chapter 2 D-P CommunicationDocument30 pagesChapter 2 D-P CommunicationEINSTEIN2DNo ratings yet
- Course Guide: Year 3Document52 pagesCourse Guide: Year 3Elise ChuaNo ratings yet
- Patient History: Objectives Building RapportDocument15 pagesPatient History: Objectives Building RapportAnonymous 23ghm1No ratings yet
- By: Kris Lyn L. TejereoDocument30 pagesBy: Kris Lyn L. TejereoKris TejereroNo ratings yet
- Counselling, Breaking Bad NewsDocument26 pagesCounselling, Breaking Bad NewsArief NorddinNo ratings yet
- Health Assessment of The Patient ParagraphdDocument23 pagesHealth Assessment of The Patient ParagraphdAmos TalsandekarNo ratings yet
- Asthma Nursing Care Plans - LippincottDocument45 pagesAsthma Nursing Care Plans - LippincottDyllanoNo ratings yet
- AVYKDocument6 pagesAVYKMinh Thành Trí LêNo ratings yet
- Comunicação Utentes Com MedoDocument4 pagesComunicação Utentes Com MedoMafaldaPereira184No ratings yet
- Practical Empathy Ethics CommunicationDocument9 pagesPractical Empathy Ethics CommunicationArshdeep NainNo ratings yet
- NP1 Study NotesDocument8 pagesNP1 Study NotesTijanne-Jayde CunialNo ratings yet
- Learn About The Key Requirements, Duties, Responsibilities, and Skills That Should Be in A Doctor Job DescriptionDocument3 pagesLearn About The Key Requirements, Duties, Responsibilities, and Skills That Should Be in A Doctor Job Descriptioncannon unisexNo ratings yet
- A Textbook of Clinical Pharmacy Practice Essential Concepts and Skills by G ParthasarathiDocument26 pagesA Textbook of Clinical Pharmacy Practice Essential Concepts and Skills by G ParthasarathiAman UpadhyayNo ratings yet
- Patient Assessment: by Grace MwanikiDocument48 pagesPatient Assessment: by Grace MwanikiPatience WaithiraNo ratings yet
- Care Study Made Simple by NMC-GHDocument19 pagesCare Study Made Simple by NMC-GHametepeprince1No ratings yet
- Clinical History TakingDocument36 pagesClinical History Takingapi-1964133775% (4)
- History3 LungooooooDocument10 pagesHistory3 LungooooooGiorgio CivitareseNo ratings yet
- History Taking by Dr. Ayman ShaltootDocument9 pagesHistory Taking by Dr. Ayman ShaltootALI ALFARDANNo ratings yet
- Savio Case Presentation Format 2024Document156 pagesSavio Case Presentation Format 2024Jeamine Talaver PalenciaNo ratings yet
- Protease Inhibitors (Pi) : Anyika CelpherDocument22 pagesProtease Inhibitors (Pi) : Anyika CelpherMalueth AnguiNo ratings yet
- Other Anti-HivDocument24 pagesOther Anti-HivMalueth AnguiNo ratings yet
- Nnrtis: Nonnucleoside Reverse Trancriptase InhibitorsDocument12 pagesNnrtis: Nonnucleoside Reverse Trancriptase InhibitorsMalueth AnguiNo ratings yet
- Hiv HaartDocument12 pagesHiv HaartMalueth AnguiNo ratings yet
- Antiretroviral Therapy: Dr. Samuel Mwaniki (Bpharm., MSC Tid, Uon)Document22 pagesAntiretroviral Therapy: Dr. Samuel Mwaniki (Bpharm., MSC Tid, Uon)Malueth AnguiNo ratings yet
- Med II Antihelminthics and Antiprotozoal Agents 2008Document31 pagesMed II Antihelminthics and Antiprotozoal Agents 2008Malueth AnguiNo ratings yet
- Antifungal DrugsDocument66 pagesAntifungal DrugsMalueth AnguiNo ratings yet
