Download as pptx, pdf, or txt
You might also like
- Question Test 2 Oshm Aug 2021Document3 pagesQuestion Test 2 Oshm Aug 2021Syamala 29No ratings yet
- Santa Ana PampangaDocument7 pagesSanta Ana PampangaKarma AkabaneNo ratings yet
- Lesson 4: The Self in Western and Eastern Thoughts: Tips and Tools For Creating and Presenting Wide Format SlidesDocument18 pagesLesson 4: The Self in Western and Eastern Thoughts: Tips and Tools For Creating and Presenting Wide Format SlidesKarma Akabane92% (12)
- N7 by Novo - Methods of ContraceptionDocument34 pagesN7 by Novo - Methods of ContraceptionEllen Rose NovoNo ratings yet
- Reproductive Health (Edustudy Point) - UnlockedDocument6 pagesReproductive Health (Edustudy Point) - UnlockedSam ManochaNo ratings yet
- Psyc1013 Lesson 6.1Document65 pagesPsyc1013 Lesson 6.1LEXIZZZNo ratings yet
- Reproductive Systems and Sexual HealthDocument6 pagesReproductive Systems and Sexual HealthAira Shane MargesNo ratings yet
- Sexually Transmitted DeseasesDocument25 pagesSexually Transmitted DeseasesTith SeavmeyNo ratings yet
- Reproductivehealthppt 140331090032 Phpapp02Document25 pagesReproductivehealthppt 140331090032 Phpapp02Antarip Acharya100% (2)
- NAMES: Salapang, Pureza Maye M. GRADE: BSN - 1 DATE: October 7, 2020Document18 pagesNAMES: Salapang, Pureza Maye M. GRADE: BSN - 1 DATE: October 7, 2020Pureza Maye SalapangNo ratings yet
- Family Planning and HormonalDocument44 pagesFamily Planning and HormonalAbdinafa Mahamud DiriyeNo ratings yet
- Concept Tutorial: Presented byDocument35 pagesConcept Tutorial: Presented byBhavna SinghNo ratings yet
- Notes Chap 04Document8 pagesNotes Chap 04umamahfarooq75No ratings yet
- Reproductive HealthDocument8 pagesReproductive HealthPriyaa MNo ratings yet
- Chapter 2 Lesson 1Document3 pagesChapter 2 Lesson 1John Carldel VivoNo ratings yet
- Sexually Transmitted Diseases : (Gonorrhea, Syphilis & Aids)Document54 pagesSexually Transmitted Diseases : (Gonorrhea, Syphilis & Aids)joel david knda mjNo ratings yet
- Reproductive HealthDocument16 pagesReproductive HealthShazia Khatoon100% (1)
- Reproductive Health-Problems & StrategiesDocument11 pagesReproductive Health-Problems & StrategiesUtkarsh SinghNo ratings yet
- Human Reproductive HealthDocument5 pagesHuman Reproductive HealthDikansha JasaiwalNo ratings yet
- Reproductive HealthDocument22 pagesReproductive Healthadityakumar50067No ratings yet
- Family PlanningDocument30 pagesFamily PlanningDIPENDRA CHAUDHARYNo ratings yet
- Notes 230615 181512 DeaDocument5 pagesNotes 230615 181512 DeaAadilNo ratings yet
- Contraceptive Assignment AdihailuDocument46 pagesContraceptive Assignment AdihailuAbas AhmedNo ratings yet
- 11 Nursing Care To Promote Fetal and Maternal HealthDocument45 pages11 Nursing Care To Promote Fetal and Maternal HealthJn CasuelaNo ratings yet
- Family Planning QuizDocument22 pagesFamily Planning QuizEllen FranciskaS1KebNo ratings yet
- 4.1: Reproductive Health-Problems and StrategiesDocument5 pages4.1: Reproductive Health-Problems and StrategiesSarthi GNo ratings yet
- Module 8 - The Diversity of Human SexualityDocument26 pagesModule 8 - The Diversity of Human SexualityTORRES DHAREN B.No ratings yet
- Chapter - 4 Reproductive Health - WatermarkDocument19 pagesChapter - 4 Reproductive Health - Watermarkrajputzerox22No ratings yet
- Sexually Transmitted DiseasesDocument45 pagesSexually Transmitted DiseasesM'Edna AguilarNo ratings yet
- Reproductive HealthDocument9 pagesReproductive HealthvidushivbpsNo ratings yet
- Reproductive HealthDocument80 pagesReproductive HealthSreejithKumarNo ratings yet
- Chap 4 Bio NotesDocument7 pagesChap 4 Bio NotesJignesh BhavsarNo ratings yet
- Family Planning: Under SupervisionDocument24 pagesFamily Planning: Under SupervisionValantino RamosNo ratings yet
- Physical and Sexual SelfDocument3 pagesPhysical and Sexual SelfAyreen Villegas JamarisNo ratings yet
- Family Planning - 6Document54 pagesFamily Planning - 6obarop9No ratings yet
- Reproductive Health Lec-02 Classnotes (Samapti Mam)Document11 pagesReproductive Health Lec-02 Classnotes (Samapti Mam)santoshkushwaha827No ratings yet
