
Clinical Anatomy of The Digestive System: Dr. Badru Ssekitooleko
Clinical Anatomy of The Digestive System: Dr. Badru Ssekitooleko
You might also like
- Anterior Cruciate Ligament InjuryDocument20 pagesAnterior Cruciate Ligament Injurymnunezh2304No ratings yet
- Venous Thromboembolism (Pe and DVT)Document31 pagesVenous Thromboembolism (Pe and DVT)NinaNo ratings yet
- Comparison of Owen's Two Poems The Letter and ConsciousDocument3 pagesComparison of Owen's Two Poems The Letter and Consciousbluebeary1230% (1)
- Questions Final EmsDocument14 pagesQuestions Final EmsSabeer MohamedNo ratings yet
- Ansi 535.4-1998Document8 pagesAnsi 535.4-1998Sirous EghlimiNo ratings yet
- GIT Applied AnatomyDocument62 pagesGIT Applied Anatomyueumana0% (1)
- Referat PeritonitisDocument18 pagesReferat PeritonitisWilliam Grandinata Soeseno100% (2)
- Stomach: Arterial and Venous Blood SupplyDocument10 pagesStomach: Arterial and Venous Blood SupplyBereket temesgenNo ratings yet
- Ana SGD 15Document67 pagesAna SGD 15Bea ManzanoNo ratings yet
- Screenshot 2023-11-26 at 5.15.31 PMDocument39 pagesScreenshot 2023-11-26 at 5.15.31 PMgauravsingh708284No ratings yet
- SURGERY - 1.5 Colon, Rectum, and Anus (Lecture)Document8 pagesSURGERY - 1.5 Colon, Rectum, and Anus (Lecture)Bianca Jane Maaliw100% (1)
- Anatomy and Physiology of Git System (Gastroinstestinal Tract)Document37 pagesAnatomy and Physiology of Git System (Gastroinstestinal Tract)Nishi RuciNo ratings yet
- Abdo. VisceraDocument123 pagesAbdo. VisceraDureti DuretiNo ratings yet
- Curs 4 Gastro IDocument23 pagesCurs 4 Gastro In bNo ratings yet
- 2.3.1 Upper Gastro-Oesophageal SurgeryDocument14 pages2.3.1 Upper Gastro-Oesophageal SurgeryZayan SyedNo ratings yet
- Abdomen and Pelvis Pearl Points by Medicose Fever TeamDocument9 pagesAbdomen and Pelvis Pearl Points by Medicose Fever TeamAurang ZaibNo ratings yet
- 1 Gastric and Duodenal Peptic Ulcer Disease 1Document30 pages1 Gastric and Duodenal Peptic Ulcer Disease 1rayNo ratings yet
- Anatomy of The Caecum, Appendix and Colon: Basic ScienceDocument4 pagesAnatomy of The Caecum, Appendix and Colon: Basic ScienceMirza RisqaNo ratings yet
- Stomach: DR Kavitha M Kjiar (Savli)Document52 pagesStomach: DR Kavitha M Kjiar (Savli)Dhaval Chauhan0% (1)
- Pemicu 2 GIDocument123 pagesPemicu 2 GIDessy DsyNo ratings yet
- Gastrointestinal Tract EmbroyologyDocument55 pagesGastrointestinal Tract Embroyologywizarddone311No ratings yet
- Small Intestine AnatomyDocument4 pagesSmall Intestine AnatomyMaria Natalie IrwandaNo ratings yet
- Surgical Anatomy of PeritoneumDocument63 pagesSurgical Anatomy of PeritoneumSuvarna RajNo ratings yet
- Anatomy of Abdominal VisceralsDocument189 pagesAnatomy of Abdominal VisceralsademabdellaaleNo ratings yet
- Transhiatal EsophagectomyDocument12 pagesTranshiatal EsophagectomyprofarmahNo ratings yet
- The StomachDocument3 pagesThe StomachSanjay KishoreNo ratings yet
- კუჭი და 12 გოჯაDocument40 pagesკუჭი და 12 გოჯაSASIDHARNo ratings yet
- Peritoneum and Gastro-Intestinal TractDocument108 pagesPeritoneum and Gastro-Intestinal TractKAYISIRE EMERYNo ratings yet
- 1 Abdominal VisceraDocument45 pages1 Abdominal VisceraMero HamedNo ratings yet
- Anatomy of StomachDocument4 pagesAnatomy of StomachIntan Putri Maisarah100% (1)
- Anatomy Atresia, Volvulus, Meckel's Diverticulum: BowelDocument45 pagesAnatomy Atresia, Volvulus, Meckel's Diverticulum: BowelkedokterankeluargaNo ratings yet
- Rectum & Anal CanalDocument14 pagesRectum & Anal CanalLisa DentonNo ratings yet