- 2 LOCAL ANAESTHETICS EgertonDocument24 pages2 LOCAL ANAESTHETICS EgertonMalueth AnguiNo ratings yet
- Antimalarial DrugsDocument49 pagesAntimalarial DrugsMalueth Angui50% (2)
- Antiviral DrugsDocument13 pagesAntiviral DrugsMalueth AnguiNo ratings yet
- Head & Neck TumoursDocument15 pagesHead & Neck TumoursMalueth AnguiNo ratings yet
- Antituberculous DrugDocument29 pagesAntituberculous DrugMalueth AnguiNo ratings yet
- Human Immunodeficiency VirusDocument24 pagesHuman Immunodeficiency VirusMalueth AnguiNo ratings yet
- Prostate CancerDocument67 pagesProstate CancerMalueth AnguiNo ratings yet
- Antiviral TherapyDocument19 pagesAntiviral TherapyMalueth AnguiNo ratings yet
- K 17 Colorectal CarcinomaDocument63 pagesK 17 Colorectal CarcinomaMalueth AnguiNo ratings yet
- Antiretroviral Therapy: Pharmacology: Cristina Gruta, PharmdDocument47 pagesAntiretroviral Therapy: Pharmacology: Cristina Gruta, PharmdMalueth AnguiNo ratings yet
- Chemotherapy: Chemotherapy, in Its Most General Sense, Refers To Treatment of Disease byDocument42 pagesChemotherapy: Chemotherapy, in Its Most General Sense, Refers To Treatment of Disease byMalueth AnguiNo ratings yet
- Hepatocellular CarcinomaDocument10 pagesHepatocellular CarcinomaMalueth AnguiNo ratings yet
- Targeted Therapy: Specific Targeted Molecules Needed For Carcinogenesis and Tumor GrowthDocument9 pagesTargeted Therapy: Specific Targeted Molecules Needed For Carcinogenesis and Tumor GrowthMalueth AnguiNo ratings yet
- Adrenal DisordersDocument36 pagesAdrenal DisordersMalueth AnguiNo ratings yet
- 2 INTRAVENOUS ANESTHESIA EgertonDocument21 pages2 INTRAVENOUS ANESTHESIA EgertonMalueth AnguiNo ratings yet
- Ambiguous Genitalia (Disorders of Sexual Differentiation) : DR GwerDocument18 pagesAmbiguous Genitalia (Disorders of Sexual Differentiation) : DR GwerMalueth AnguiNo ratings yet
- Child Abuse and NeglectDocument25 pagesChild Abuse and NeglectMalueth Angui100% (1)
- Immunization:: DR Wamalwa DDocument45 pagesImmunization:: DR Wamalwa DMalueth Angui0% (1)
- Hypoparathyroidism: DR GwerDocument14 pagesHypoparathyroidism: DR GwerMalueth AnguiNo ratings yet
- Cytogenetics PresentationDocument11 pagesCytogenetics PresentationMalueth AnguiNo ratings yet
- ABDOMINAL AND PELVIC MASSES IN PEDIATRICS - Level 4Document26 pagesABDOMINAL AND PELVIC MASSES IN PEDIATRICS - Level 4Malueth AnguiNo ratings yet
- Constitutional Growth DelayDocument23 pagesConstitutional Growth DelayMalueth AnguiNo ratings yet
- Child Abuse & Neglect: MBCHB Iv 2006Document24 pagesChild Abuse & Neglect: MBCHB Iv 2006Malueth AnguiNo ratings yet
- NCH EndorsementsDocument7 pagesNCH EndorsementsAisa AusanNo ratings yet
- Vasavi - Charaka Case PresentationDocument50 pagesVasavi - Charaka Case PresentationHemanthKumarNo ratings yet
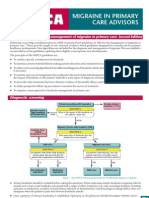
- National Guidelines - MigraineDocument4 pagesNational Guidelines - MigraineSean CardozoNo ratings yet
- EntireDrugPack - BFN FINAL 090217 PDFDocument134 pagesEntireDrugPack - BFN FINAL 090217 PDFDeny HudaNo ratings yet
