
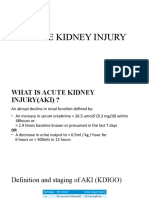
Acute Kidney Injury: DR B Parag Department of Nephrology
Acute Kidney Injury: DR B Parag Department of Nephrology
You might also like
- Chapter 15-Basics of Electrical Systems: True/FalseDocument190 pagesChapter 15-Basics of Electrical Systems: True/FalsewesamNo ratings yet
- Acute Renal FailureDocument33 pagesAcute Renal FailureAqsa Akbar AliNo ratings yet
- Acute Renal Failure - PPT 1Document36 pagesAcute Renal Failure - PPT 1Jay Paul100% (1)
- Renal Acute Kidney InjuryDocument41 pagesRenal Acute Kidney InjuryTim SilvaNo ratings yet
- Noel A. Villanueva, MD, FPCP, FPSNDocument62 pagesNoel A. Villanueva, MD, FPCP, FPSNagilNo ratings yet
- Acute Renal Failure Lecture 1 Critical Care Nursing NewDocument41 pagesAcute Renal Failure Lecture 1 Critical Care Nursing NewEdwin Jose SNo ratings yet
- Nephrology & Urology: Archer Online USMLE ReviewsDocument107 pagesNephrology & Urology: Archer Online USMLE ReviewsBeerappaJanpetNo ratings yet
- Management of Acute Kidney InjuryDocument31 pagesManagement of Acute Kidney InjurysumitNo ratings yet
- AkiDocument38 pagesAkiPhillip MartinezNo ratings yet
- Alternative NamesDocument67 pagesAlternative NamespashaNo ratings yet
- Acute Kidney InjuryDocument60 pagesAcute Kidney InjuryAbegail Fermanejo-GeneraoNo ratings yet
- 22.AKI ProtocolDocument2 pages22.AKI ProtocolRed DevilNo ratings yet
- Acute Renal Failure Lecture 1 Critical Care NursingDocument52 pagesAcute Renal Failure Lecture 1 Critical Care NursingDina Rasmita100% (2)
- Acute Renal FailureDocument10 pagesAcute Renal FailureSypheruNo ratings yet
- Acute Renal FailureDocument28 pagesAcute Renal FailureAs SyarifNo ratings yet
- Acute Kidney Injury: DR Hodan Ahmed Dept of Pediatrics and Child Health Amoud Medical School, AUDocument32 pagesAcute Kidney Injury: DR Hodan Ahmed Dept of Pediatrics and Child Health Amoud Medical School, AUMohamoud MohamedNo ratings yet
- Caz Clinic - IRADocument35 pagesCaz Clinic - IRAIonela Roberta100% (1)
- AkiDocument42 pagesAkimarauder_popNo ratings yet
- Acute Renal FailureDocument31 pagesAcute Renal FailureODONG MARTINNo ratings yet
- Dr. Tjatur Winarsanto SPPDDocument37 pagesDr. Tjatur Winarsanto SPPDEndah Risky GustiyantiNo ratings yet
- Acute Kidney Injury (AKI) : by Prof Grace Irimu Consultant Pediatrician and NephrologistDocument43 pagesAcute Kidney Injury (AKI) : by Prof Grace Irimu Consultant Pediatrician and Nephrologistokwadha simionNo ratings yet
- Approach To Acute Renal FailureDocument40 pagesApproach To Acute Renal FailureMochammad Fariz AmsalNo ratings yet
- Acute Renal Failure BDocument60 pagesAcute Renal Failure BEzekiel moraraNo ratings yet
- DR Ankit Soni DNB Trainee (Peds)Document28 pagesDR Ankit Soni DNB Trainee (Peds)Ankit SoniNo ratings yet
- Acute and Chronic Renal Failure MyDocument45 pagesAcute and Chronic Renal Failure MyJoseph Krafft100% (3)
- Acute Renal FailureDocument33 pagesAcute Renal Failureimranqazi11No ratings yet
