
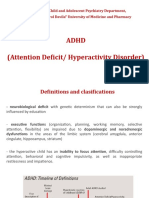
Child and Adolescent Psychiatry Department, "Carol Davila" University of Medicine and Pharmacy
Child and Adolescent Psychiatry Department, "Carol Davila" University of Medicine and Pharmacy
You might also like
- The Broad Scope of Ego Function Assessment (Leopold Bellak, Lisa Goldsmith) PDFDocument605 pagesThe Broad Scope of Ego Function Assessment (Leopold Bellak, Lisa Goldsmith) PDFAmbrose66100% (1)
- NCPDocument1 pageNCPNneka Andrea Datiles0% (2)
- Beyond Complex Trauma. An Existential View of Adverse Childhood Experiences PDFDocument17 pagesBeyond Complex Trauma. An Existential View of Adverse Childhood Experiences PDFAndreea Pal100% (1)
- DSM-5 Insanely Simplified: Unlocking The Spectrums Within DSM-5 and ICD-10 - PsychiatryDocument5 pagesDSM-5 Insanely Simplified: Unlocking The Spectrums Within DSM-5 and ICD-10 - Psychiatrylucebycu0% (1)
- Neurobiology of Attention Deficit Hyperactivity Disorder (ADHD) - A PrimerDocument37 pagesNeurobiology of Attention Deficit Hyperactivity Disorder (ADHD) - A PrimerCynde Kerr100% (2)
- Brain CureDocument157 pagesBrain CureJosh BillNo ratings yet
- Fenomenologija Adolescentskog Samoozlijeđivanja 2015Document9 pagesFenomenologija Adolescentskog Samoozlijeđivanja 2015petarvedrisNo ratings yet
- Allen Thiher, Revels in Madness. Insanity in Medicine and Literature, University of Michigan Press 1999.Document360 pagesAllen Thiher, Revels in Madness. Insanity in Medicine and Literature, University of Michigan Press 1999.vpglam100% (1)
- Prison Architecture and DesignDocument46 pagesPrison Architecture and Designbryant neutron100% (1)
- Lecture 3 2022 - ADHD, ODD, CDDocument34 pagesLecture 3 2022 - ADHD, ODD, CDEduard DinuNo ratings yet
- Evolutionary Underpinnings of Adhd: Inattention and Hyperactivity-Impulsivity: Psychobiological andDocument5 pagesEvolutionary Underpinnings of Adhd: Inattention and Hyperactivity-Impulsivity: Psychobiological andjohn fossella100% (1)
- Williams 2008Document10 pagesWilliams 2008LUIS FELIPE CHAGAS CALDEIRA CATAONo ratings yet
- Askep Adhd 2018Document24 pagesAskep Adhd 2018paulus ikeNo ratings yet
- Adhd. BioscienceDocument18 pagesAdhd. BioscienceJuan Carlos Muñoz SalmerónNo ratings yet
- AdhdDocument30 pagesAdhdНевена ЈончићNo ratings yet
- A Review of Executive Function Deficits and PharmacologicalDocument7 pagesA Review of Executive Function Deficits and Pharmacologicaljose carlos pires coelhoNo ratings yet
- Ttention Eficit Isorder: Definitions, Epidemiology, and PathophysiologyDocument15 pagesTtention Eficit Isorder: Definitions, Epidemiology, and Pathophysiologyzhe tempNo ratings yet
- Emotional Health in Attention Deficit HyperactivitDocument5 pagesEmotional Health in Attention Deficit HyperactivitAzucena DONo ratings yet
- ADHDDocument31 pagesADHDGnaneswar PiduguNo ratings yet
- Attention Defisit Hyperactivity Disorder : Kelompok 4 Pediatric Nursing PSIK UB 2017Document23 pagesAttention Defisit Hyperactivity Disorder : Kelompok 4 Pediatric Nursing PSIK UB 2017Sulis Nurul BadriyahNo ratings yet
- Aetiology of Schizophrenia - All SetDocument63 pagesAetiology of Schizophrenia - All SetAthul RajNo ratings yet
- Attention-Deficit Hyperactivity Disorder: by Chris GolnerDocument22 pagesAttention-Deficit Hyperactivity Disorder: by Chris GolnerChaé RiNo ratings yet
- Frontal Systems Dysfunction in Children With Attention-Deficit/ Hyperactivity Disorder and Learning DisabilitiesDocument8 pagesFrontal Systems Dysfunction in Children With Attention-Deficit/ Hyperactivity Disorder and Learning DisabilitiesBarry BurijonNo ratings yet