- Assigment د امل خليفهDocument5 pagesAssigment د امل خليفهShimaa Abdel hameedNo ratings yet
- Reproductive Health: in Urban TerritoriesDocument16 pagesReproductive Health: in Urban TerritoriesSiddharth JainNo ratings yet
- Reproductive Health Biology (Hod Notes)Document19 pagesReproductive Health Biology (Hod Notes)ankitvlogger876No ratings yet
- Reproductive Halth ProjectDocument15 pagesReproductive Halth Projectkksidhu2905No ratings yet
- Family Planning (Dr. Saleem Adil)Document54 pagesFamily Planning (Dr. Saleem Adil)salimadilNo ratings yet
- Family Planning: It's Time To Think Seriously About Family PlanningDocument10 pagesFamily Planning: It's Time To Think Seriously About Family PlanningKavya YadavNo ratings yet
- Infertility PDFDocument12 pagesInfertility PDFdian_c87100% (1)
- Population Dynamics NewDocument169 pagesPopulation Dynamics Newhiral mistry100% (1)
- Biology 1Document15 pagesBiology 1Mordhwaj Singh TomarNo ratings yet
- Reproductive Health-Protected-UnlockedDocument14 pagesReproductive Health-Protected-UnlockedDevarsh PanchalNo ratings yet
- Chapter 4 - Reproductive Health NotesDocument5 pagesChapter 4 - Reproductive Health NotesShagufta100% (1)
- Reproductive HealthDocument6 pagesReproductive HealthBiju MylachalNo ratings yet
- ContraceptivesDocument19 pagesContraceptivesTamoya ShirleyNo ratings yet
- Module 8 Uts Quiz ReviewerDocument4 pagesModule 8 Uts Quiz ReviewerCHARLES LUIGI MESANo ratings yet
- 12 Biology - Reproductive HealthDocument4 pages12 Biology - Reproductive HealthTanya Mishra100% (1)
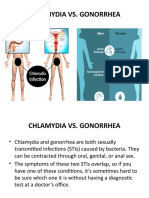
- Chlamydia Vs GonorrhoeaDocument31 pagesChlamydia Vs Gonorrhoeakyro draxNo ratings yet
- Abortifacient and ContraceptivesDocument100 pagesAbortifacient and ContraceptivesMario MorenoNo ratings yet
- Special EthicsDocument22 pagesSpecial Ethicsenzo1098No ratings yet
- Notes On ContraceptionDocument2 pagesNotes On ContraceptionImad Q. KhaleelNo ratings yet
- Population Growth and Its ManagementDocument22 pagesPopulation Growth and Its ManagementSAGAR POUDELNo ratings yet
- Family WelfareDocument17 pagesFamily WelfareValarmathiNo ratings yet
- Assessment of Fetal Well - BeingDocument40 pagesAssessment of Fetal Well - BeingFrancia ToledanoNo ratings yet
- Chapter 7 - Preventing Pregnancy Common Ways of Preventing PregnancyDocument3 pagesChapter 7 - Preventing Pregnancy Common Ways of Preventing PregnancyJennie WatanabeNo ratings yet
- Biology ProjectDocument9 pagesBiology ProjectNitesh JaiswalNo ratings yet
- TORCHDocument31 pagesTORCHRupali Arora100% (3)
- 3.torch InfectionsDocument15 pages3.torch InfectionsKuleshwar SahuNo ratings yet
- Globalization of ReligionDocument11 pagesGlobalization of ReligionKarma AkabaneNo ratings yet
- Toyota Motor Corporation: Darwin D. Ambalong (BS AIS)Document7 pagesToyota Motor Corporation: Darwin D. Ambalong (BS AIS)Karma AkabaneNo ratings yet
- Economics: Unlimited Wants ScarcityDocument27 pagesEconomics: Unlimited Wants ScarcityKarma AkabaneNo ratings yet
- Nilagang BaboyDocument1 pageNilagang BaboyKarma AkabaneNo ratings yet
- Global Divides: The North and The SouthDocument9 pagesGlobal Divides: The North and The SouthKarma AkabaneNo ratings yet
- Week 16-17 Module in Research PaperDocument5 pagesWeek 16-17 Module in Research PaperKarma AkabaneNo ratings yet
- Gives A Similar Effect From A Desired Good or Service Satisfy The Same Need From A Good or Service Replace Sagood OR ServiceDocument2 pagesGives A Similar Effect From A Desired Good or Service Satisfy The Same Need From A Good or Service Replace Sagood OR ServiceKarma AkabaneNo ratings yet
- Readings in Philippine History Quiz 3 - 4 - Midterm EXAMDocument18 pagesReadings in Philippine History Quiz 3 - 4 - Midterm EXAMKarma Akabane100% (3)
- The Causes and Effects of EarthquakesDocument4 pagesThe Causes and Effects of EarthquakesKarma AkabaneNo ratings yet
- Economic SystemsDocument6 pagesEconomic SystemsKarma AkabaneNo ratings yet