- 1-Gastric and Duodenal UlcerDocument21 pages1-Gastric and Duodenal UlcerSeceleanu MarianNo ratings yet
- Lecture StomachDocument31 pagesLecture StomachAmaetenNo ratings yet
- Embryology of Digestive System1Document62 pagesEmbryology of Digestive System1Gina AnnisahNo ratings yet
- LO1 Anatomy and Histology of Lower Gi TractDocument180 pagesLO1 Anatomy and Histology of Lower Gi TractIcarus WingsNo ratings yet
- Anatomy of Hepatobiliary SystemDocument54 pagesAnatomy of Hepatobiliary SystemM.GANESHNo ratings yet
- Disorders of EsophagusDocument27 pagesDisorders of EsophagusFranci Kay SichuNo ratings yet
- Embryo Development Ofthe GI SytermDocument11 pagesEmbryo Development Ofthe GI SytermKingNo ratings yet
- Abdominal AnatomyDocument39 pagesAbdominal AnatomyRahul MandhanNo ratings yet
- მსხვილი ნაწლავი 1Document36 pagesმსხვილი ნაწლავი 1Malak A MahadeenNo ratings yet
- Digestive System-1Document19 pagesDigestive System-1asakingofhNo ratings yet
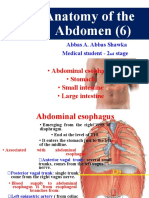
- Anatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineDocument34 pagesAnatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineBilal YimamNo ratings yet
- Development of The Gi SystemDocument6 pagesDevelopment of The Gi SystemKingNo ratings yet
- GI Anatomy Golden!Document39 pagesGI Anatomy Golden!Ayodeji SotimehinNo ratings yet
- Clinical Embriology and Anatomy of Gi Tract Part1Document44 pagesClinical Embriology and Anatomy of Gi Tract Part1trianaamalia100% (1)
- Large Intestine - Structure and FunctionDocument13 pagesLarge Intestine - Structure and FunctiondivyasreekanthanNo ratings yet
- Anatomy and Physiology of Pancreas of Surgical RelevanceDocument96 pagesAnatomy and Physiology of Pancreas of Surgical Relevancechandana pallavaNo ratings yet
- Histology of GITDocument58 pagesHistology of GITOlatomide OlaniranNo ratings yet
- Esophagus AnatomyDocument5 pagesEsophagus AnatomyJinNo ratings yet
- Learning ObjectivesDocument162 pagesLearning ObjectivesNovita IskandarNo ratings yet
- Ac 2Document104 pagesAc 2saide limNo ratings yet
- Overview of Gastrointestinal Tract Perforation 2023Document51 pagesOverview of Gastrointestinal Tract Perforation 2023Ricardo Javier Arreola PeraltaNo ratings yet
- The Small Intestine - Duodenum - Jejunum - Ileum - TeachMeAnatomyDocument4 pagesThe Small Intestine - Duodenum - Jejunum - Ileum - TeachMeAnatomyFelix Oriono100% (1)
- Vago ThomasDocument29 pagesVago ThomasEsti Rahmawati SuryaningrumNo ratings yet
- Mesentric Vascular Disease: Presenter: Vijay N Chairperson: DR Surendra AgarwalDocument74 pagesMesentric Vascular Disease: Presenter: Vijay N Chairperson: DR Surendra AgarwalAnonymous fpRB2h6No ratings yet
- Abdominal Cavity: Prep by Lect: S Hassan AskariDocument38 pagesAbdominal Cavity: Prep by Lect: S Hassan AskariNaveed AfridiNo ratings yet
- Anatomy StomachDocument43 pagesAnatomy StomachBijo K BennyNo ratings yet
- Peritoneum, Peritoneal Cavity, and Diaphragm 11-6-15-1Document67 pagesPeritoneum, Peritoneal Cavity, and Diaphragm 11-6-15-1Deny ShajiniNo ratings yet
- Cirugia Anatomica Del Intestino GruesoDocument3 pagesCirugia Anatomica Del Intestino GruesoWildor Herrera GuevaraNo ratings yet
- The Stomach - Structure - Neurovasculature - TeachMeAnatomyDocument4 pagesThe Stomach - Structure - Neurovasculature - TeachMeAnatomyyamanuel25No ratings yet
- Jejunal and Ileal AtresiasDocument37 pagesJejunal and Ileal AtresiasABDUL RAHIM UMAR FAROUKNo ratings yet