- Chapter 7 - Attention Deficit Disorder - 2018 - Integrative MedicineDocument15 pagesChapter 7 - Attention Deficit Disorder - 2018 - Integrative MedicineandreNo ratings yet
- Genro Et Al., 2010Document15 pagesGenro Et Al., 2010priyaNo ratings yet
- Etiology of ADHDDocument2 pagesEtiology of ADHDMuhammad Ihtisham KhanNo ratings yet
- Attention-Deficit /hyperactivity Disorder Evaluation and Diagnosis A Practical ApproachDocument32 pagesAttention-Deficit /hyperactivity Disorder Evaluation and Diagnosis A Practical ApproachArun GeorgeNo ratings yet
- (PEDIA) Developmental ConditionsDocument8 pages(PEDIA) Developmental ConditionsPAULINE VIVIEN ACLANNo ratings yet
- JDN 10089Document18 pagesJDN 10089Lívia MeloNo ratings yet
- Attention-Deficit/Hyperactivity Disorder (ADHD)Document38 pagesAttention-Deficit/Hyperactivity Disorder (ADHD)Amir MahmoudNo ratings yet
- A Psychophysiological Marker of Attention Deficit/Hyperactivity Disorder (ADHD) - Defining The EEG Consistency IndexDocument16 pagesA Psychophysiological Marker of Attention Deficit/Hyperactivity Disorder (ADHD) - Defining The EEG Consistency IndexneuropsicojcNo ratings yet
- Attention-Deficit/Hyperactivity DisorderDocument3 pagesAttention-Deficit/Hyperactivity DisorderAkhwand SaulatNo ratings yet
- W4-Module4 Disorders Diagnosed in Infancy, Childhood and AdolescenceDocument18 pagesW4-Module4 Disorders Diagnosed in Infancy, Childhood and AdolescenceDizon, Sharmaine L.No ratings yet
- ADHDDocument5 pagesADHDnikita.callistaNo ratings yet
- Alege CorectDocument41 pagesAlege CorectIna RomaniucNo ratings yet
- A Review of Fronto-Striatal and Fronto-Cortical Brain Abnormalities in Children and Adults With Attention Deficit Hyperactivity Disorder.Document22 pagesA Review of Fronto-Striatal and Fronto-Cortical Brain Abnormalities in Children and Adults With Attention Deficit Hyperactivity Disorder.Víctor RománNo ratings yet
- Primer: in UteroDocument6 pagesPrimer: in UteroSandra MedinaNo ratings yet
- Lecture 8 NotesDocument3 pagesLecture 8 NotesAafreen AhmedNo ratings yet
- Funciones Ejecutivas de Niños Con Trastorno Por Déficit de Atención e Hiperactividad Con o Sin Epilepsia Rolándica BenignaDocument9 pagesFunciones Ejecutivas de Niños Con Trastorno Por Déficit de Atención e Hiperactividad Con o Sin Epilepsia Rolándica BenignaCarolina GuzmánNo ratings yet
- Neuropsychiatry of Learning DisabilitiesDocument9 pagesNeuropsychiatry of Learning DisabilitiesWaheedullah AhmadiNo ratings yet
- Cognitive DisorderDocument32 pagesCognitive DisorderArra MayNo ratings yet
- Redalyc - Alteraciones Estructurales Encefálicas en El Trastorno Por Déficit de Atención e Hiperactividad Una Actualización.Document11 pagesRedalyc - Alteraciones Estructurales Encefálicas en El Trastorno Por Déficit de Atención e Hiperactividad Una Actualización.nadiareyescuvl2014No ratings yet
- Neuropsychological Assessment - M.Phil. Part 2Document4 pagesNeuropsychological Assessment - M.Phil. Part 2Shatakshi MishraNo ratings yet
- Machinskaya Et Al From The Journal Site Psy Neuro 2014Document14 pagesMachinskaya Et Al From The Journal Site Psy Neuro 2014ReginaNo ratings yet
- Neuroscience and Biobehavioral Reviews: Stephen V. FaraoneDocument16 pagesNeuroscience and Biobehavioral Reviews: Stephen V. FaraoneliliaNo ratings yet
- Complementary and Alternative Medical Therapies For Children With Attention-Deficit/ Hyperactivity Disorder (ADHD)Document15 pagesComplementary and Alternative Medical Therapies For Children With Attention-Deficit/ Hyperactivity Disorder (ADHD)Antonio DibellaNo ratings yet