- Cirrhosis of LiverDocument106 pagesCirrhosis of LiveraahadNo ratings yet
- Acute Kidney InjuryDocument23 pagesAcute Kidney InjuryBaraka SayoreNo ratings yet
- Nursing Management of AKIDocument24 pagesNursing Management of AKIheenamaharjanNo ratings yet
- Acute& Chronic Kidney DiseaseDocument91 pagesAcute& Chronic Kidney DiseaseSonia YadavNo ratings yet
- Manajemen Anestesi Pada Uremic SyndromeDocument27 pagesManajemen Anestesi Pada Uremic SyndromeAdi Nugroho MelyanaNo ratings yet
- Renal FailureDocument23 pagesRenal FailurerjfeeleyNo ratings yet
- Renal Faliure 1Document50 pagesRenal Faliure 1180045No ratings yet
- Acute Kidney InjuryDocument3 pagesAcute Kidney InjuryHarkirat AtwalNo ratings yet
- Acute Renal FailureDocument75 pagesAcute Renal FailureAshwin Raghav SankarNo ratings yet
- Renal Calculi & Renal FailureDocument17 pagesRenal Calculi & Renal Failureazlan100% (1)
- Kidney: Disorders of TheDocument52 pagesKidney: Disorders of ThejuliusromatolentinoNo ratings yet
- Acute Renal Failure: DR Grania PriceDocument24 pagesAcute Renal Failure: DR Grania PriceCastro KisuuleNo ratings yet
- Acute Renal Failure: Dr. Sami Abdo RadmanDocument23 pagesAcute Renal Failure: Dr. Sami Abdo RadmanAdeniran CharlesNo ratings yet
- Aki - CKDDocument51 pagesAki - CKDAyu Luh Ratri WeningNo ratings yet
- Acute Renal FailureDocument10 pagesAcute Renal FailureAlia PutriNo ratings yet
- Acute Kidney Injury: Syakib BakriDocument46 pagesAcute Kidney Injury: Syakib BakriBhisma D. SyaputraNo ratings yet
- Acute Kidney InjuryDocument40 pagesAcute Kidney InjuryNabin SimkhadaNo ratings yet
- Final AKI For IM 2014Document45 pagesFinal AKI For IM 2014Andika Yusuf RamadhanNo ratings yet
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisDocument35 pagesLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanNo ratings yet
- Chronic Renal Failure 4-9-18Document27 pagesChronic Renal Failure 4-9-18Muhammad MakkiNo ratings yet
- Cirrhosis Copy FINAL EDITEDDocument42 pagesCirrhosis Copy FINAL EDITEDpraisidNo ratings yet
- Alternative NamesDocument67 pagesAlternative NamespashaNo ratings yet
- AcuterenalfailureDocument3 pagesAcuterenalfailureJessica JacksonNo ratings yet
- Dr.P.Sankaranarayanan MD: Emeritus Professor of Medicine Acs Medical College & HospitalDocument81 pagesDr.P.Sankaranarayanan MD: Emeritus Professor of Medicine Acs Medical College & HospitalvaishnaviNo ratings yet
- AKI Acute Kidney InjuryDocument46 pagesAKI Acute Kidney InjuryVia AnggraeniNo ratings yet
- Acute Chronic Kidney InjuryDocument29 pagesAcute Chronic Kidney InjuryPriya GKNo ratings yet
- 7.acute Renal Failure (ARF)Document20 pages7.acute Renal Failure (ARF)Mahesh RathnayakeNo ratings yet
- 2D2016 3.4-2 Azotemia and Urinary Abnormalities (Harrison's)Document7 pages2D2016 3.4-2 Azotemia and Urinary Abnormalities (Harrison's)elleinas100% (1)
- 6 Aurora LoaezaDocument21 pages6 Aurora LoaezaGaby CrespoNo ratings yet
- Acute Renal FailureDocument32 pagesAcute Renal FailureTharen OfficialNo ratings yet