- Blok GastrointestinalDocument103 pagesBlok GastrointestinalArLyne MakinNo ratings yet
- Abdominal VisceraDocument4 pagesAbdominal ViscerazahraaNo ratings yet
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- "Please Do Something For My Period Pain": Max Brinsmead MB Bs PHD May 2015Document18 pages"Please Do Something For My Period Pain": Max Brinsmead MB Bs PHD May 2015NinaNo ratings yet
- Descriptive Epidemiology Study Designs: Zziwa Swaibu (BEH, MPH MUK)Document47 pagesDescriptive Epidemiology Study Designs: Zziwa Swaibu (BEH, MPH MUK)Nina100% (1)
- Newborn Assessment & Care. KabaleDocument41 pagesNewborn Assessment & Care. KabaleNinaNo ratings yet
- Iv Fluids: Beneficial or More Harm?Document20 pagesIv Fluids: Beneficial or More Harm?NinaNo ratings yet
- Palpitations: DR Polamuri Tabitha PG First YrDocument37 pagesPalpitations: DR Polamuri Tabitha PG First YrNinaNo ratings yet
- DR - Chinmoy Saha M.D. (Cardiology) Phase B ResidentDocument32 pagesDR - Chinmoy Saha M.D. (Cardiology) Phase B ResidentNinaNo ratings yet
- Fluid Therapy in Medical Disorders: DR Y RaghunandhiniDocument44 pagesFluid Therapy in Medical Disorders: DR Y RaghunandhiniNinaNo ratings yet
- Family Medicine (Def-Hist)Document22 pagesFamily Medicine (Def-Hist)NinaNo ratings yet
- Sampling Procedures: by Dr. Mina NakawukaDocument44 pagesSampling Procedures: by Dr. Mina NakawukaNinaNo ratings yet
- S.3 C - Part17 PDFDocument1 pageS.3 C - Part17 PDFNinaNo ratings yet
- Applying The Sociological Imagination To Health, Illness, and The BodyDocument5 pagesApplying The Sociological Imagination To Health, Illness, and The BodyNinaNo ratings yet
- Health CareDocument12 pagesHealth CareNinaNo ratings yet
- Heartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaDocument31 pagesHeartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaNinaNo ratings yet
- Cholera and Management of Dehydration: by Yunus Ramadhan Facilitated by DR Kibengo FreddieDocument18 pagesCholera and Management of Dehydration: by Yunus Ramadhan Facilitated by DR Kibengo FreddieNinaNo ratings yet
- Electrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesDocument44 pagesElectrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesNinaNo ratings yet
- Fluids: Presenter: Atwebembere Raymond Faciliitator: Dr. KibengoDocument34 pagesFluids: Presenter: Atwebembere Raymond Faciliitator: Dr. KibengoNinaNo ratings yet
- Introduction To ECG: Presenter: Emiacu Kenneth Facilitator: Dr. Ssebuliba MosesDocument36 pagesIntroduction To ECG: Presenter: Emiacu Kenneth Facilitator: Dr. Ssebuliba MosesNinaNo ratings yet
- Clinical History A Symptom Tailored Approach: Presenter: Walter Karim L .MBCHB V Facilitator:Dr. Damani AliDocument15 pagesClinical History A Symptom Tailored Approach: Presenter: Walter Karim L .MBCHB V Facilitator:Dr. Damani AliNinaNo ratings yet
- Thyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoDocument35 pagesThyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoNinaNo ratings yet
- Tetanus: Presenter:Walter K Facilitator: DR - DamaniDocument21 pagesTetanus: Presenter:Walter K Facilitator: DR - DamaniNinaNo ratings yet
- Acromegaly: Atwebembere Raymond 214-083011-07132 Dr. Ssebuliba MosesDocument32 pagesAcromegaly: Atwebembere Raymond 214-083011-07132 Dr. Ssebuliba MosesNinaNo ratings yet
- Splenomegaly and White Cell Abnormalities: Benjamin Kizito Birungi Facilitator: Dr. Ssebuliba MosesDocument58 pagesSplenomegaly and White Cell Abnormalities: Benjamin Kizito Birungi Facilitator: Dr. Ssebuliba MosesNinaNo ratings yet
