Download as pptx, pdf, or txt
You might also like
- Q1 PR2 LAS WEEK 3 Kinds of VariablesDocument16 pagesQ1 PR2 LAS WEEK 3 Kinds of VariablesAnalie Cabanlit100% (4)
- Malaria: DR Sulaiman Conteh Medical StudentsDocument36 pagesMalaria: DR Sulaiman Conteh Medical StudentsAbubakar JallohNo ratings yet
- Bio MalariaDocument10 pagesBio MalariaAnonymous 42shXQPSjNo ratings yet
- MALARIA (Autosaved)Document16 pagesMALARIA (Autosaved)Mpanso Ahmad AlhijjNo ratings yet
- Protozoa 1Document6 pagesProtozoa 1Farhat KhanNo ratings yet
- E MalariaDocument40 pagesE MalariaUmair AliNo ratings yet
- Anti Malarial AgentsDocument23 pagesAnti Malarial AgentsJia YingNo ratings yet
- MalariaDocument34 pagesMalariaKidistNo ratings yet
- Plasm Odium SDocument9 pagesPlasm Odium SAnonymous 7zl6IBNo ratings yet
- Malaria FalciparumDocument35 pagesMalaria FalciparumAboubakar Moalim Mahad moh'dNo ratings yet
- Lec 9 MalariaDocument42 pagesLec 9 MalariaMye AkmaNo ratings yet
- MalariaDocument62 pagesMalariaYousuf skNo ratings yet
- MalariaDocument49 pagesMalaria2253010837No ratings yet
- MalariaDocument15 pagesMalariaEssa KhanNo ratings yet
- BIO3242 - Lecture 3Document86 pagesBIO3242 - Lecture 3NGOGA NISINGIZWE NESTORNo ratings yet
- Parasitic Inclusions in ErythrocytesDocument27 pagesParasitic Inclusions in ErythrocytesLian Marie ViñasNo ratings yet
- Assingment of ParasateDocument36 pagesAssingment of ParasateHibaaq AxmedNo ratings yet
- Plasmodium SPPDocument15 pagesPlasmodium SPPMuhammad MuneebNo ratings yet
- P. VivaxDocument33 pagesP. VivaxAboubakar Moalim Mahad moh'dNo ratings yet
- Unit 11. Blood and Tissue Coccidian (Apicomplexa)Document40 pagesUnit 11. Blood and Tissue Coccidian (Apicomplexa)Michael DawitNo ratings yet
- MalariaDocument28 pagesMalariaAbdul AtaNo ratings yet
- Plasmodium Ovale: Phylum Subphylum Class Subclass Family Genes Species:Plasmodium OvaleDocument36 pagesPlasmodium Ovale: Phylum Subphylum Class Subclass Family Genes Species:Plasmodium OvaleAditya MuchayatsyahNo ratings yet
- Lecture 10 (Plasmodium) (F)Document59 pagesLecture 10 (Plasmodium) (F)jolan.freedomNo ratings yet
- Malaria 1Document20 pagesMalaria 1Ankush GahlotNo ratings yet
- Patogenesis Malaria - Dr. A. Visi Kartika, SP - PADocument26 pagesPatogenesis Malaria - Dr. A. Visi Kartika, SP - PAahmadyawidyatmaNo ratings yet
- Major Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemDocument121 pagesMajor Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemƯớc Của BếttingNo ratings yet
- Major Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemDocument128 pagesMajor Bacteria Infecting The Hematology System 2. Major Parasites Infecting The Hematologic SystemƯớc Của BếttingNo ratings yet
- MalariaDocument16 pagesMalariachachamwangoNo ratings yet
- 10 Parasit Malaria. P.falciparum Dan P.vivaxDocument26 pages10 Parasit Malaria. P.falciparum Dan P.vivaxLABOR BMCNo ratings yet
- Parasitic Causes of HaematologyDocument65 pagesParasitic Causes of HaematologySolomonNo ratings yet
- Jordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDocument20 pagesJordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDaniel AtiehNo ratings yet
