Download as ppt, pdf, or txt
You might also like
- Autism For DummiesDocument11 pagesAutism For Dummiesgocyndigo72yahoocomNo ratings yet
- The Battle Against Covid-19 Filipino American Healthcare Workers on the Frontlines of the Pandemic ResponseFrom EverandThe Battle Against Covid-19 Filipino American Healthcare Workers on the Frontlines of the Pandemic ResponseNo ratings yet
- Essay Example 1 - DementiaDocument7 pagesEssay Example 1 - DementiaMarzio FagioliNo ratings yet
- Recovery High Schools in Massachusetts: A Promising, Comprehensive Model For Adolescent Substance Abuse and DependenceDocument44 pagesRecovery High Schools in Massachusetts: A Promising, Comprehensive Model For Adolescent Substance Abuse and DependenceThe Stacie Mathewson FoundationNo ratings yet
- Know Your Soil PDFDocument20 pagesKnow Your Soil PDFbpcdivNo ratings yet
- Healthcare FinancingDocument4 pagesHealthcare Financingabas ibrahimNo ratings yet
- Health System Model of VietnamDocument20 pagesHealth System Model of Vietnamsneha khuranaNo ratings yet
- Dr. Padma Bhatia: Assistant Professor Department of Community Medicine G.M.C., Bhopal. M.P. IndiaDocument30 pagesDr. Padma Bhatia: Assistant Professor Department of Community Medicine G.M.C., Bhopal. M.P. IndiaSakshi SuriNo ratings yet
- health care system of swedenبDocument34 pageshealth care system of swedenبAhmedAljebouli0% (1)
- Tools of Health Economics PDFDocument53 pagesTools of Health Economics PDFAdnan RahatNo ratings yet
- HygieneDocument204 pagesHygieneMary SericNo ratings yet
- Chapter 16Document5 pagesChapter 16Pranay PandeyNo ratings yet
- Influenza Health Promotion ProjectDocument8 pagesInfluenza Health Promotion Projectapi-284269118No ratings yet
- Health InsuranceDocument36 pagesHealth Insurancevijaya lakshmi100% (2)
- Research Thesis FinalDocument22 pagesResearch Thesis Finalsurendra100% (3)
- Health Systems Strengthening - The University of MelbourneDocument14 pagesHealth Systems Strengthening - The University of MelbourneEstefanía MariñoNo ratings yet
- Health EducationDocument27 pagesHealth EducationTsi Koy Love HurtsNo ratings yet
- CMN 463 Lecture 2 Insurance Medicare and MedicaidDocument18 pagesCMN 463 Lecture 2 Insurance Medicare and MedicaidCarlos GuiterizNo ratings yet
- Health Indicators: Dr. Ali Nasre AlamDocument37 pagesHealth Indicators: Dr. Ali Nasre AlamShimmering MoonNo ratings yet
- Health PromotionDocument4 pagesHealth PromotionJithendra KumarNo ratings yet
- 5 Disease Transmission and Outbreak Investigation - 1Document10 pages5 Disease Transmission and Outbreak Investigation - 1RoniAnasoka100% (1)
- Health Insurance HandbookDocument10 pagesHealth Insurance HandbookvinaysekharNo ratings yet
- 5 Do We Need Economics in MedicineDocument24 pages5 Do We Need Economics in MedicineHanan AhmedNo ratings yet
- CHN 1 Topic 1 HandoutsDocument26 pagesCHN 1 Topic 1 Handoutsfleur harrisonNo ratings yet
- My PresentationDocument14 pagesMy PresentationnamithaNo ratings yet
- Report On Health Insurance 2Document23 pagesReport On Health Insurance 2DrJaideep KumarNo ratings yet
- Community Mobilisation and Participation in HealthDocument33 pagesCommunity Mobilisation and Participation in HealthMayom MabuongNo ratings yet
- Financial Products AssignmentDocument14 pagesFinancial Products AssignmentHimanshuNo ratings yet
- Health Promotion Plan PresentationDocument5 pagesHealth Promotion Plan PresentationGeorge KavuviNo ratings yet
- Health EconomicsDocument227 pagesHealth EconomicsagezeNo ratings yet
- Lesson 1 - Introduction To Disease Control NewDocument21 pagesLesson 1 - Introduction To Disease Control NewValopinho 5No ratings yet