- Acute Renal FailureDocument13 pagesAcute Renal FailureGlorianne Palor100% (2)
- Acuterenalfailure2filesmerged 190509071023Document85 pagesAcuterenalfailure2filesmerged 190509071023ellise abundoNo ratings yet
- Acute Kidney Injury: Sarah Abigail C. Ong Siu Second Year ResidentDocument41 pagesAcute Kidney Injury: Sarah Abigail C. Ong Siu Second Year ResidentSarah Ong SiuNo ratings yet
- Exam 2 STUDY GUIDEDocument121 pagesExam 2 STUDY GUIDEJulie BrandtNo ratings yet
- Approach To Chronic Kidney DiseaseDocument32 pagesApproach To Chronic Kidney DiseasebgfhnfgNo ratings yet
- Renal Replacement TherapyDocument23 pagesRenal Replacement TherapybgfhnfgNo ratings yet
- Urinary Tract InfectionsDocument20 pagesUrinary Tract Infectionsbgfhnfg100% (1)
- FC Path (SA) Viro Regulations 12 7 2020Document9 pagesFC Path (SA) Viro Regulations 12 7 2020bgfhnfgNo ratings yet
- Dip For Med (SA) Clin Regulations 10 8 2020Document17 pagesDip For Med (SA) Clin Regulations 10 8 2020bgfhnfgNo ratings yet
- Robbins & Cotran Pathologic Basis of Disease - With STUDENT CONSULT Online Access, 8e (PDFDrive - Com) - 89-105Document17 pagesRobbins & Cotran Pathologic Basis of Disease - With STUDENT CONSULT Online Access, 8e (PDFDrive - Com) - 89-105bgfhnfgNo ratings yet
- Dettol Liquid Hand Wash SDSDocument10 pagesDettol Liquid Hand Wash SDSaskdfhaosljudgnNo ratings yet
- Emax 2222Document85 pagesEmax 2222camNo ratings yet
- Nepro Plastics Pvc4Document12 pagesNepro Plastics Pvc4chaouch.najehNo ratings yet
- Timken GreaseDocument68 pagesTimken Greasesf wNo ratings yet
- Life Processes - CBSE Class 10 BiologyDocument7 pagesLife Processes - CBSE Class 10 BiologyGurukul24x775% (8)
- 1 - Ne - b2 Sety Leksykalne U7iDocument1 page1 - Ne - b2 Sety Leksykalne U7iAneta WalejewskaNo ratings yet
- Membrane Based SeparationDocument2 pagesMembrane Based SeparationRitika RawatNo ratings yet
- FCR Solution: System ConfigurationDocument3 pagesFCR Solution: System ConfigurationLaura CorderoNo ratings yet
- Pelaporan IKP Puskesmas Arjaty Daud 2022Document16 pagesPelaporan IKP Puskesmas Arjaty Daud 2022Fajar Slalu CeriaNo ratings yet
- Long Term LiabilitiesDocument21 pagesLong Term Liabilitiesnioriatti8924No ratings yet
- 29102015000000B - Boehler DCMS-IG - SWDocument1 page29102015000000B - Boehler DCMS-IG - SWErdinc BayatNo ratings yet
- Cylinder Safety Poster (ID 801089) 042019 B2 500x700mmDocument1 pageCylinder Safety Poster (ID 801089) 042019 B2 500x700mmChris TeohNo ratings yet
- Chemistry InvestigatoryDocument15 pagesChemistry InvestigatoryTushar JaiswalNo ratings yet
- 09 em 002Document6 pages09 em 002Zelva ChileNo ratings yet
- Individual Weekly Home Learning Plan: Palina East National High SchoolDocument4 pagesIndividual Weekly Home Learning Plan: Palina East National High Schoolmark joseph cometaNo ratings yet
- Interpretation of The Maha Dasha of KetuDocument25 pagesInterpretation of The Maha Dasha of Ketuktpadmanabhan9202100% (1)