- Attention-Deficit Hyperactivity Disorder: by Group 6Document18 pagesAttention-Deficit Hyperactivity Disorder: by Group 6bayu kuberaNo ratings yet
- Adhd SeminarDocument46 pagesAdhd Seminarshruti kumarNo ratings yet
- Attention-Deficit/ Hyperactivity Disorder: Hicham Baba - Med3 Psychiatry ClerkshipDocument18 pagesAttention-Deficit/ Hyperactivity Disorder: Hicham Baba - Med3 Psychiatry ClerkshipAli B. SafadiNo ratings yet
- Attention DeficitDocument40 pagesAttention DeficitAbelNo ratings yet
- Attention-Deficit/Hyperactivity Disorder: Thomas J. Spencer, MDDocument3 pagesAttention-Deficit/Hyperactivity Disorder: Thomas J. Spencer, MDJesica AlvarezNo ratings yet
- Pierpont Et Al-2015-Developmental Medicine & Child Neurology PDFDocument8 pagesPierpont Et Al-2015-Developmental Medicine & Child Neurology PDFargiaescuNo ratings yet
- Neuropsychological Profile Associated To PKAN in Its Initial Phase A Case Series ReportDocument7 pagesNeuropsychological Profile Associated To PKAN in Its Initial Phase A Case Series ReportNataly CastañedaNo ratings yet
- Nice (2008) CRDocument10 pagesNice (2008) CRCallum BromleyNo ratings yet
- Articulo Biomedical Casanova - CastejonDocument4 pagesArticulo Biomedical Casanova - CastejonLILIANA CASANOVANo ratings yet
- Attention-Deficit-Hyperactivity Disorder and Reward Deficiency SyndromeDocument26 pagesAttention-Deficit-Hyperactivity Disorder and Reward Deficiency SyndromeLauren SerafiniNo ratings yet
- New Developments in The Treatment of ADHDDocument12 pagesNew Developments in The Treatment of ADHDJamile Gonçalves PsicólogaNo ratings yet
- TX BipolarDocument7 pagesTX BipolarSILVIA JULIETH RAMIREZ BRICEÑONo ratings yet
- 2 - Attention Deficit Hyperactivity Disorder (ADHD)Document19 pages2 - Attention Deficit Hyperactivity Disorder (ADHD)Ammar AlnajjarNo ratings yet
- Clinical Case Analysis AdhdDocument5 pagesClinical Case Analysis AdhdSiobhan GreeneNo ratings yet
- TDAH y MRFDocument10 pagesTDAH y MRFJosé Oscar Tarazona La TorreNo ratings yet
- ADHD, Brain Functioning, and Transcendental Meditation PracticeDocument10 pagesADHD, Brain Functioning, and Transcendental Meditation PracticeNatseenNo ratings yet
- Manual IV (DSM-IV) of The American Psychiatric AssociationDocument24 pagesManual IV (DSM-IV) of The American Psychiatric AssociationcristieristiieNo ratings yet
- Case ReportDocument5 pagesCase ReportDenta HaritsaNo ratings yet
- Attention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHDFrom EverandAttention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHDNo ratings yet
- Child and Adolescent Behavioral Health: A Resource for Advanced Practice Psychiatric and Primary Care Practitioners in NursingFrom EverandChild and Adolescent Behavioral Health: A Resource for Advanced Practice Psychiatric and Primary Care Practitioners in NursingEdilma L. YearwoodNo ratings yet
- Marijuana and MadnessDocument236 pagesMarijuana and MadnessJesse Clayton100% (1)
- Substance Use DisorderDocument7 pagesSubstance Use DisorderSora HeartsNo ratings yet
- Psychologist Vs PsychiatristDocument2 pagesPsychologist Vs PsychiatristNuman AshrafNo ratings yet
- Psychiatric Morbidity in Cancer Patients: Original ResearchDocument8 pagesPsychiatric Morbidity in Cancer Patients: Original ResearchGautami ThirumalaisamyNo ratings yet
- Icd 10Document3 pagesIcd 10sequoyahNo ratings yet
- Ocd Resource PacketDocument47 pagesOcd Resource Packetapi-231586322No ratings yet
