Download as pptx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Curriculum PlanningDocument16 pagesCurriculum Planningmanju100% (3)
- Bullying, Stalking and ExtortionDocument17 pagesBullying, Stalking and ExtortionJLafge83% (6)
- Hydatidiform MoleDocument27 pagesHydatidiform MolemanjuNo ratings yet
- Assisting With Dilatation and Curettage ProcedureDocument3 pagesAssisting With Dilatation and Curettage ProceduremanjuNo ratings yet
- Assisting in Insertion of Intrauterine Contraceptive Device (Copper-T)Document4 pagesAssisting in Insertion of Intrauterine Contraceptive Device (Copper-T)manju100% (1)
- Performing and Suturing An EpisiotomyDocument4 pagesPerforming and Suturing An EpisiotomymanjuNo ratings yet
- TeenagepregnancyDocument16 pagesTeenagepregnancymanjuNo ratings yet
- Reduction of Risk of The RadiationsDocument2 pagesReduction of Risk of The RadiationsmanjuNo ratings yet
- SimulationDocument22 pagesSimulationmanjuNo ratings yet
- How To Register A Partnership in SECDocument4 pagesHow To Register A Partnership in SECMa Zola EstelaNo ratings yet
- HCI634K - Technical Data SheetDocument8 pagesHCI634K - Technical Data SheetQuynhNo ratings yet
- Unusual Ways Usual DestinationDocument3 pagesUnusual Ways Usual DestinationLina Saad0% (1)
- Engine Throttle ControlDocument14 pagesEngine Throttle Controltiago100% (1)
- Grade 2 - 1ST Periodical TestDocument5 pagesGrade 2 - 1ST Periodical TestGAY IBANEZ100% (1)
- Test Method For DDF ProjectDocument13 pagesTest Method For DDF ProjectrantosbNo ratings yet
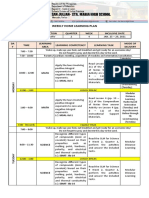
- Weekly Home Learning Plan: Grade Section Quarter Week Inclusive DateDocument3 pagesWeekly Home Learning Plan: Grade Section Quarter Week Inclusive DateMarvin Yebes ArceNo ratings yet
- Ordinary People Summary ChartDocument2 pagesOrdinary People Summary Chartangela_cristiniNo ratings yet
- CBWorld August1981 PDFDocument64 pagesCBWorld August1981 PDFbobbyunlockNo ratings yet
- Major Landforms of The Earth NotesDocument3 pagesMajor Landforms of The Earth NotesSIMMA SAI PRASANNANo ratings yet
- Past Simple Weekend.m4aDocument7 pagesPast Simple Weekend.m4aCarmen Victoria Niño RamosNo ratings yet
- DO - 159 - S2015 Duration of SchoolDocument2 pagesDO - 159 - S2015 Duration of SchoolAnonymous qg3W2rsRcGNo ratings yet
- DMPB 9015 e Rev4Document109 pagesDMPB 9015 e Rev4mohammad hazbehzadNo ratings yet
- Enya Ukuleles - Enya Music UsaDocument1 pageEnya Ukuleles - Enya Music Usav9zmmt9g7hNo ratings yet
- The Quiescent Benefits and Drawbacks of Coffee IntakeDocument6 pagesThe Quiescent Benefits and Drawbacks of Coffee IntakeVikram Singh ChauhanNo ratings yet
- Alaina Dauscher - Career Journal #01Document2 pagesAlaina Dauscher - Career Journal #01Alaina DauscherNo ratings yet
- Birinci Pozisyon Notalar Ve IsimleriDocument3 pagesBirinci Pozisyon Notalar Ve IsimleriEmre KözNo ratings yet
- Chinas Legal Strategy To Cope With US Export ContDocument9 pagesChinas Legal Strategy To Cope With US Export Contb19fd0013No ratings yet
- Saving Trees Comprehension QuestionsDocument3 pagesSaving Trees Comprehension QuestionsJayamathiVeerapa100% (1)
- ANALE - Stiinte Economice - Vol 2 - 2014 - FinalDocument250 pagesANALE - Stiinte Economice - Vol 2 - 2014 - FinalmhldcnNo ratings yet
- Manual PDFDocument3 pagesManual PDFDiego FernandezNo ratings yet
- British Baker Top Bakery Trends 2023Document15 pagesBritish Baker Top Bakery Trends 2023kiagus artaNo ratings yet
- Intrnship Report On WapdaDocument106 pagesIntrnship Report On WapdaNarain MenghwarNo ratings yet
- Desmand Whitson Resume 1PDFDocument2 pagesDesmand Whitson Resume 1PDFRed RaptureNo ratings yet
- A Bravo Delta Lancaster Model Worth 329: 38 Paralle L Paralle LDocument116 pagesA Bravo Delta Lancaster Model Worth 329: 38 Paralle L Paralle LAnonymous 7Je2SSU100% (2)
- CONSTITUTIONAL - CHANGES - TO - BE - MADE - pdf-SOME IMPORTANT CHANGES TO BE MADE IN THE LANKAN PDFDocument32 pagesCONSTITUTIONAL - CHANGES - TO - BE - MADE - pdf-SOME IMPORTANT CHANGES TO BE MADE IN THE LANKAN PDFThavam RatnaNo ratings yet
- Emu LinesDocument22 pagesEmu LinesRahul MehraNo ratings yet
- Intro To ForsciDocument16 pagesIntro To ForsciChloe MaciasNo ratings yet
- Vii-Philosophy of HPERD & SportsDocument4 pagesVii-Philosophy of HPERD & SportsAnonymous hHT0iOyQAz100% (1)