- Phy Investigatory Project Tangent GalvanDocument11 pagesPhy Investigatory Project Tangent Galvankomal mahelaNo ratings yet
- Electronic Reservation Slip (ERS) : 6617575281 12102/jananeswari Exp Ac 3 Tier Sleeper (3A)Document2 pagesElectronic Reservation Slip (ERS) : 6617575281 12102/jananeswari Exp Ac 3 Tier Sleeper (3A)Sparsh SharmaNo ratings yet
- Env LawDocument16 pagesEnv LawHeena ShaikhNo ratings yet
- CVDocument2 pagesCVTaha Akhtar KhanNo ratings yet
- Practical Bacteriology Laboratory Manual: Prepared byDocument37 pagesPractical Bacteriology Laboratory Manual: Prepared bysalamon2tNo ratings yet
- Kiln Inlet Analyzer.: CalibrationDocument3 pagesKiln Inlet Analyzer.: CalibrationZakariya ChoudharyNo ratings yet
- 11 Plus Comprehension Summary Test Paper 4 IjhDocument12 pages11 Plus Comprehension Summary Test Paper 4 IjhKrishnapriya GovindNo ratings yet
- Organic Termite Killer As Replacement To Chemical InsecticidesDocument13 pagesOrganic Termite Killer As Replacement To Chemical InsecticidesROSELYN RAMOSNo ratings yet
- Skripsi Alvi AkmaliaDocument94 pagesSkripsi Alvi Akmaliakhoiriah nasutionNo ratings yet
- 5-x Exam 5-Study Guide-Urinary SystemDocument9 pages5-x Exam 5-Study Guide-Urinary SystemAllison GajadharNo ratings yet
- H. P. Lovecraft - PolarisDocument3 pagesH. P. Lovecraft - PolarisBárbara AlvesNo ratings yet
- Playground and Water Safety GuidelinesDocument50 pagesPlayground and Water Safety GuidelinesNgoc Nhu NguyenNo ratings yet
- Drying Bed Design PDFDocument29 pagesDrying Bed Design PDFAshokNo ratings yet





























































































Download as pptx, pdf, or txt
You might also like
- Chapter 15-Basics of Electrical Systems: True/FalseDocument190 pagesChapter 15-Basics of Electrical Systems: True/FalsewesamNo ratings yet
- Acute Renal FailureDocument33 pagesAcute Renal FailureAqsa Akbar AliNo ratings yet
- Acute Renal Failure - PPT 1Document36 pagesAcute Renal Failure - PPT 1Jay Paul100% (1)
- Renal Acute Kidney InjuryDocument41 pagesRenal Acute Kidney InjuryTim SilvaNo ratings yet
- Noel A. Villanueva, MD, FPCP, FPSNDocument62 pagesNoel A. Villanueva, MD, FPCP, FPSNagilNo ratings yet
- Acute Renal Failure Lecture 1 Critical Care Nursing NewDocument41 pagesAcute Renal Failure Lecture 1 Critical Care Nursing NewEdwin Jose SNo ratings yet
- Nephrology & Urology: Archer Online USMLE ReviewsDocument107 pagesNephrology & Urology: Archer Online USMLE ReviewsBeerappaJanpetNo ratings yet
- Management of Acute Kidney InjuryDocument31 pagesManagement of Acute Kidney InjurysumitNo ratings yet
- AkiDocument38 pagesAkiPhillip MartinezNo ratings yet
- Alternative NamesDocument67 pagesAlternative NamespashaNo ratings yet
- Acute Kidney InjuryDocument60 pagesAcute Kidney InjuryAbegail Fermanejo-GeneraoNo ratings yet
- 22.AKI ProtocolDocument2 pages22.AKI ProtocolRed DevilNo ratings yet
- Acute Renal Failure Lecture 1 Critical Care NursingDocument52 pagesAcute Renal Failure Lecture 1 Critical Care NursingDina Rasmita100% (2)
