Download as pptx, pdf, or txt
You might also like
- Characters of Wisdom - Taoist Tales of The Acupuncture Points (PDFDrive) PDFDocument563 pagesCharacters of Wisdom - Taoist Tales of The Acupuncture Points (PDFDrive) PDFProf. Ivo Sampaio100% (3)
- Us 2300 MM en A4 V2 PDFDocument38 pagesUs 2300 MM en A4 V2 PDFanon_92451991350% (2)
- AARP Foundation MLM Research Study Report 10.8.18Document40 pagesAARP Foundation MLM Research Study Report 10.8.18Lindy Lou Yamilo100% (1)
- A.J. Barker's Letter To Coach KillDocument9 pagesA.J. Barker's Letter To Coach KillLeslie RolanderNo ratings yet
- Biochemical Test of BacteriaDocument33 pagesBiochemical Test of Bacteriaaziskf100% (2)
- E Book Colon Cleanse Psyllium Bentonite Clay BlendDocument16 pagesE Book Colon Cleanse Psyllium Bentonite Clay Blendsvp3761100% (2)
- Arch Expansion and LengtheningDocument105 pagesArch Expansion and Lengtheningpriyanka chaudharyNo ratings yet
- Arch ExpansionDocument140 pagesArch ExpansionBimalKrishna100% (1)
- Arch Expansion in Orthodontics / Orthodontic Courses by Indian Dental AcademyDocument152 pagesArch Expansion in Orthodontics / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Torque in OrthodonticsDocument115 pagesTorque in OrthodonticsRohini TondaNo ratings yet
- Buccal CorridorDocument3 pagesBuccal Corridoreili1100% (1)
- Slow Maxillary ExpansionDocument11 pagesSlow Maxillary Expansionteju patneediNo ratings yet
- ExpansionDocument6 pagesExpansionTejinder SinghNo ratings yet
- CANINEDocument10 pagesCANINEHarish Kumar.THOTANo ratings yet
- 5-Aetiology of MalocclusionDocument7 pages5-Aetiology of MalocclusionKhalid Mortaja100% (1)
- Bows & RetractorsDocument53 pagesBows & RetractorsSri RengalakshmiNo ratings yet
- Game Plan Sheet 1 1Document4 pagesGame Plan Sheet 1 1Coach BrownNo ratings yet
- Expansion in The Absence of Crossbite - Rationale and ProtocolDocument12 pagesExpansion in The Absence of Crossbite - Rationale and Protocoljeyran efarsani100% (1)
- Presented By: Satyam Mehta Bds Iv YrDocument29 pagesPresented By: Satyam Mehta Bds Iv YrGurdeep SinghNo ratings yet
- ActivatorDocument69 pagesActivatorParijat Chakraborty PJNo ratings yet
- Lab 2Document3 pagesLab 2Fatimah AmjedNo ratings yet
- Development of OcclusionDocument50 pagesDevelopment of OcclusionSaid Said100% (1)
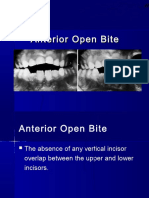
- Anterior Open BiteDocument34 pagesAnterior Open BiteAbdullah100% (1)
- Ricketts TriadDocument23 pagesRicketts TriadSonu RajuNo ratings yet
- Mode of Action of Functional Appliances / Orthodontic Courses by Indian Dental AcademyDocument116 pagesMode of Action of Functional Appliances / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Mechanics of Tooth MovementDocument19 pagesMechanics of Tooth MovementRouben ParmanumNo ratings yet
- Sunday, March 2, 2008: Important Orthodontic StudiesDocument6 pagesSunday, March 2, 2008: Important Orthodontic StudiesXnb HajiNo ratings yet
- 275 AnchorageDocument41 pages275 AnchorageMohan NathNo ratings yet
- Removable AppliancesDocument80 pagesRemovable AppliancesSurabhi SaxenaNo ratings yet
- MBT Arch FormDocument101 pagesMBT Arch Formdangi.ishu29No ratings yet
- Biostatistics and OrthodonticsDocument72 pagesBiostatistics and Orthodonticsvelangni50% (2)
- Three M's FinalDocument47 pagesThree M's Finallakshmi sagar100% (1)
- Cephalometric SuperimpositionDocument39 pagesCephalometric Superimpositionmohammed.eskanderNo ratings yet
