
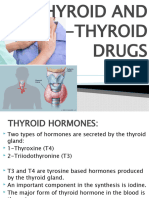
Thyroid & Antithyroid Drugs
Thyroid & Antithyroid Drugs
You might also like
- Clinical Chemistry 3: EndocrinologyDocument21 pagesClinical Chemistry 3: EndocrinologyRomie Solacito100% (3)
- Pharmacology 4th Semester BSN Notes, Educational PlatformDocument985 pagesPharmacology 4th Semester BSN Notes, Educational PlatformPen N PapersNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (3)
- Route of AdministrationDocument48 pagesRoute of AdministrationFranchesca LugoNo ratings yet
- Endocrine DisordersDocument77 pagesEndocrine Disordersahmad100% (2)
- Endocrine Vety PharmaDocument16 pagesEndocrine Vety PharmaSunilNo ratings yet
- Endocrine System 2016Document58 pagesEndocrine System 2016museayana5271No ratings yet
- Insulin and Oral Hypoglycemic AgentsDocument27 pagesInsulin and Oral Hypoglycemic Agentsapi-19916399100% (1)
- Anti AsthmaDocument34 pagesAnti AsthmaDRx Raju ChandranNo ratings yet
- Endocrine Drug: T4 Is Secreted in Excess To T3Document10 pagesEndocrine Drug: T4 Is Secreted in Excess To T3emmanuelNo ratings yet
- Module 3.4 - EndocrineDocument5 pagesModule 3.4 - EndocrineCatherine Sinen ObinqueNo ratings yet
- Endocrine Pharmacology by DR - Mayur SaytaDocument27 pagesEndocrine Pharmacology by DR - Mayur Saytasahilthakker2012No ratings yet
- Lecture16 Anti Diabetic DrugsDocument61 pagesLecture16 Anti Diabetic Drugsharis.18No ratings yet
- Management and Medications in Thyroid Strom and Myxoedema ComaDocument41 pagesManagement and Medications in Thyroid Strom and Myxoedema ComaBhavesh kunvarNo ratings yet
- Shaina Dionisia Palacol Candice Guillermo Gelzan RoldanDocument55 pagesShaina Dionisia Palacol Candice Guillermo Gelzan RoldanEdelrose LapitanNo ratings yet
- Ch-10 Endocrine PharmacologyDocument16 pagesCh-10 Endocrine PharmacologyAyro Business CenterNo ratings yet
- Thyroid CrisisDocument34 pagesThyroid CrisisRidyah Ning TyasNo ratings yet
- All Endocrine PharmacologyDocument143 pagesAll Endocrine PharmacologyabenezergebrekirstosNo ratings yet
- Antidiabetic Drugs. Nurse 2024Document32 pagesAntidiabetic Drugs. Nurse 2024Ayro Business CenterNo ratings yet
- Pharmacology Volume 1 Unit 6 EndocrineDocument76 pagesPharmacology Volume 1 Unit 6 EndocrineAkhilesh TiwariNo ratings yet
- The Thyroid Gland PRINT 2021Document9 pagesThe Thyroid Gland PRINT 2021abcde990075No ratings yet
- 05 Chapter Endrocrine SystemDocument40 pages05 Chapter Endrocrine SystemMSKCNo ratings yet
- Pharmacology LectureDocument5 pagesPharmacology LectureAbdullahayad farouqNo ratings yet
- Insulin and Oral HypoglycemicsDocument38 pagesInsulin and Oral HypoglycemicsEdwin GithogeNo ratings yet
- Pancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyDocument69 pagesPancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyRalf EmoteroNo ratings yet
- Seminar 6 - Psychopharmacology - EctDocument108 pagesSeminar 6 - Psychopharmacology - EctA. TivieanNo ratings yet
- Antidiabetic Drugs. 12 May Modified 2016 of 2015 - 2017 11 17 MayDocument54 pagesAntidiabetic Drugs. 12 May Modified 2016 of 2015 - 2017 11 17 Mayblue sapphireNo ratings yet
- Thyroid & Antithyroid Drugs - 2020Document7 pagesThyroid & Antithyroid Drugs - 2020ireneNo ratings yet
- Thyroid DrugsDocument6 pagesThyroid DrugsThe Real UploaderNo ratings yet
- Lecture 9 Endocrine HormonesDocument18 pagesLecture 9 Endocrine HormonesKC PalattaoNo ratings yet