- Gidyq-Aa AnalysisDocument2 pagesGidyq-Aa Analysisapi-457706578No ratings yet
- Obsessive Compulsive Disorder CaseDocument2 pagesObsessive Compulsive Disorder CaseMarcela CamposNo ratings yet
- Clinicians Guide To AutismDocument20 pagesClinicians Guide To AutismNadia Desanti RachmatikaNo ratings yet
- 12th Congres SRFTTCDocument82 pages12th Congres SRFTTCValentina Anuta100% (1)
- Psychiatric NursingDocument31 pagesPsychiatric NursingSofia LiNo ratings yet
- ppt10 DISSDocument21 pagesppt10 DISSLahn Chen LauganasNo ratings yet
- Concise Guide To Ethics in Mental Health CareDocument379 pagesConcise Guide To Ethics in Mental Health Caresandrogb1977No ratings yet
- Emerging Focal Points in Depression and Anxiety: 22 ECNP Congress, IstanbulDocument92 pagesEmerging Focal Points in Depression and Anxiety: 22 ECNP Congress, Istanbuldorina.amaliaNo ratings yet
- Quiz (Perfect)Document3 pagesQuiz (Perfect)kuro hanabusaNo ratings yet
- Depression Supporting Students at School PDFDocument3 pagesDepression Supporting Students at School PDFMrié ChrsNo ratings yet
- Josephs 2006Document15 pagesJosephs 2006gvalcoNo ratings yet
- BP6 15depression PDFDocument75 pagesBP6 15depression PDFada ramosNo ratings yet
- Case 3Document3 pagesCase 3Nur AzizaNo ratings yet
- An Introduction To EFTDocument25 pagesAn Introduction To EFTdiplomat0No ratings yet
- Depression and Anxiety Disorders: Benefits of Exercise, Yoga, and MeditationDocument8 pagesDepression and Anxiety Disorders: Benefits of Exercise, Yoga, and MeditationRobiantiNo ratings yet
- Complementary Therapies in NursingDocument12 pagesComplementary Therapies in NursingHamza Ishtiaq100% (1)
- DR Russ Harris - A Non-Technical Overview of ACTDocument7 pagesDR Russ Harris - A Non-Technical Overview of ACTtoftb750% (2)























































































Download as pptx, pdf, or txt
You might also like
- The Broad Scope of Ego Function Assessment (Leopold Bellak, Lisa Goldsmith) PDFDocument605 pagesThe Broad Scope of Ego Function Assessment (Leopold Bellak, Lisa Goldsmith) PDFAmbrose66100% (1)
- NCPDocument1 pageNCPNneka Andrea Datiles0% (2)
- Beyond Complex Trauma. An Existential View of Adverse Childhood Experiences PDFDocument17 pagesBeyond Complex Trauma. An Existential View of Adverse Childhood Experiences PDFAndreea Pal100% (1)
- DSM-5 Insanely Simplified: Unlocking The Spectrums Within DSM-5 and ICD-10 - PsychiatryDocument5 pagesDSM-5 Insanely Simplified: Unlocking The Spectrums Within DSM-5 and ICD-10 - Psychiatrylucebycu0% (1)
- Neurobiology of Attention Deficit Hyperactivity Disorder (ADHD) - A PrimerDocument37 pagesNeurobiology of Attention Deficit Hyperactivity Disorder (ADHD) - A PrimerCynde Kerr100% (2)
- Brain CureDocument157 pagesBrain CureJosh BillNo ratings yet
- Fenomenologija Adolescentskog Samoozlijeđivanja 2015Document9 pagesFenomenologija Adolescentskog Samoozlijeđivanja 2015petarvedrisNo ratings yet
- Allen Thiher, Revels in Madness. Insanity in Medicine and Literature, University of Michigan Press 1999.Document360 pagesAllen Thiher, Revels in Madness. Insanity in Medicine and Literature, University of Michigan Press 1999.vpglam100% (1)
- Prison Architecture and DesignDocument46 pagesPrison Architecture and Designbryant neutron100% (1)
- Lecture 3 2022 - ADHD, ODD, CDDocument34 pagesLecture 3 2022 - ADHD, ODD, CDEduard DinuNo ratings yet