- Miniscrew Assisted Rapid Palatal Expansion (Marpe) - ExpandingHorizons To Achieve An Optimum in Transverse Dimension A ReviewDocument15 pagesMiniscrew Assisted Rapid Palatal Expansion (Marpe) - ExpandingHorizons To Achieve An Optimum in Transverse Dimension A Reviewaa bbNo ratings yet
- 6-Ateiology of MO IIDocument8 pages6-Ateiology of MO IIKhalid Mortaja100% (1)
- Differential Diagnostic Analysis System: Clinicians' CornerDocument8 pagesDifferential Diagnostic Analysis System: Clinicians' CornerSawita KumariNo ratings yet
- Early Alt-RAMEC and Facial Mask Protocol in Class III MalocclusionDocument9 pagesEarly Alt-RAMEC and Facial Mask Protocol in Class III MalocclusionNievecillaNeiraNo ratings yet
- The Scope and Limitation of Fixed AppliancesDocument4 pagesThe Scope and Limitation of Fixed AppliancesAthirah AzizNo ratings yet
- Rotation of Jaws During Growth and Maturational and Aging ChangesDocument15 pagesRotation of Jaws During Growth and Maturational and Aging Changesshahzeb memon100% (1)
- Rapid Maxillary Expansion - A Narrative ReviewDocument8 pagesRapid Maxillary Expansion - A Narrative ReviewMADA100% (1)
- Rapid MaxillaryDocument24 pagesRapid MaxillaryDon George GeojanNo ratings yet
- Methods of Cephalometric Superimposition - A ReviewDocument4 pagesMethods of Cephalometric Superimposition - A ReviewAniket PotnisNo ratings yet
- Goals of Orthodontic TreatmentDocument14 pagesGoals of Orthodontic TreatmentemanNo ratings yet
- Fixed Orthodontic ApplianceDocument45 pagesFixed Orthodontic ApplianceBudi AthAnza SuhartonoNo ratings yet
- Bowden1978 Theoretical Considerations of Headgear Therapy 2Document10 pagesBowden1978 Theoretical Considerations of Headgear Therapy 2solodont1No ratings yet
- Normal and Abnormal Growth of The Mandible. A Synthesis of Longitudinal Cephalometric Implant Studies Over A Period of 25 YearsDocument46 pagesNormal and Abnormal Growth of The Mandible. A Synthesis of Longitudinal Cephalometric Implant Studies Over A Period of 25 Yearsegray797No ratings yet
- Development of Dentition and Occlusion: Sujina.SDocument214 pagesDevelopment of Dentition and Occlusion: Sujina.SsathyaNo ratings yet
- Basic Principles of GrowthDocument29 pagesBasic Principles of GrowthMohsin HabibNo ratings yet
- Principles of The Alexander DisciplineDocument5 pagesPrinciples of The Alexander DisciplineSarah Fauzia SiregarNo ratings yet
- Newer Orthodontic ArchwiresDocument49 pagesNewer Orthodontic ArchwiresnivethaseshaNo ratings yet
- 11.moderate Nonskeletal Problems in Preadolescent ChildrenDocument11 pages11.moderate Nonskeletal Problems in Preadolescent ChildrenyasmineNo ratings yet
- Surgically Assisted Rapid Maxillary Expansion Combined With MaxillaryDocument21 pagesSurgically Assisted Rapid Maxillary Expansion Combined With MaxillaryKumar NiwalikarNo ratings yet
- 7Document6 pages7Sungo GridsawanNo ratings yet
- C-Axis: A Growth Vector For The MaxillaDocument2 pagesC-Axis: A Growth Vector For The MaxillaMariyamNo ratings yet
- Burstone1962 PDFDocument18 pagesBurstone1962 PDFParameswaran ManiNo ratings yet
- Removable Appliance TherapyDocument6 pagesRemovable Appliance TherapyardyvanviestaNo ratings yet
- Evaluation of The Vertical Holding Appliance in Treatment of High-Angle PatientsDocument6 pagesEvaluation of The Vertical Holding Appliance in Treatment of High-Angle PatientsDrGurinder KanwarNo ratings yet