- FO-Antidiabetic-27042020-Blok 7Document64 pagesFO-Antidiabetic-27042020-Blok 7Indah NurhalizaNo ratings yet
- لقطة شاشة ٢٠٢١-٠٢-٠٥ في ١.٤٦.٥٧ مDocument2 pagesلقطة شاشة ٢٠٢١-٠٢-٠٥ في ١.٤٦.٥٧ مDr. Emad Elbadawy د عماد البدويNo ratings yet
- Drug Study On Agents Used Thyroid and Glucose MetabolismDocument18 pagesDrug Study On Agents Used Thyroid and Glucose Metabolismaeliusz19No ratings yet
- Thyroid and Antithyroid DrugsDocument38 pagesThyroid and Antithyroid DrugsbrkbsnNo ratings yet
- What Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsDocument9 pagesWhat Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsIshaani GargNo ratings yet
- Chapter 34 Insulin & Oral Antidiabetic DrugsDocument24 pagesChapter 34 Insulin & Oral Antidiabetic DrugsIlham RamadhanNo ratings yet
- Immunosuppressants NotesDocument20 pagesImmunosuppressants NotesmadcalNo ratings yet
- Pituitary &thyroid NotesDocument7 pagesPituitary &thyroid NotesAli salimNo ratings yet
- Endocrine PharmacologyDocument42 pagesEndocrine PharmacologyAhmed El SharkawyNo ratings yet
- Disease Spotlight: Diabetes Mellitus: Insulin Insulin Is A Drug That Is Used To ControlDocument7 pagesDisease Spotlight: Diabetes Mellitus: Insulin Insulin Is A Drug That Is Used To ControlMIR SARTAJNo ratings yet
- 11 - Drugs For Thyroid Problems2Document51 pages11 - Drugs For Thyroid Problems2nica velanoNo ratings yet
- Diabetes Mellitus-1 3Document18 pagesDiabetes Mellitus-1 3Narmeen RahimNo ratings yet
- 10 Endocrine PharmacologyDocument34 pages10 Endocrine PharmacologyNaol TolchaNo ratings yet
- I. Title: Drugs Affecting The Endocrine System Ii. ReferencesDocument14 pagesI. Title: Drugs Affecting The Endocrine System Ii. ReferencesGenierose YantoNo ratings yet
- Clinical Pharmacy Chapter Seven Thyroid Disorders: Rowa' Al-RamahiDocument16 pagesClinical Pharmacy Chapter Seven Thyroid Disorders: Rowa' Al-Ramahiabdelrhman aboodaNo ratings yet
- Antidiabetic HerbsDocument21 pagesAntidiabetic HerbsUsamaNo ratings yet
- Unit 1 Antidiabetic Drugs Pharmacy-IIDocument69 pagesUnit 1 Antidiabetic Drugs Pharmacy-IIAsad MirajNo ratings yet
- Insulin, Oral Hypoglycemic Agents-1Document23 pagesInsulin, Oral Hypoglycemic Agents-1IbrahimNo ratings yet
- M3 - Lesson 1bDocument20 pagesM3 - Lesson 1bLhara MañoNo ratings yet
- Drugs Used To Treat Diabetes - MellitusDocument37 pagesDrugs Used To Treat Diabetes - MellitusjisooNo ratings yet
- An Overview On Tirzepatide, Dual-Targeted Treatment For Diabetes and ObesityDocument6 pagesAn Overview On Tirzepatide, Dual-Targeted Treatment For Diabetes and ObesityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Endocrine DrugsDocument42 pagesEndocrine DrugsSolaNo ratings yet
- Pharmacology ResearchDocument20 pagesPharmacology ResearchaagalhazmiNo ratings yet
- anaes&DMDocument11 pagesanaes&DMMohamed Satti AbdalsadigNo ratings yet
- 14) Drugs For Thyroid DisordersDocument13 pages14) Drugs For Thyroid DisordersLatiNo ratings yet
- Common Anti-Diabetics and AnticoagulantsDocument14 pagesCommon Anti-Diabetics and AnticoagulantsemmanuelmkibuniNo ratings yet
- Pharmacology LectureDocument6 pagesPharmacology LectureAbdullahayad farouqNo ratings yet
- Thyroid Disorders - 2023Document82 pagesThyroid Disorders - 2023JEPHTHAH KWASI DANSONo ratings yet
- AntiDiabetic Drugs 2 BDocument50 pagesAntiDiabetic Drugs 2 BAvinash RajNo ratings yet