- HLS19 Q12 NO - English (10116)Document1 pageHLS19 Q12 NO - English (10116)陳順玲No ratings yet
- Psychotherapy For BPDDocument5 pagesPsychotherapy For BPDJuanaNo ratings yet
- Common Guidelines For Diagnostic Approaches To Leukemias PDFDocument35 pagesCommon Guidelines For Diagnostic Approaches To Leukemias PDFNarendraswari Mendina KusumawardhaniNo ratings yet
- Trans - Research - Overview of Evidence Based MedicineDocument2 pagesTrans - Research - Overview of Evidence Based MedicinegailNo ratings yet
- 2011 Veterinary Vaccinesand Their Importanceto Animal Healthand Public HealthDocument11 pages2011 Veterinary Vaccinesand Their Importanceto Animal Healthand Public HealthCARLOTA DIAZ AGUILARNo ratings yet
- Daftar Barang Mau ED Bulan Maret - Agustus Tahun 2021Document29 pagesDaftar Barang Mau ED Bulan Maret - Agustus Tahun 2021fiannysjahjadiNo ratings yet
- PEP20 02 01 004 - Final - 508Document346 pagesPEP20 02 01 004 - Final - 508Amel EzNo ratings yet
- Free Practice Questions & Answers For The Pharmacology ExamDocument3 pagesFree Practice Questions & Answers For The Pharmacology ExamDalbir SinghNo ratings yet
- The Treatment and Management of Selfharm in Emergency Departments Slide Set Powerpoint 189897661Document41 pagesThe Treatment and Management of Selfharm in Emergency Departments Slide Set Powerpoint 189897661Zorbey TurkalpNo ratings yet
- Module 1-INTRO TO OSH-SO1Document12 pagesModule 1-INTRO TO OSH-SO1RocsNo ratings yet
- NCP FormatDocument9 pagesNCP FormatNiña AngNo ratings yet
- Pediatrics-in-Review 1989 - Acute Diarrhea in Children PDFDocument10 pagesPediatrics-in-Review 1989 - Acute Diarrhea in Children PDFmob3No ratings yet
- The Use of Warfarin in Prosthetic Heart Valves Patient Short VersionDocument27 pagesThe Use of Warfarin in Prosthetic Heart Valves Patient Short VersionStanley Santosa KamadjajaNo ratings yet
- Managing The Difficult Soft Tissue Envelope in Facial and Rhinoplasty SurgeryDocument15 pagesManaging The Difficult Soft Tissue Envelope in Facial and Rhinoplasty SurgeryFabian Camelo OtorrinoNo ratings yet
- DGCA Human Performance & LimitationsDocument6 pagesDGCA Human Performance & Limitationsabdur rahim100% (1)
- Question Paper Ms ObgDocument2 pagesQuestion Paper Ms ObgAliyaNo ratings yet
- A Comparative Clinical Study ofDocument11 pagesA Comparative Clinical Study ofArter AdamNo ratings yet
- Is Sammy AliveDocument2 pagesIs Sammy Aliveapi-342334216No ratings yet
- Electrocardiograph Y (ECG / Ekg) : Rose Dyane F - Nunag, RMT, MPHDocument52 pagesElectrocardiograph Y (ECG / Ekg) : Rose Dyane F - Nunag, RMT, MPHClaire GonoNo ratings yet
- Causes and Treatment of AddictionDocument21 pagesCauses and Treatment of AddictionNizam100% (1)
- Smoking ScriptDocument3 pagesSmoking ScriptNorjetalexis Maningo CabreraNo ratings yet
- IV Med Notes v1Document181 pagesIV Med Notes v1Joan Manabat BugnaNo ratings yet
- Heart Failure Clinical Pathway TemplateDocument3 pagesHeart Failure Clinical Pathway Templategusmarinda fauziahNo ratings yet
- Hot Stone Massage BenefitsjhxnjDocument2 pagesHot Stone Massage Benefitsjhxnjsecondstove31No ratings yet