- Health IndicatorDocument30 pagesHealth IndicatorPawan KumarNo ratings yet
- Long Term CareDocument24 pagesLong Term CareOlawale JohnsonNo ratings yet
- A Quick Overview of Your Proposal: This Answer Is Limited To 1000 Characters, or About 100 Words. Characters LeftDocument13 pagesA Quick Overview of Your Proposal: This Answer Is Limited To 1000 Characters, or About 100 Words. Characters LeftaracaunaNo ratings yet
- National Guidelines For Management of Covid-19Document203 pagesNational Guidelines For Management of Covid-19African Centre for Media ExcellenceNo ratings yet
- History of Abortion: BortionDocument7 pagesHistory of Abortion: Bortion'Riya ShingwaNo ratings yet
- Adolescent Pregnancy Prevention Program: Click HereDocument16 pagesAdolescent Pregnancy Prevention Program: Click HereMacy Wu100% (1)
- 3 Puntland Health Policy FrameworkDocument46 pages3 Puntland Health Policy Frameworkkunciil100% (1)
- Scope of NursingDocument27 pagesScope of NursingBlanche Gonzalez100% (2)
- Clinical Area Objective Headnursing Activities Students Activities EvaluationDocument2 pagesClinical Area Objective Headnursing Activities Students Activities EvaluationTrixie Anne GamotinNo ratings yet
- Nhs/Local Government Joint Working: Briefing PaperDocument7 pagesNhs/Local Government Joint Working: Briefing PaperSandeepkumar ChennuNo ratings yet
- Community AssessmentDocument9 pagesCommunity Assessmentرانيا احمد عبد الكريمNo ratings yet
- Health Insurance: Passed By: Rhea May PoriloDocument12 pagesHealth Insurance: Passed By: Rhea May PoriloRhea May PoriloNo ratings yet
- BeneficenceDocument3 pagesBeneficenceAngelique Jade EnriquezNo ratings yet
- Quality Improvement PaperDocument8 pagesQuality Improvement Paperapi-401406690No ratings yet
- Chronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesFrom EverandChronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesNo ratings yet
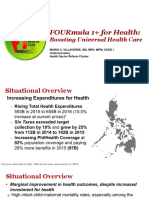
- 4 FOURmula 1 For Health Boosting Universal Health Care by DR Beverly HoDocument12 pages4 FOURmula 1 For Health Boosting Universal Health Care by DR Beverly HoJanella DandanNo ratings yet
- Genomics and Nursing PracticeDocument7 pagesGenomics and Nursing Practicebernadette_olaveNo ratings yet
- Running Head: Human Immunodeficiency Virus (Hiv)Document10 pagesRunning Head: Human Immunodeficiency Virus (Hiv)Alisha SharanNo ratings yet
- An Exploration of School Nurse Role in Secondary Girls Schools in BahrainDocument6 pagesAn Exploration of School Nurse Role in Secondary Girls Schools in BahrainGlobal Research and Development Services100% (1)
- Discussion 6 AnswerDocument2 pagesDiscussion 6 AnsweranushavergheseNo ratings yet
- Ethical DilemaDocument9 pagesEthical Dilemadavid proctorNo ratings yet
- Health InsuranceDocument28 pagesHealth InsuranceVikramaditya MuralidharanNo ratings yet
- HiAP PowerpointDocument21 pagesHiAP Powerpointjaypee pengNo ratings yet
- Dynamics of Disease TransmissionDocument30 pagesDynamics of Disease TransmissionSyed Sanan shahNo ratings yet
- Department of Health Departmental Report 2008Document253 pagesDepartment of Health Departmental Report 2008Bren-RNo ratings yet
- Dsunzh Ekè Fed F'K (KK CKKSMZ: F'K (KK Lnu) 17) Bulfvv W'Kuy (Ks K) JKMT, Osu Q) Fnyyh&110002Document8 pagesDsunzh Ekè Fed F'K (KK CKKSMZ: F'K (KK Lnu) 17) Bulfvv W'Kuy (Ks K) JKMT, Osu Q) Fnyyh&110002Tanvi Tanya100% (1)
- 2 Epidemiology TerminologyDocument33 pages2 Epidemiology Terminologynithin shenoiNo ratings yet
- Rehabilitation Nursing: Dr. Rohit, MBBS, DNB Physical Medicine and RehabilitationDocument21 pagesRehabilitation Nursing: Dr. Rohit, MBBS, DNB Physical Medicine and RehabilitationRupali RautNo ratings yet