- Acute Renal FailureDocument10 pagesAcute Renal FailureSypheruNo ratings yet
- Acute Renal FailureDocument28 pagesAcute Renal FailureAs SyarifNo ratings yet
- Acute Kidney Injury: DR Hodan Ahmed Dept of Pediatrics and Child Health Amoud Medical School, AUDocument32 pagesAcute Kidney Injury: DR Hodan Ahmed Dept of Pediatrics and Child Health Amoud Medical School, AUMohamoud MohamedNo ratings yet
- Caz Clinic - IRADocument35 pagesCaz Clinic - IRAIonela Roberta100% (1)
- AkiDocument42 pagesAkimarauder_popNo ratings yet
- Acute Renal FailureDocument31 pagesAcute Renal FailureODONG MARTINNo ratings yet
- Dr. Tjatur Winarsanto SPPDDocument37 pagesDr. Tjatur Winarsanto SPPDEndah Risky GustiyantiNo ratings yet
- Acute Kidney Injury (AKI) : by Prof Grace Irimu Consultant Pediatrician and NephrologistDocument43 pagesAcute Kidney Injury (AKI) : by Prof Grace Irimu Consultant Pediatrician and Nephrologistokwadha simionNo ratings yet
- Approach To Acute Renal FailureDocument40 pagesApproach To Acute Renal FailureMochammad Fariz AmsalNo ratings yet
- Acute Renal Failure BDocument60 pagesAcute Renal Failure BEzekiel moraraNo ratings yet
- DR Ankit Soni DNB Trainee (Peds)Document28 pagesDR Ankit Soni DNB Trainee (Peds)Ankit SoniNo ratings yet
- Acute and Chronic Renal Failure MyDocument45 pagesAcute and Chronic Renal Failure MyJoseph Krafft100% (3)
- Acute Renal FailureDocument33 pagesAcute Renal Failureimranqazi11No ratings yet
- Cirrhosis of LiverDocument106 pagesCirrhosis of LiveraahadNo ratings yet
- Acute Kidney InjuryDocument23 pagesAcute Kidney InjuryBaraka SayoreNo ratings yet
- Nursing Management of AKIDocument24 pagesNursing Management of AKIheenamaharjanNo ratings yet
- Acute& Chronic Kidney DiseaseDocument91 pagesAcute& Chronic Kidney DiseaseSonia YadavNo ratings yet
- Manajemen Anestesi Pada Uremic SyndromeDocument27 pagesManajemen Anestesi Pada Uremic SyndromeAdi Nugroho MelyanaNo ratings yet
- Renal FailureDocument23 pagesRenal FailurerjfeeleyNo ratings yet
- Renal Faliure 1Document50 pagesRenal Faliure 1180045No ratings yet
- Acute Kidney InjuryDocument3 pagesAcute Kidney InjuryHarkirat AtwalNo ratings yet
- Acute Renal FailureDocument75 pagesAcute Renal FailureAshwin Raghav SankarNo ratings yet
- Renal Calculi & Renal FailureDocument17 pagesRenal Calculi & Renal Failureazlan100% (1)
- Kidney: Disorders of TheDocument52 pagesKidney: Disorders of ThejuliusromatolentinoNo ratings yet
- Acute Renal Failure: DR Grania PriceDocument24 pagesAcute Renal Failure: DR Grania PriceCastro KisuuleNo ratings yet
- Acute Renal Failure: Dr. Sami Abdo RadmanDocument23 pagesAcute Renal Failure: Dr. Sami Abdo RadmanAdeniran CharlesNo ratings yet
- Aki - CKDDocument51 pagesAki - CKDAyu Luh Ratri WeningNo ratings yet
- Acute Renal FailureDocument10 pagesAcute Renal FailureAlia PutriNo ratings yet
- Acute Kidney Injury: Syakib BakriDocument46 pagesAcute Kidney Injury: Syakib BakriBhisma D. SyaputraNo ratings yet