- Splints and Tractions in OrthopaedicsDocument56 pagesSplints and Tractions in OrthopaedicsNinaNo ratings yet
- Management of Epilepsy: by Ejuu Seth MBCHB - 5 Facilitated by Dr. Daman AliDocument42 pagesManagement of Epilepsy: by Ejuu Seth MBCHB - 5 Facilitated by Dr. Daman AliNinaNo ratings yet
- Palpitations AND Heartbeat Disorders: By: Aisha Sara Tasnim Physician: DR SsebulibaDocument22 pagesPalpitations AND Heartbeat Disorders: By: Aisha Sara Tasnim Physician: DR SsebulibaNinaNo ratings yet
- Comatose PTDocument20 pagesComatose PTNinaNo ratings yet
- Diabetes Mellitus Complications: Ssenabulya F Ronny MBCHB V Moderator Dr. Mutebi 4B Endocrinology UnitDocument55 pagesDiabetes Mellitus Complications: Ssenabulya F Ronny MBCHB V Moderator Dr. Mutebi 4B Endocrinology UnitNinaNo ratings yet
- Permission To Attend Hockey DayDocument4 pagesPermission To Attend Hockey Dayapi-244287783No ratings yet
- Star Wars D20 - Gertie's Form-FillableDocument2 pagesStar Wars D20 - Gertie's Form-FillableArchmageAdbaNo ratings yet
- Musculature and Fascia: Station 1: The Anterior Abdominal WallDocument10 pagesMusculature and Fascia: Station 1: The Anterior Abdominal WallAlia SahniNo ratings yet
- Opioid AnalgesicDocument12 pagesOpioid AnalgesicFaria Islam JuhiNo ratings yet
- Baum LawsuitDocument97 pagesBaum LawsuitCBCSASKNo ratings yet
- Trigonum Coli AnteriorDocument22 pagesTrigonum Coli AnteriorPramudita DinarNo ratings yet
- Anatomi Neurology 2Document22 pagesAnatomi Neurology 2LindaNo ratings yet
- Another First Aid XXXXDocument20 pagesAnother First Aid XXXXQuennie Anne SabaterNo ratings yet
- MecexerciciosDocument14 pagesMecexerciciosJoão PadilhaNo ratings yet
- Abdo Pelvis - Lecture 01 - Anterior Abdominal WallDocument24 pagesAbdo Pelvis - Lecture 01 - Anterior Abdominal Wallsurgery 1No ratings yet
- The Fast Medium Bowler PDFDocument5 pagesThe Fast Medium Bowler PDFramjdNo ratings yet
- Roy of The Rovers - A New Beginning - Week 9Document6 pagesRoy of The Rovers - A New Beginning - Week 9Cyril "Storky" KnightNo ratings yet
- AccidentDocument84 pagesAccidentNaftasica100% (1)
- Anatomy Practical OSPEDocument33 pagesAnatomy Practical OSPEAbdi Ñãśìr Møhàmèď ŚàĺàhNo ratings yet
- Candidate Guide Trauma Case Pelvic TraumaDocument6 pagesCandidate Guide Trauma Case Pelvic Traumadebby nirmasariNo ratings yet
- Athletic Trainer Essay 3Document5 pagesAthletic Trainer Essay 3api-457915016No ratings yet
- JA SampleDocument4 pagesJA SampleJane CANo ratings yet
- English Premier League: 90 Minutes + Injury Time ResultsDocument12 pagesEnglish Premier League: 90 Minutes + Injury Time ResultsAnonymous s7e7aV3BQENo ratings yet
- G-9 MapehDocument4 pagesG-9 MapehHoniel PagoboNo ratings yet
- Traction: Yasmin Samy Fouad Mohammed AttiaDocument20 pagesTraction: Yasmin Samy Fouad Mohammed AttiaAhmad YaseenNo ratings yet
- Gelig Vs People of The Philippines-173150Document1 pageGelig Vs People of The Philippines-173150george almeda100% (1)
- Emergency Response Plan Flow ChartDocument1 pageEmergency Response Plan Flow Charte cubeNo ratings yet
- Carbonate and Fracture ReservoirsDocument8 pagesCarbonate and Fracture ReservoirsAijaz Ali0% (1)
- Epson Projector EB-700U Installation GuideDocument119 pagesEpson Projector EB-700U Installation GuideBhavin MaradiaNo ratings yet
- Anatomy of The Shoulder JointDocument44 pagesAnatomy of The Shoulder JointAuza Moses Ibrahim100% (1)