- 6-Global Health and Globalization and Public HealthDocument67 pages6-Global Health and Globalization and Public HealthMoreiyamNo ratings yet
- 2019 NCC Npsgs FinalDocument1 page2019 NCC Npsgs FinalJaic Ealston D. TampusNo ratings yet
- Community Health A Complete Guide - 2020 EditionFrom EverandCommunity Health A Complete Guide - 2020 EditionRating: 5 out of 5 stars5/5 (1)
- 5 1 Why Your Body Needs NutrientsDocument3 pages5 1 Why Your Body Needs Nutrientsapi-261782961No ratings yet
- Post Partum Psychosis Nursing Diagnosis: Aurelio, Lyca Mae MDocument3 pagesPost Partum Psychosis Nursing Diagnosis: Aurelio, Lyca Mae MLyca Mae AurelioNo ratings yet
- Rose Doe v. The City of New York, Et. Al.Document57 pagesRose Doe v. The City of New York, Et. Al.Daily Caller News FoundationNo ratings yet
- Isolated Third Nerve PalsyDocument4 pagesIsolated Third Nerve PalsySora KerovaNo ratings yet
- NewDocument17 pagesNewMadhu BalaNo ratings yet
- Individual Performance Commitment and Review (Ipcr) : Name of Employee: Approved By: Date Date FiledDocument12 pagesIndividual Performance Commitment and Review (Ipcr) : Name of Employee: Approved By: Date Date FiledTiffanny Diane Agbayani RuedasNo ratings yet
- Which of The Following Is NOT True About Dust?Document3 pagesWhich of The Following Is NOT True About Dust?lucel palaca100% (1)
- Firefly Prime Mobile AppDocument7 pagesFirefly Prime Mobile Appmukh bhaNo ratings yet
- Molly McDowell - Course Project Part 1Document5 pagesMolly McDowell - Course Project Part 1Adelaide DariaNo ratings yet
- The Effects of Trauma and How To Deal With It Jim BanksDocument5 pagesThe Effects of Trauma and How To Deal With It Jim Banks2bug2me2not2No ratings yet
- Lab Report For ParacetamolDocument5 pagesLab Report For Paracetamol9gcfz8zf9xNo ratings yet
- HPLC Article - 1Document8 pagesHPLC Article - 1akkimipadmaNo ratings yet
- Mt. Olive - August 2012-FINALDocument52 pagesMt. Olive - August 2012-FINALjoe9783No ratings yet
- Phenotypic and Molecular Characterizations OF: Salmonella Species in EthiopiaDocument194 pagesPhenotypic and Molecular Characterizations OF: Salmonella Species in EthiopiaAmid CapmariNo ratings yet
- Adolescence and Preg Position PaperDocument2 pagesAdolescence and Preg Position PaperNichole Trisha MontalbaNo ratings yet
- Chapter 21 Muscle Blood FlowDocument17 pagesChapter 21 Muscle Blood Flowelmedina omeragicNo ratings yet
- Illustrative Teaching Case: Cerebral Fat EmbolismDocument3 pagesIllustrative Teaching Case: Cerebral Fat Embolismandy wookNo ratings yet
- CSQ Nap4 FullDocument219 pagesCSQ Nap4 FullJeisson FarroNo ratings yet
- Kit For Human Thyroid Stimulating Hormone (HTSH) : Irmak-9Document2 pagesKit For Human Thyroid Stimulating Hormone (HTSH) : Irmak-9micky mouseNo ratings yet
- Rabbit KeepingDocument12 pagesRabbit KeepingMoses NdwaruNo ratings yet
- Closed PTW AuditDocument1 pageClosed PTW Auditf.BNo ratings yet
- 12.2 - Regulation of Body TemperatureDocument38 pages12.2 - Regulation of Body Temperature022797SemelllNo ratings yet
- MCQ in OphthalmologyDocument108 pagesMCQ in OphthalmologySushi HtetNo ratings yet
- Language Disorders - 5Document27 pagesLanguage Disorders - 5Marta Sampedro GonzalezNo ratings yet
- Chun-Hung Chen Kun-Cheng ChouDocument38 pagesChun-Hung Chen Kun-Cheng ChoutwnationNo ratings yet
- Case Study 8 Construction SafetyDocument2 pagesCase Study 8 Construction SafetyJerome BricenioNo ratings yet
- Diet For Patient With Parkinson's DiseaseDocument2 pagesDiet For Patient With Parkinson's DiseaseNuzulina SafiraNo ratings yet
- EthicsDocument10 pagesEthicsMadhubala JNo ratings yet