- Acute Kidney InjuryDocument40 pagesAcute Kidney InjuryNabin SimkhadaNo ratings yet
- Final AKI For IM 2014Document45 pagesFinal AKI For IM 2014Andika Yusuf RamadhanNo ratings yet
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisDocument35 pagesLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanNo ratings yet
- Chronic Renal Failure 4-9-18Document27 pagesChronic Renal Failure 4-9-18Muhammad MakkiNo ratings yet
- Cirrhosis Copy FINAL EDITEDDocument42 pagesCirrhosis Copy FINAL EDITEDpraisidNo ratings yet
- Alternative NamesDocument67 pagesAlternative NamespashaNo ratings yet
- AcuterenalfailureDocument3 pagesAcuterenalfailureJessica JacksonNo ratings yet
- Dr.P.Sankaranarayanan MD: Emeritus Professor of Medicine Acs Medical College & HospitalDocument81 pagesDr.P.Sankaranarayanan MD: Emeritus Professor of Medicine Acs Medical College & HospitalvaishnaviNo ratings yet
- AKI Acute Kidney InjuryDocument46 pagesAKI Acute Kidney InjuryVia AnggraeniNo ratings yet
- Acute Chronic Kidney InjuryDocument29 pagesAcute Chronic Kidney InjuryPriya GKNo ratings yet
- 7.acute Renal Failure (ARF)Document20 pages7.acute Renal Failure (ARF)Mahesh RathnayakeNo ratings yet
- 2D2016 3.4-2 Azotemia and Urinary Abnormalities (Harrison's)Document7 pages2D2016 3.4-2 Azotemia and Urinary Abnormalities (Harrison's)elleinas100% (1)
- 6 Aurora LoaezaDocument21 pages6 Aurora LoaezaGaby CrespoNo ratings yet
- Acute Renal FailureDocument32 pagesAcute Renal FailureTharen OfficialNo ratings yet
- Acute Renal FailureDocument13 pagesAcute Renal FailureGlorianne Palor100% (2)
- Acuterenalfailure2filesmerged 190509071023Document85 pagesAcuterenalfailure2filesmerged 190509071023ellise abundoNo ratings yet
- Acute Kidney Injury: Sarah Abigail C. Ong Siu Second Year ResidentDocument41 pagesAcute Kidney Injury: Sarah Abigail C. Ong Siu Second Year ResidentSarah Ong SiuNo ratings yet
- Exam 2 STUDY GUIDEDocument121 pagesExam 2 STUDY GUIDEJulie BrandtNo ratings yet
- Approach To Chronic Kidney DiseaseDocument32 pagesApproach To Chronic Kidney DiseasebgfhnfgNo ratings yet
- Renal Replacement TherapyDocument23 pagesRenal Replacement TherapybgfhnfgNo ratings yet
- Urinary Tract InfectionsDocument20 pagesUrinary Tract Infectionsbgfhnfg100% (1)
- FC Path (SA) Viro Regulations 12 7 2020Document9 pagesFC Path (SA) Viro Regulations 12 7 2020bgfhnfgNo ratings yet
- Dip For Med (SA) Clin Regulations 10 8 2020Document17 pagesDip For Med (SA) Clin Regulations 10 8 2020bgfhnfgNo ratings yet
- Robbins & Cotran Pathologic Basis of Disease - With STUDENT CONSULT Online Access, 8e (PDFDrive - Com) - 89-105Document17 pagesRobbins & Cotran Pathologic Basis of Disease - With STUDENT CONSULT Online Access, 8e (PDFDrive - Com) - 89-105bgfhnfgNo ratings yet
- Dettol Liquid Hand Wash SDSDocument10 pagesDettol Liquid Hand Wash SDSaskdfhaosljudgnNo ratings yet
- Emax 2222Document85 pagesEmax 2222camNo ratings yet
- Nepro Plastics Pvc4Document12 pagesNepro Plastics Pvc4chaouch.najehNo ratings yet