- Chapter 4 The Law of TortsDocument28 pagesChapter 4 The Law of TortsmaleekahNo ratings yet




















































































































Download as ppt, pdf, or txt
You might also like
- Anterior Cruciate Ligament InjuryDocument20 pagesAnterior Cruciate Ligament Injurymnunezh2304No ratings yet
- Venous Thromboembolism (Pe and DVT)Document31 pagesVenous Thromboembolism (Pe and DVT)NinaNo ratings yet
- Comparison of Owen's Two Poems The Letter and ConsciousDocument3 pagesComparison of Owen's Two Poems The Letter and Consciousbluebeary1230% (1)
- Questions Final EmsDocument14 pagesQuestions Final EmsSabeer MohamedNo ratings yet
- Ansi 535.4-1998Document8 pagesAnsi 535.4-1998Sirous EghlimiNo ratings yet
- GIT Applied AnatomyDocument62 pagesGIT Applied Anatomyueumana0% (1)
- Referat PeritonitisDocument18 pagesReferat PeritonitisWilliam Grandinata Soeseno100% (2)
- Stomach: Arterial and Venous Blood SupplyDocument10 pagesStomach: Arterial and Venous Blood SupplyBereket temesgenNo ratings yet
- Ana SGD 15Document67 pagesAna SGD 15Bea ManzanoNo ratings yet
- Screenshot 2023-11-26 at 5.15.31 PMDocument39 pagesScreenshot 2023-11-26 at 5.15.31 PMgauravsingh708284No ratings yet
- SURGERY - 1.5 Colon, Rectum, and Anus (Lecture)Document8 pagesSURGERY - 1.5 Colon, Rectum, and Anus (Lecture)Bianca Jane Maaliw100% (1)
- Anatomy and Physiology of Git System (Gastroinstestinal Tract)Document37 pagesAnatomy and Physiology of Git System (Gastroinstestinal Tract)Nishi RuciNo ratings yet
- Abdo. VisceraDocument123 pagesAbdo. VisceraDureti DuretiNo ratings yet
- Curs 4 Gastro IDocument23 pagesCurs 4 Gastro In bNo ratings yet
- 2.3.1 Upper Gastro-Oesophageal SurgeryDocument14 pages2.3.1 Upper Gastro-Oesophageal SurgeryZayan SyedNo ratings yet
- Abdomen and Pelvis Pearl Points by Medicose Fever TeamDocument9 pagesAbdomen and Pelvis Pearl Points by Medicose Fever TeamAurang ZaibNo ratings yet
- 1 Gastric and Duodenal Peptic Ulcer Disease 1Document30 pages1 Gastric and Duodenal Peptic Ulcer Disease 1rayNo ratings yet
- Anatomy of The Caecum, Appendix and Colon: Basic ScienceDocument4 pagesAnatomy of The Caecum, Appendix and Colon: Basic ScienceMirza RisqaNo ratings yet
- Stomach: DR Kavitha M Kjiar (Savli)Document52 pagesStomach: DR Kavitha M Kjiar (Savli)Dhaval Chauhan0% (1)
- Pemicu 2 GIDocument123 pagesPemicu 2 GIDessy DsyNo ratings yet
- Gastrointestinal Tract EmbroyologyDocument55 pagesGastrointestinal Tract Embroyologywizarddone311No ratings yet
- Small Intestine AnatomyDocument4 pagesSmall Intestine AnatomyMaria Natalie IrwandaNo ratings yet
- Surgical Anatomy of PeritoneumDocument63 pagesSurgical Anatomy of PeritoneumSuvarna RajNo ratings yet
- Anatomy of Abdominal VisceralsDocument189 pagesAnatomy of Abdominal VisceralsademabdellaaleNo ratings yet
- Transhiatal EsophagectomyDocument12 pagesTranshiatal EsophagectomyprofarmahNo ratings yet
- The StomachDocument3 pagesThe StomachSanjay KishoreNo ratings yet
- კუჭი და 12 გოჯაDocument40 pagesკუჭი და 12 გოჯაSASIDHARNo ratings yet
- Peritoneum and Gastro-Intestinal TractDocument108 pagesPeritoneum and Gastro-Intestinal TractKAYISIRE EMERYNo ratings yet
- 1 Abdominal VisceraDocument45 pages1 Abdominal VisceraMero HamedNo ratings yet
- Anatomy of StomachDocument4 pagesAnatomy of StomachIntan Putri Maisarah100% (1)
- Anatomy Atresia, Volvulus, Meckel's Diverticulum: BowelDocument45 pagesAnatomy Atresia, Volvulus, Meckel's Diverticulum: BowelkedokterankeluargaNo ratings yet