- Malaria M1Document102 pagesMalaria M1frankozed1No ratings yet
- Malaria Trans EditedDocument4 pagesMalaria Trans EditedSven OrdanzaNo ratings yet
- PlasmodiumDocument20 pagesPlasmodiummah noorNo ratings yet
- Jordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDocument20 pagesJordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDaniel AtiehNo ratings yet
- Protozoa. Sporozoa. Haemosporidia (The Malaria Parasites)Document22 pagesProtozoa. Sporozoa. Haemosporidia (The Malaria Parasites)Sharan MurugaboopathyNo ratings yet
- Jordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDocument20 pagesJordan University Faculty of Dentistry DR Mohammad Al-Tamimi, MD, PHDDaniel AtiehNo ratings yet
- Med. Parasitology 2022Document46 pagesMed. Parasitology 2022Atintande CamilusNo ratings yet
- SESSION 16-Malaria and TrypanosomiasisDocument46 pagesSESSION 16-Malaria and Trypanosomiasisgbunyara100No ratings yet
- Protozoa InfectionsDocument71 pagesProtozoa InfectionsfaithjoycelineNo ratings yet
- Pathology of Malaria and Haemoglobinopathies - 051213Document50 pagesPathology of Malaria and Haemoglobinopathies - 051213Miracle OdenigboNo ratings yet
- Collette MalariaDocument47 pagesCollette Malariacollinsmwila98No ratings yet
- Plasmodium ReportDocument43 pagesPlasmodium ReportGenessa Agustin BuenafeNo ratings yet
- MedicalMicrobiology&Parasitology 2Document9 pagesMedicalMicrobiology&Parasitology 222mls0115No ratings yet
- Plasmodium SPP.: Parasitology DeptDocument38 pagesPlasmodium SPP.: Parasitology DeptDedy SavradinataNo ratings yet
- Presentation On Malaria (Autosaved)Document21 pagesPresentation On Malaria (Autosaved)zoeakatNo ratings yet
- Malaria and Climate Change1248scribdDocument3 pagesMalaria and Climate Change1248scribdGuadalupe JamesNo ratings yet
- المحاضرة 11 و 12 مادة الطفيلياتDocument18 pagesالمحاضرة 11 و 12 مادة الطفيلياتdyabw6430No ratings yet
- Malaria 141112210953 Conversion Gate02Document33 pagesMalaria 141112210953 Conversion Gate02shubham vermaNo ratings yet
- HandoutsDocument22 pagesHandoutschayChay gapolNo ratings yet
- PlasmodiumDocument99 pagesPlasmodiumCharlene SuliganNo ratings yet
- Plasmodium MalariaDocument21 pagesPlasmodium MalariaSarahNo ratings yet
- Chapter 6 (Hemoparasites)Document58 pagesChapter 6 (Hemoparasites)cheru koreNo ratings yet
- Plasmodium SpeciesDocument61 pagesPlasmodium SpeciesSubhas KarnaNo ratings yet
- PlasmodiumDocument15 pagesPlasmodiumanil singhNo ratings yet
- Protozoan DiseasesDocument10 pagesProtozoan DiseasesmarijaNo ratings yet
- MalariaDocument57 pagesMalariaDawit g/kidanNo ratings yet
- Plasmodiumspp 230727053539 5ffdb015Document51 pagesPlasmodiumspp 230727053539 5ffdb015راوند اعبيدNo ratings yet
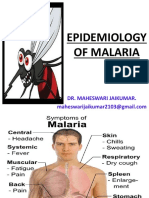
- Epidemiology of Malaria: Dr. Maheswari JaikumarDocument70 pagesEpidemiology of Malaria: Dr. Maheswari JaikumarBijay Kumar MahatoNo ratings yet
- MalariaDocument4 pagesMalarianafrabNo ratings yet
- Okatse Canyon: Mások Ezeket Keresték MégDocument1 pageOkatse Canyon: Mások Ezeket Keresték Mégtom kemNo ratings yet