- Evolutionary Underpinnings of Adhd: Inattention and Hyperactivity-Impulsivity: Psychobiological andDocument5 pagesEvolutionary Underpinnings of Adhd: Inattention and Hyperactivity-Impulsivity: Psychobiological andjohn fossella100% (1)
- Williams 2008Document10 pagesWilliams 2008LUIS FELIPE CHAGAS CALDEIRA CATAONo ratings yet
- Askep Adhd 2018Document24 pagesAskep Adhd 2018paulus ikeNo ratings yet
- Adhd. BioscienceDocument18 pagesAdhd. BioscienceJuan Carlos Muñoz SalmerónNo ratings yet
- AdhdDocument30 pagesAdhdНевена ЈончићNo ratings yet
- A Review of Executive Function Deficits and PharmacologicalDocument7 pagesA Review of Executive Function Deficits and Pharmacologicaljose carlos pires coelhoNo ratings yet
- Ttention Eficit Isorder: Definitions, Epidemiology, and PathophysiologyDocument15 pagesTtention Eficit Isorder: Definitions, Epidemiology, and Pathophysiologyzhe tempNo ratings yet
- Emotional Health in Attention Deficit HyperactivitDocument5 pagesEmotional Health in Attention Deficit HyperactivitAzucena DONo ratings yet
- ADHDDocument31 pagesADHDGnaneswar PiduguNo ratings yet
- Attention Defisit Hyperactivity Disorder : Kelompok 4 Pediatric Nursing PSIK UB 2017Document23 pagesAttention Defisit Hyperactivity Disorder : Kelompok 4 Pediatric Nursing PSIK UB 2017Sulis Nurul BadriyahNo ratings yet
- Aetiology of Schizophrenia - All SetDocument63 pagesAetiology of Schizophrenia - All SetAthul RajNo ratings yet
- Attention-Deficit Hyperactivity Disorder: by Chris GolnerDocument22 pagesAttention-Deficit Hyperactivity Disorder: by Chris GolnerChaé RiNo ratings yet
- Frontal Systems Dysfunction in Children With Attention-Deficit/ Hyperactivity Disorder and Learning DisabilitiesDocument8 pagesFrontal Systems Dysfunction in Children With Attention-Deficit/ Hyperactivity Disorder and Learning DisabilitiesBarry BurijonNo ratings yet
- Chapter 7 - Attention Deficit Disorder - 2018 - Integrative MedicineDocument15 pagesChapter 7 - Attention Deficit Disorder - 2018 - Integrative MedicineandreNo ratings yet
- Genro Et Al., 2010Document15 pagesGenro Et Al., 2010priyaNo ratings yet
- Etiology of ADHDDocument2 pagesEtiology of ADHDMuhammad Ihtisham KhanNo ratings yet
- Attention-Deficit /hyperactivity Disorder Evaluation and Diagnosis A Practical ApproachDocument32 pagesAttention-Deficit /hyperactivity Disorder Evaluation and Diagnosis A Practical ApproachArun GeorgeNo ratings yet
- (PEDIA) Developmental ConditionsDocument8 pages(PEDIA) Developmental ConditionsPAULINE VIVIEN ACLANNo ratings yet
- JDN 10089Document18 pagesJDN 10089Lívia MeloNo ratings yet
- Attention-Deficit/Hyperactivity Disorder (ADHD)Document38 pagesAttention-Deficit/Hyperactivity Disorder (ADHD)Amir MahmoudNo ratings yet
- A Psychophysiological Marker of Attention Deficit/Hyperactivity Disorder (ADHD) - Defining The EEG Consistency IndexDocument16 pagesA Psychophysiological Marker of Attention Deficit/Hyperactivity Disorder (ADHD) - Defining The EEG Consistency IndexneuropsicojcNo ratings yet
- Attention-Deficit/Hyperactivity DisorderDocument3 pagesAttention-Deficit/Hyperactivity DisorderAkhwand SaulatNo ratings yet
- W4-Module4 Disorders Diagnosed in Infancy, Childhood and AdolescenceDocument18 pagesW4-Module4 Disorders Diagnosed in Infancy, Childhood and AdolescenceDizon, Sharmaine L.No ratings yet
- ADHDDocument5 pagesADHDnikita.callistaNo ratings yet
- Alege CorectDocument41 pagesAlege CorectIna RomaniucNo ratings yet