- Rectum & Anal CanalDocument14 pagesRectum & Anal CanalLisa DentonNo ratings yet
- 1-Gastric and Duodenal UlcerDocument21 pages1-Gastric and Duodenal UlcerSeceleanu MarianNo ratings yet
- Lecture StomachDocument31 pagesLecture StomachAmaetenNo ratings yet
- Embryology of Digestive System1Document62 pagesEmbryology of Digestive System1Gina AnnisahNo ratings yet
- LO1 Anatomy and Histology of Lower Gi TractDocument180 pagesLO1 Anatomy and Histology of Lower Gi TractIcarus WingsNo ratings yet
- Anatomy of Hepatobiliary SystemDocument54 pagesAnatomy of Hepatobiliary SystemM.GANESHNo ratings yet
- Disorders of EsophagusDocument27 pagesDisorders of EsophagusFranci Kay SichuNo ratings yet
- Embryo Development Ofthe GI SytermDocument11 pagesEmbryo Development Ofthe GI SytermKingNo ratings yet
- Abdominal AnatomyDocument39 pagesAbdominal AnatomyRahul MandhanNo ratings yet
- მსხვილი ნაწლავი 1Document36 pagesმსხვილი ნაწლავი 1Malak A MahadeenNo ratings yet
- Digestive System-1Document19 pagesDigestive System-1asakingofhNo ratings yet
- Anatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineDocument34 pagesAnatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineBilal YimamNo ratings yet
- Development of The Gi SystemDocument6 pagesDevelopment of The Gi SystemKingNo ratings yet
- GI Anatomy Golden!Document39 pagesGI Anatomy Golden!Ayodeji SotimehinNo ratings yet
- Clinical Embriology and Anatomy of Gi Tract Part1Document44 pagesClinical Embriology and Anatomy of Gi Tract Part1trianaamalia100% (1)
- Large Intestine - Structure and FunctionDocument13 pagesLarge Intestine - Structure and FunctiondivyasreekanthanNo ratings yet
- Anatomy and Physiology of Pancreas of Surgical RelevanceDocument96 pagesAnatomy and Physiology of Pancreas of Surgical Relevancechandana pallavaNo ratings yet
- Histology of GITDocument58 pagesHistology of GITOlatomide OlaniranNo ratings yet
- Esophagus AnatomyDocument5 pagesEsophagus AnatomyJinNo ratings yet
- Learning ObjectivesDocument162 pagesLearning ObjectivesNovita IskandarNo ratings yet
- Ac 2Document104 pagesAc 2saide limNo ratings yet
- Overview of Gastrointestinal Tract Perforation 2023Document51 pagesOverview of Gastrointestinal Tract Perforation 2023Ricardo Javier Arreola PeraltaNo ratings yet
- The Small Intestine - Duodenum - Jejunum - Ileum - TeachMeAnatomyDocument4 pagesThe Small Intestine - Duodenum - Jejunum - Ileum - TeachMeAnatomyFelix Oriono100% (1)
- Vago ThomasDocument29 pagesVago ThomasEsti Rahmawati SuryaningrumNo ratings yet
- Mesentric Vascular Disease: Presenter: Vijay N Chairperson: DR Surendra AgarwalDocument74 pagesMesentric Vascular Disease: Presenter: Vijay N Chairperson: DR Surendra AgarwalAnonymous fpRB2h6No ratings yet
- Abdominal Cavity: Prep by Lect: S Hassan AskariDocument38 pagesAbdominal Cavity: Prep by Lect: S Hassan AskariNaveed AfridiNo ratings yet
- Anatomy StomachDocument43 pagesAnatomy StomachBijo K BennyNo ratings yet
- Peritoneum, Peritoneal Cavity, and Diaphragm 11-6-15-1Document67 pagesPeritoneum, Peritoneal Cavity, and Diaphragm 11-6-15-1Deny ShajiniNo ratings yet
- Cirugia Anatomica Del Intestino GruesoDocument3 pagesCirugia Anatomica Del Intestino GruesoWildor Herrera GuevaraNo ratings yet
- The Stomach - Structure - Neurovasculature - TeachMeAnatomyDocument4 pagesThe Stomach - Structure - Neurovasculature - TeachMeAnatomyyamanuel25No ratings yet
- Jejunal and Ileal AtresiasDocument37 pagesJejunal and Ileal AtresiasABDUL RAHIM UMAR FAROUKNo ratings yet
- Blok GastrointestinalDocument103 pagesBlok GastrointestinalArLyne MakinNo ratings yet