- Introduction To Quality: DHVTSU-Sto. Tomas CampusDocument53 pagesIntroduction To Quality: DHVTSU-Sto. Tomas CampusKarma AkabaneNo ratings yet
- Reality of LiesDocument2 pagesReality of LiesKarma Akabane100% (1)
- Chapter 1 Defining GlobalizationupdatedDocument51 pagesChapter 1 Defining GlobalizationupdatedKarma Akabane92% (24)
- Causes and Effects of EarthquakesDocument4 pagesCauses and Effects of EarthquakesKarma AkabaneNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Ispa Pada Orang Dewasa Di Desa Besuk Kecamatan Bantaran Kabupaten ProbolinggoDocument10 pagesFaktor-Faktor Yang Berhubungan Dengan Kejadian Ispa Pada Orang Dewasa Di Desa Besuk Kecamatan Bantaran Kabupaten ProbolinggoirfanNo ratings yet
- Impact of Trend Analysis On Quality of Finished Products in A Pharmaceutical IndustryDocument5 pagesImpact of Trend Analysis On Quality of Finished Products in A Pharmaceutical IndustryUMYU Journal of Microbiology Research (UJMR)No ratings yet
- PSM (Must Know)Document19 pagesPSM (Must Know)PranavNo ratings yet
- Contribution of Air Pollution To COPD and Small Airway DysfunctionDocument8 pagesContribution of Air Pollution To COPD and Small Airway DysfunctionWahyuNo ratings yet
- NCP HicbanDocument4 pagesNCP HicbanJenn chanNo ratings yet
- Nepali Concept of Psychological TraumaDocument28 pagesNepali Concept of Psychological TraumaAnanta ChaliseNo ratings yet
- Pharma Midterms CnsDocument67 pagesPharma Midterms CnsAL-NAZAERNo ratings yet
- Cat Record BookDocument26 pagesCat Record BookanvitNo ratings yet
- Vaccination Should Be CompulsoryDocument2 pagesVaccination Should Be CompulsoryPA ZENo ratings yet
- DownloadDocument1 pageDownloadAnderson Manuel Marquez NuñezNo ratings yet
- Benefits of Green TeaDocument2 pagesBenefits of Green TeaOWAISNo ratings yet
- Whiplash Injuries and Brain DeathDocument55 pagesWhiplash Injuries and Brain DeathAde RezekiNo ratings yet
- Acetylcholine Esterase AntibodyDocument2 pagesAcetylcholine Esterase AntibodySrinivasanNo ratings yet
- Makerere AR 67th Graduation Day2 22ndfeb2017Document40 pagesMakerere AR 67th Graduation Day2 22ndfeb2017The Independent Magazine100% (2)
- B Auch Muller 2015Document7 pagesB Auch Muller 2015AdityaNo ratings yet
- Ebnp SippDocument18 pagesEbnp SippthethayNo ratings yet
- Problem Tree RRL - Group 1Document16 pagesProblem Tree RRL - Group 1Daniel ParungaoNo ratings yet
- Report On Abhinav Bindra PDFDocument18 pagesReport On Abhinav Bindra PDFkritika.negi45No ratings yet
- Power Meditation: by Mahaswami MedhiranandaDocument7 pagesPower Meditation: by Mahaswami Medhiranandaanhadbalbir7347No ratings yet
- Khuman Life Healing IntakeDocument18 pagesKhuman Life Healing IntakehaobijampeterkhumanNo ratings yet
- Meningococcal Infection in ChildrenDocument6 pagesMeningococcal Infection in ChildrenAdrian KhomanNo ratings yet
- Psychology Research PaperDocument15 pagesPsychology Research Paperapi-509267463No ratings yet
- Área A Ciencias de La Salud: Simulacro Virtual Acem Semestral - Repaso San Marcos 2021-IDocument26 pagesÁrea A Ciencias de La Salud: Simulacro Virtual Acem Semestral - Repaso San Marcos 2021-IPERCY VITON DIAZNo ratings yet
- Tension Type HeadacheDocument18 pagesTension Type HeadacheRiris SihotangNo ratings yet
- Roflumilast - A Review of Chronic Obstructive Pulmonary Disease (COPD) TreatmentDocument18 pagesRoflumilast - A Review of Chronic Obstructive Pulmonary Disease (COPD) TreatmentMoh. FirmansahNo ratings yet
- Clinical Guidlines and Clinical PathwaysDocument32 pagesClinical Guidlines and Clinical PathwaysAmbreen Tariq100% (1)
- Texas UMW Legislative Event 2015 Legislative AgendaDocument1 pageTexas UMW Legislative Event 2015 Legislative Agendabee5834No ratings yet
- A Study On The Effectiveness of Welfare Measures Towards Employees of Coffee Day Global LTD, BangaloreDocument85 pagesA Study On The Effectiveness of Welfare Measures Towards Employees of Coffee Day Global LTD, BangaloremadhuNo ratings yet
- Safety Data Sheet: Section 1. IdentificationDocument12 pagesSafety Data Sheet: Section 1. IdentificationNihar BNo ratings yet