- A Review of Fronto-Striatal and Fronto-Cortical Brain Abnormalities in Children and Adults With Attention Deficit Hyperactivity Disorder.Document22 pagesA Review of Fronto-Striatal and Fronto-Cortical Brain Abnormalities in Children and Adults With Attention Deficit Hyperactivity Disorder.Víctor RománNo ratings yet
- Primer: in UteroDocument6 pagesPrimer: in UteroSandra MedinaNo ratings yet
- Lecture 8 NotesDocument3 pagesLecture 8 NotesAafreen AhmedNo ratings yet
- Funciones Ejecutivas de Niños Con Trastorno Por Déficit de Atención e Hiperactividad Con o Sin Epilepsia Rolándica BenignaDocument9 pagesFunciones Ejecutivas de Niños Con Trastorno Por Déficit de Atención e Hiperactividad Con o Sin Epilepsia Rolándica BenignaCarolina GuzmánNo ratings yet
- Neuropsychiatry of Learning DisabilitiesDocument9 pagesNeuropsychiatry of Learning DisabilitiesWaheedullah AhmadiNo ratings yet
- Cognitive DisorderDocument32 pagesCognitive DisorderArra MayNo ratings yet
- Redalyc - Alteraciones Estructurales Encefálicas en El Trastorno Por Déficit de Atención e Hiperactividad Una Actualización.Document11 pagesRedalyc - Alteraciones Estructurales Encefálicas en El Trastorno Por Déficit de Atención e Hiperactividad Una Actualización.nadiareyescuvl2014No ratings yet
- Neuropsychological Assessment - M.Phil. Part 2Document4 pagesNeuropsychological Assessment - M.Phil. Part 2Shatakshi MishraNo ratings yet
- Machinskaya Et Al From The Journal Site Psy Neuro 2014Document14 pagesMachinskaya Et Al From The Journal Site Psy Neuro 2014ReginaNo ratings yet
- Neuroscience and Biobehavioral Reviews: Stephen V. FaraoneDocument16 pagesNeuroscience and Biobehavioral Reviews: Stephen V. FaraoneliliaNo ratings yet
- Complementary and Alternative Medical Therapies For Children With Attention-Deficit/ Hyperactivity Disorder (ADHD)Document15 pagesComplementary and Alternative Medical Therapies For Children With Attention-Deficit/ Hyperactivity Disorder (ADHD)Antonio DibellaNo ratings yet
- Attention-Deficit Hyperactivity Disorder: by Group 6Document18 pagesAttention-Deficit Hyperactivity Disorder: by Group 6bayu kuberaNo ratings yet
- Adhd SeminarDocument46 pagesAdhd Seminarshruti kumarNo ratings yet
- Attention-Deficit/ Hyperactivity Disorder: Hicham Baba - Med3 Psychiatry ClerkshipDocument18 pagesAttention-Deficit/ Hyperactivity Disorder: Hicham Baba - Med3 Psychiatry ClerkshipAli B. SafadiNo ratings yet
- Attention DeficitDocument40 pagesAttention DeficitAbelNo ratings yet
- Attention-Deficit/Hyperactivity Disorder: Thomas J. Spencer, MDDocument3 pagesAttention-Deficit/Hyperactivity Disorder: Thomas J. Spencer, MDJesica AlvarezNo ratings yet
- Pierpont Et Al-2015-Developmental Medicine & Child Neurology PDFDocument8 pagesPierpont Et Al-2015-Developmental Medicine & Child Neurology PDFargiaescuNo ratings yet
- Neuropsychological Profile Associated To PKAN in Its Initial Phase A Case Series ReportDocument7 pagesNeuropsychological Profile Associated To PKAN in Its Initial Phase A Case Series ReportNataly CastañedaNo ratings yet
- Nice (2008) CRDocument10 pagesNice (2008) CRCallum BromleyNo ratings yet
- Articulo Biomedical Casanova - CastejonDocument4 pagesArticulo Biomedical Casanova - CastejonLILIANA CASANOVANo ratings yet
- Attention-Deficit-Hyperactivity Disorder and Reward Deficiency SyndromeDocument26 pagesAttention-Deficit-Hyperactivity Disorder and Reward Deficiency SyndromeLauren SerafiniNo ratings yet
- New Developments in The Treatment of ADHDDocument12 pagesNew Developments in The Treatment of ADHDJamile Gonçalves PsicólogaNo ratings yet
- TX BipolarDocument7 pagesTX BipolarSILVIA JULIETH RAMIREZ BRICEÑONo ratings yet