- Abdominal VisceraDocument4 pagesAbdominal ViscerazahraaNo ratings yet
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- "Please Do Something For My Period Pain": Max Brinsmead MB Bs PHD May 2015Document18 pages"Please Do Something For My Period Pain": Max Brinsmead MB Bs PHD May 2015NinaNo ratings yet
- Descriptive Epidemiology Study Designs: Zziwa Swaibu (BEH, MPH MUK)Document47 pagesDescriptive Epidemiology Study Designs: Zziwa Swaibu (BEH, MPH MUK)Nina100% (1)
- Newborn Assessment & Care. KabaleDocument41 pagesNewborn Assessment & Care. KabaleNinaNo ratings yet
- Iv Fluids: Beneficial or More Harm?Document20 pagesIv Fluids: Beneficial or More Harm?NinaNo ratings yet
- Palpitations: DR Polamuri Tabitha PG First YrDocument37 pagesPalpitations: DR Polamuri Tabitha PG First YrNinaNo ratings yet
- DR - Chinmoy Saha M.D. (Cardiology) Phase B ResidentDocument32 pagesDR - Chinmoy Saha M.D. (Cardiology) Phase B ResidentNinaNo ratings yet
- Fluid Therapy in Medical Disorders: DR Y RaghunandhiniDocument44 pagesFluid Therapy in Medical Disorders: DR Y RaghunandhiniNinaNo ratings yet
- Family Medicine (Def-Hist)Document22 pagesFamily Medicine (Def-Hist)NinaNo ratings yet
- Sampling Procedures: by Dr. Mina NakawukaDocument44 pagesSampling Procedures: by Dr. Mina NakawukaNinaNo ratings yet
- S.3 C - Part17 PDFDocument1 pageS.3 C - Part17 PDFNinaNo ratings yet
- Applying The Sociological Imagination To Health, Illness, and The BodyDocument5 pagesApplying The Sociological Imagination To Health, Illness, and The BodyNinaNo ratings yet
- Health CareDocument12 pagesHealth CareNinaNo ratings yet
- Heartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaDocument31 pagesHeartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaNinaNo ratings yet
- Cholera and Management of Dehydration: by Yunus Ramadhan Facilitated by DR Kibengo FreddieDocument18 pagesCholera and Management of Dehydration: by Yunus Ramadhan Facilitated by DR Kibengo FreddieNinaNo ratings yet
- Electrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesDocument44 pagesElectrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesNinaNo ratings yet
- Fluids: Presenter: Atwebembere Raymond Faciliitator: Dr. KibengoDocument34 pagesFluids: Presenter: Atwebembere Raymond Faciliitator: Dr. KibengoNinaNo ratings yet
- Introduction To ECG: Presenter: Emiacu Kenneth Facilitator: Dr. Ssebuliba MosesDocument36 pagesIntroduction To ECG: Presenter: Emiacu Kenneth Facilitator: Dr. Ssebuliba MosesNinaNo ratings yet
- Clinical History A Symptom Tailored Approach: Presenter: Walter Karim L .MBCHB V Facilitator:Dr. Damani AliDocument15 pagesClinical History A Symptom Tailored Approach: Presenter: Walter Karim L .MBCHB V Facilitator:Dr. Damani AliNinaNo ratings yet
- Thyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoDocument35 pagesThyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoNinaNo ratings yet
- Tetanus: Presenter:Walter K Facilitator: DR - DamaniDocument21 pagesTetanus: Presenter:Walter K Facilitator: DR - DamaniNinaNo ratings yet
- Acromegaly: Atwebembere Raymond 214-083011-07132 Dr. Ssebuliba MosesDocument32 pagesAcromegaly: Atwebembere Raymond 214-083011-07132 Dr. Ssebuliba MosesNinaNo ratings yet
- Splenomegaly and White Cell Abnormalities: Benjamin Kizito Birungi Facilitator: Dr. Ssebuliba MosesDocument58 pagesSplenomegaly and White Cell Abnormalities: Benjamin Kizito Birungi Facilitator: Dr. Ssebuliba MosesNinaNo ratings yet