- World's Famous NewspapersDocument8 pagesWorld's Famous NewspapersgopiganjaNo ratings yet
- Application Activity: Giving BackDocument3 pagesApplication Activity: Giving BackHillary Anne BautistaNo ratings yet
- An Empirical Equation Relating Fatigue Limit and Mean Stress - NASA PDFDocument31 pagesAn Empirical Equation Relating Fatigue Limit and Mean Stress - NASA PDFjohnyboyNo ratings yet
- Westbourne Baptist Church NW CalgaryDocument4 pagesWestbourne Baptist Church NW CalgaryBonnie BaldwinNo ratings yet
- Reguladores de Voltaje 79xxDocument13 pagesReguladores de Voltaje 79xxJuan Angel Cerda GuerraNo ratings yet
- BoilssdDocument3 pagesBoilssdZaid KhanNo ratings yet
- ADAPTED SportsDocument20 pagesADAPTED SportsWalter San LuisNo ratings yet
- Project Management Plan Template ProcessDocument7 pagesProject Management Plan Template ProcessShanekia Lawson-WellsNo ratings yet
- Rrl-Team 5Document10 pagesRrl-Team 5Alea AicoNo ratings yet
- Asav QuickDocument26 pagesAsav QuickWamba Gotico LeonNo ratings yet
- Software Manual Ifm 7391009UKDocument19 pagesSoftware Manual Ifm 7391009UKpatriciobenavidesmNo ratings yet
- Lesson 1 Principles and TheoriesDocument11 pagesLesson 1 Principles and TheoriesJoycee BoNo ratings yet
- Group Discussion 1Document15 pagesGroup Discussion 1salman10993No ratings yet
- Wisdom-Sophia: Contrasting Approaches To A Complex ThemeDocument12 pagesWisdom-Sophia: Contrasting Approaches To A Complex ThemeDramonesNo ratings yet
- Ap Biology Mid Term PretestDocument30 pagesAp Biology Mid Term PretestKrisnavimala Krishnan0% (1)
- Automatic Sorting MachineDocument6 pagesAutomatic Sorting Machinemuhammad ranggaNo ratings yet
- TCRWP Running Records Guidebook A-K - Literacy InterventionDocument22 pagesTCRWP Running Records Guidebook A-K - Literacy InterventionBeggo double GNo ratings yet
- L.chandra Vs Union of IndiaDocument15 pagesL.chandra Vs Union of IndiaKashish GaurNo ratings yet
- Vocabulary + Grammar Unit 3 Test ADocument3 pagesVocabulary + Grammar Unit 3 Test AJoana FernandesNo ratings yet
- Atmospheric LayersDocument5 pagesAtmospheric LayersMary Jane Magat EspirituNo ratings yet
- Level 1 - Cambridge Vocab For IELTS, English, Ielts - MemriseDocument3 pagesLevel 1 - Cambridge Vocab For IELTS, English, Ielts - MemrisetunisianouNo ratings yet
- English Quiz by Mohammad Shoaib PDFDocument11 pagesEnglish Quiz by Mohammad Shoaib PDFSHUAIB UDDAINNo ratings yet
- The Effects of Two Instrumentation Techniques For VDW - Rotate InstDocument8 pagesThe Effects of Two Instrumentation Techniques For VDW - Rotate InstRodrigo Cassana RojasNo ratings yet
- PFR IV Family CodeDocument152 pagesPFR IV Family CodeJennelie jandusayNo ratings yet
- 1 s2.0 S0888327017305654 MainDocument10 pages1 s2.0 S0888327017305654 MainchinnavenkateswarluNo ratings yet
- Jadual Alimah 2021.V3Document6 pagesJadual Alimah 2021.V3maryam cookNo ratings yet
- Research Paper #6Document9 pagesResearch Paper #6Venice Claire CabiliNo ratings yet
- Does God ExistDocument8 pagesDoes God ExistNeda StefanovicNo ratings yet