- 2 - Attention Deficit Hyperactivity Disorder (ADHD)Document19 pages2 - Attention Deficit Hyperactivity Disorder (ADHD)Ammar AlnajjarNo ratings yet
- Clinical Case Analysis AdhdDocument5 pagesClinical Case Analysis AdhdSiobhan GreeneNo ratings yet
- TDAH y MRFDocument10 pagesTDAH y MRFJosé Oscar Tarazona La TorreNo ratings yet
- ADHD, Brain Functioning, and Transcendental Meditation PracticeDocument10 pagesADHD, Brain Functioning, and Transcendental Meditation PracticeNatseenNo ratings yet
- Manual IV (DSM-IV) of The American Psychiatric AssociationDocument24 pagesManual IV (DSM-IV) of The American Psychiatric AssociationcristieristiieNo ratings yet
- Case ReportDocument5 pagesCase ReportDenta HaritsaNo ratings yet
- Attention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHDFrom EverandAttention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHDNo ratings yet
- Child and Adolescent Behavioral Health: A Resource for Advanced Practice Psychiatric and Primary Care Practitioners in NursingFrom EverandChild and Adolescent Behavioral Health: A Resource for Advanced Practice Psychiatric and Primary Care Practitioners in NursingEdilma L. YearwoodNo ratings yet
- Marijuana and MadnessDocument236 pagesMarijuana and MadnessJesse Clayton100% (1)
- Substance Use DisorderDocument7 pagesSubstance Use DisorderSora HeartsNo ratings yet
- Psychologist Vs PsychiatristDocument2 pagesPsychologist Vs PsychiatristNuman AshrafNo ratings yet
- Psychiatric Morbidity in Cancer Patients: Original ResearchDocument8 pagesPsychiatric Morbidity in Cancer Patients: Original ResearchGautami ThirumalaisamyNo ratings yet
- Icd 10Document3 pagesIcd 10sequoyahNo ratings yet
- Ocd Resource PacketDocument47 pagesOcd Resource Packetapi-231586322No ratings yet
- Gidyq-Aa AnalysisDocument2 pagesGidyq-Aa Analysisapi-457706578No ratings yet
- Obsessive Compulsive Disorder CaseDocument2 pagesObsessive Compulsive Disorder CaseMarcela CamposNo ratings yet
- Clinicians Guide To AutismDocument20 pagesClinicians Guide To AutismNadia Desanti RachmatikaNo ratings yet
- 12th Congres SRFTTCDocument82 pages12th Congres SRFTTCValentina Anuta100% (1)
- Psychiatric NursingDocument31 pagesPsychiatric NursingSofia LiNo ratings yet
- ppt10 DISSDocument21 pagesppt10 DISSLahn Chen LauganasNo ratings yet
- Concise Guide To Ethics in Mental Health CareDocument379 pagesConcise Guide To Ethics in Mental Health Caresandrogb1977No ratings yet
- Emerging Focal Points in Depression and Anxiety: 22 ECNP Congress, IstanbulDocument92 pagesEmerging Focal Points in Depression and Anxiety: 22 ECNP Congress, Istanbuldorina.amaliaNo ratings yet
- Quiz (Perfect)Document3 pagesQuiz (Perfect)kuro hanabusaNo ratings yet
- Depression Supporting Students at School PDFDocument3 pagesDepression Supporting Students at School PDFMrié ChrsNo ratings yet
- Josephs 2006Document15 pagesJosephs 2006gvalcoNo ratings yet
- BP6 15depression PDFDocument75 pagesBP6 15depression PDFada ramosNo ratings yet
- Case 3Document3 pagesCase 3Nur AzizaNo ratings yet
- An Introduction To EFTDocument25 pagesAn Introduction To EFTdiplomat0No ratings yet
- Depression and Anxiety Disorders: Benefits of Exercise, Yoga, and MeditationDocument8 pagesDepression and Anxiety Disorders: Benefits of Exercise, Yoga, and MeditationRobiantiNo ratings yet
- Complementary Therapies in NursingDocument12 pagesComplementary Therapies in NursingHamza Ishtiaq100% (1)
- DR Russ Harris - A Non-Technical Overview of ACTDocument7 pagesDR Russ Harris - A Non-Technical Overview of ACTtoftb750% (2)