- Timken GreaseDocument68 pagesTimken Greasesf wNo ratings yet
- Life Processes - CBSE Class 10 BiologyDocument7 pagesLife Processes - CBSE Class 10 BiologyGurukul24x775% (8)
- 1 - Ne - b2 Sety Leksykalne U7iDocument1 page1 - Ne - b2 Sety Leksykalne U7iAneta WalejewskaNo ratings yet
- Membrane Based SeparationDocument2 pagesMembrane Based SeparationRitika RawatNo ratings yet
- FCR Solution: System ConfigurationDocument3 pagesFCR Solution: System ConfigurationLaura CorderoNo ratings yet
- Pelaporan IKP Puskesmas Arjaty Daud 2022Document16 pagesPelaporan IKP Puskesmas Arjaty Daud 2022Fajar Slalu CeriaNo ratings yet
- Long Term LiabilitiesDocument21 pagesLong Term Liabilitiesnioriatti8924No ratings yet
- 29102015000000B - Boehler DCMS-IG - SWDocument1 page29102015000000B - Boehler DCMS-IG - SWErdinc BayatNo ratings yet
- Cylinder Safety Poster (ID 801089) 042019 B2 500x700mmDocument1 pageCylinder Safety Poster (ID 801089) 042019 B2 500x700mmChris TeohNo ratings yet
- Chemistry InvestigatoryDocument15 pagesChemistry InvestigatoryTushar JaiswalNo ratings yet
- 09 em 002Document6 pages09 em 002Zelva ChileNo ratings yet
- Individual Weekly Home Learning Plan: Palina East National High SchoolDocument4 pagesIndividual Weekly Home Learning Plan: Palina East National High Schoolmark joseph cometaNo ratings yet
- Interpretation of The Maha Dasha of KetuDocument25 pagesInterpretation of The Maha Dasha of Ketuktpadmanabhan9202100% (1)
- Phy Investigatory Project Tangent GalvanDocument11 pagesPhy Investigatory Project Tangent Galvankomal mahelaNo ratings yet
- Electronic Reservation Slip (ERS) : 6617575281 12102/jananeswari Exp Ac 3 Tier Sleeper (3A)Document2 pagesElectronic Reservation Slip (ERS) : 6617575281 12102/jananeswari Exp Ac 3 Tier Sleeper (3A)Sparsh SharmaNo ratings yet
- Env LawDocument16 pagesEnv LawHeena ShaikhNo ratings yet
- CVDocument2 pagesCVTaha Akhtar KhanNo ratings yet
- Practical Bacteriology Laboratory Manual: Prepared byDocument37 pagesPractical Bacteriology Laboratory Manual: Prepared bysalamon2tNo ratings yet
- Kiln Inlet Analyzer.: CalibrationDocument3 pagesKiln Inlet Analyzer.: CalibrationZakariya ChoudharyNo ratings yet
- 11 Plus Comprehension Summary Test Paper 4 IjhDocument12 pages11 Plus Comprehension Summary Test Paper 4 IjhKrishnapriya GovindNo ratings yet
- Organic Termite Killer As Replacement To Chemical InsecticidesDocument13 pagesOrganic Termite Killer As Replacement To Chemical InsecticidesROSELYN RAMOSNo ratings yet
- Skripsi Alvi AkmaliaDocument94 pagesSkripsi Alvi Akmaliakhoiriah nasutionNo ratings yet
- 5-x Exam 5-Study Guide-Urinary SystemDocument9 pages5-x Exam 5-Study Guide-Urinary SystemAllison GajadharNo ratings yet
- H. P. Lovecraft - PolarisDocument3 pagesH. P. Lovecraft - PolarisBárbara AlvesNo ratings yet
- Playground and Water Safety GuidelinesDocument50 pagesPlayground and Water Safety GuidelinesNgoc Nhu NguyenNo ratings yet
- Drying Bed Design PDFDocument29 pagesDrying Bed Design PDFAshokNo ratings yet