- Biomecanica PDFDocument76 pagesBiomecanica PDFxamarraNo ratings yet
- Face MaskDocument7 pagesFace MaskWaraphon JanewakornwongNo ratings yet
- Bauschinger EffectDocument2 pagesBauschinger EffectNagaVenkateshGNo ratings yet
- Arch ExpansionDocument32 pagesArch ExpansionMoola Bharath Reddy100% (5)
- Max ExpansionDocument4 pagesMax ExpansionPZNo ratings yet
- Final OrthoDocument46 pagesFinal OrthoAparna YadavNo ratings yet
- Work Safety Alert Pressed To Death by An Elevating Work PlatformDocument3 pagesWork Safety Alert Pressed To Death by An Elevating Work Platformhessian123No ratings yet
- Olear Ehv GroupDocument16 pagesOlear Ehv GroupSRINIVAS KOMMINENINo ratings yet
- Submitted JTOIDocument10 pagesSubmitted JTOIFAHIRA RAHMA NATHANIANo ratings yet
- Lemon Grass FeasibilityDocument7 pagesLemon Grass FeasibilityGanyfer DoradoNo ratings yet
- Nano Bio SensingDocument603 pagesNano Bio SensingOnyong Galarion100% (1)
- FMRC 6049 Flammable and Combustible Liquid Storage BuildingsDocument19 pagesFMRC 6049 Flammable and Combustible Liquid Storage Buildingsdyıldırım_4No ratings yet
- Properties of Concrete 3.1 Properties of ConcreteDocument4 pagesProperties of Concrete 3.1 Properties of ConcreteErwin LipardoNo ratings yet
- JP-5000 HVOF Gun: Thermal Spray Spare PartsDocument4 pagesJP-5000 HVOF Gun: Thermal Spray Spare PartsNARENDER KUMARNo ratings yet
- Project Materials Handling and Preservation ProcedureDocument2 pagesProject Materials Handling and Preservation ProcedureGbenga Mobolade100% (3)
- The Boy Scouts' First Camp Fire: by Herbert CarterDocument109 pagesThe Boy Scouts' First Camp Fire: by Herbert CarterGutenberg.orgNo ratings yet
- Hernia Surgical Mesh Implants: What Is A Hernia?Document3 pagesHernia Surgical Mesh Implants: What Is A Hernia?Vishnu KumarNo ratings yet
- Isocyanate SDocument14 pagesIsocyanate SAna VrsaljkoNo ratings yet
- NEW Chapter 4 - Product ConceptDocument21 pagesNEW Chapter 4 - Product ConceptleeminhoangrybirdNo ratings yet
- Cellular MovementsDocument27 pagesCellular MovementsngidizzmNo ratings yet
- Waste Management Technologies in Japanese Cement Industry - From Manufacturing To EcofactuaringDocument6 pagesWaste Management Technologies in Japanese Cement Industry - From Manufacturing To EcofactuaringRati YuliarningsihNo ratings yet
- CHEM 141 Lab 2 (Reactions) ProcedureDocument5 pagesCHEM 141 Lab 2 (Reactions) ProcedureKiersten RobertsNo ratings yet
- Guidelines For Human Settlement Planning and Design Redbook V2Document379 pagesGuidelines For Human Settlement Planning and Design Redbook V2Mark JacobsNo ratings yet
- Chapter 2 Area of DevelopmentDocument35 pagesChapter 2 Area of DevelopmentDon JuanNo ratings yet
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Ufc 3 600 01Document132 pagesUfc 3 600 01Juan RomeroNo ratings yet
- Hamilc10@ferris EduDocument3 pagesHamilc10@ferris Eduapi-242356240No ratings yet
- Blood Clinical CorellaionsDocument12 pagesBlood Clinical Corellaionssinte beyuNo ratings yet
- DDCP SF 04 04aDocument6 pagesDDCP SF 04 04aMohammad FarajNo ratings yet
- Lic Credit Card Application FormDocument2 pagesLic Credit Card Application FormAakash NaskarNo ratings yet
- GE Compact-Airway-Modules-Caiovx-And-CovxDocument4 pagesGE Compact-Airway-Modules-Caiovx-And-CovxmalucNo ratings yet
- 8100 Series Fire Pumps: Replacement Parts ForDocument10 pages8100 Series Fire Pumps: Replacement Parts ForAlvialvarezNo ratings yet