- Splints and Tractions in OrthopaedicsDocument56 pagesSplints and Tractions in OrthopaedicsNinaNo ratings yet
- Management of Epilepsy: by Ejuu Seth MBCHB - 5 Facilitated by Dr. Daman AliDocument42 pagesManagement of Epilepsy: by Ejuu Seth MBCHB - 5 Facilitated by Dr. Daman AliNinaNo ratings yet
- Palpitations AND Heartbeat Disorders: By: Aisha Sara Tasnim Physician: DR SsebulibaDocument22 pagesPalpitations AND Heartbeat Disorders: By: Aisha Sara Tasnim Physician: DR SsebulibaNinaNo ratings yet
- Comatose PTDocument20 pagesComatose PTNinaNo ratings yet
- Diabetes Mellitus Complications: Ssenabulya F Ronny MBCHB V Moderator Dr. Mutebi 4B Endocrinology UnitDocument55 pagesDiabetes Mellitus Complications: Ssenabulya F Ronny MBCHB V Moderator Dr. Mutebi 4B Endocrinology UnitNinaNo ratings yet
- Permission To Attend Hockey DayDocument4 pagesPermission To Attend Hockey Dayapi-244287783No ratings yet
- Star Wars D20 - Gertie's Form-FillableDocument2 pagesStar Wars D20 - Gertie's Form-FillableArchmageAdbaNo ratings yet
- Musculature and Fascia: Station 1: The Anterior Abdominal WallDocument10 pagesMusculature and Fascia: Station 1: The Anterior Abdominal WallAlia SahniNo ratings yet
- Opioid AnalgesicDocument12 pagesOpioid AnalgesicFaria Islam JuhiNo ratings yet
- Baum LawsuitDocument97 pagesBaum LawsuitCBCSASKNo ratings yet
- Trigonum Coli AnteriorDocument22 pagesTrigonum Coli AnteriorPramudita DinarNo ratings yet
- Anatomi Neurology 2Document22 pagesAnatomi Neurology 2LindaNo ratings yet
- Another First Aid XXXXDocument20 pagesAnother First Aid XXXXQuennie Anne SabaterNo ratings yet
- MecexerciciosDocument14 pagesMecexerciciosJoão PadilhaNo ratings yet
- Abdo Pelvis - Lecture 01 - Anterior Abdominal WallDocument24 pagesAbdo Pelvis - Lecture 01 - Anterior Abdominal Wallsurgery 1No ratings yet
- The Fast Medium Bowler PDFDocument5 pagesThe Fast Medium Bowler PDFramjdNo ratings yet
- Roy of The Rovers - A New Beginning - Week 9Document6 pagesRoy of The Rovers - A New Beginning - Week 9Cyril "Storky" KnightNo ratings yet
- AccidentDocument84 pagesAccidentNaftasica100% (1)
- Anatomy Practical OSPEDocument33 pagesAnatomy Practical OSPEAbdi Ñãśìr Møhàmèď ŚàĺàhNo ratings yet
- Candidate Guide Trauma Case Pelvic TraumaDocument6 pagesCandidate Guide Trauma Case Pelvic Traumadebby nirmasariNo ratings yet
- Athletic Trainer Essay 3Document5 pagesAthletic Trainer Essay 3api-457915016No ratings yet
- JA SampleDocument4 pagesJA SampleJane CANo ratings yet
- English Premier League: 90 Minutes + Injury Time ResultsDocument12 pagesEnglish Premier League: 90 Minutes + Injury Time ResultsAnonymous s7e7aV3BQENo ratings yet
- G-9 MapehDocument4 pagesG-9 MapehHoniel PagoboNo ratings yet
- Traction: Yasmin Samy Fouad Mohammed AttiaDocument20 pagesTraction: Yasmin Samy Fouad Mohammed AttiaAhmad YaseenNo ratings yet
- Gelig Vs People of The Philippines-173150Document1 pageGelig Vs People of The Philippines-173150george almeda100% (1)
- Emergency Response Plan Flow ChartDocument1 pageEmergency Response Plan Flow Charte cubeNo ratings yet
- Carbonate and Fracture ReservoirsDocument8 pagesCarbonate and Fracture ReservoirsAijaz Ali0% (1)
- Epson Projector EB-700U Installation GuideDocument119 pagesEpson Projector EB-700U Installation GuideBhavin MaradiaNo ratings yet
- Anatomy of The Shoulder JointDocument44 pagesAnatomy of The Shoulder JointAuza Moses Ibrahim100% (1)
- Chapter 4 The Law of TortsDocument28 pagesChapter 4 The Law of TortsmaleekahNo ratings yet