- Insulin and Oral AntidiabeticsDocument24 pagesInsulin and Oral AntidiabeticsMirza Shaharyar Baig100% (1)
- Natural Hormones and Their Synthetic Analogues 2. Hormone Like Substances 3. Drugs That Stimulate or Suppress Hormone SecretionDocument6 pagesNatural Hormones and Their Synthetic Analogues 2. Hormone Like Substances 3. Drugs That Stimulate or Suppress Hormone SecretionMarianne CruzNo ratings yet
- THYROIDDocument24 pagesTHYROIDanaya khan StudentNo ratings yet
- 04 Psych Crash CourseDocument33 pages04 Psych Crash CourseFranchesca LugoNo ratings yet
- What Is The Difference Between Sign and Symptom?Document7 pagesWhat Is The Difference Between Sign and Symptom?Franchesca LugoNo ratings yet
- 2018 UPlink NMAT Review Social Science LectureDocument133 pages2018 UPlink NMAT Review Social Science LectureFranchesca LugoNo ratings yet
- C-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Document11 pagesC-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Franchesca LugoNo ratings yet
- Presented By: VIVEK DEVDocument38 pagesPresented By: VIVEK DEVFranchesca LugoNo ratings yet
- Ishac M2 Cardio Antihypertensives 2010Document16 pagesIshac M2 Cardio Antihypertensives 2010Franchesca LugoNo ratings yet
- Chief Pharmacist Supervising PharmacistDocument3 pagesChief Pharmacist Supervising PharmacistFranchesca LugoNo ratings yet
- Name: Sex: Age:: Waist Hip RatioDocument2 pagesName: Sex: Age:: Waist Hip RatioFranchesca LugoNo ratings yet
- Pharmacy Policies and Procedures Manual: Last Updated: Month, Day, Year Last Reviewed: Month, Day, YearDocument53 pagesPharmacy Policies and Procedures Manual: Last Updated: Month, Day, Year Last Reviewed: Month, Day, YearFranchesca LugoNo ratings yet
- GC 9 Rizal Module 4 Jose Rizals FamilyDocument9 pagesGC 9 Rizal Module 4 Jose Rizals FamilyFranchesca LugoNo ratings yet
- Ethics: Lugo, Franchesca Nicole Y. BSP 3A Mr. Kenneth SungaDocument10 pagesEthics: Lugo, Franchesca Nicole Y. BSP 3A Mr. Kenneth SungaFranchesca LugoNo ratings yet
- Ethics Module 4 - Lugo, F.N.Document3 pagesEthics Module 4 - Lugo, F.N.Franchesca LugoNo ratings yet
- C-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Document8 pagesC-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Franchesca LugoNo ratings yet
- Tertiary SourcesDocument55 pagesTertiary SourcesFranchesca LugoNo ratings yet
- C-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Document13 pagesC-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Franchesca LugoNo ratings yet
- Angeles University FoundationDocument2 pagesAngeles University FoundationFranchesca LugoNo ratings yet
- C-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Document11 pagesC-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Franchesca LugoNo ratings yet
- Solve THE Following: Write Down The Formula and Include Your Solution and THE UNIT USED. (20 Points) 1 Whole Sheet of Pad PaperDocument3 pagesSolve THE Following: Write Down The Formula and Include Your Solution and THE UNIT USED. (20 Points) 1 Whole Sheet of Pad PaperFranchesca LugoNo ratings yet
- Liquid FormsDocument29 pagesLiquid FormsFranchesca LugoNo ratings yet
- Summery of Htma Theresa - VernonDocument5 pagesSummery of Htma Theresa - Vernonsisi marxNo ratings yet
- Endocrine SystemDocument10 pagesEndocrine SystemPeej Reyes100% (1)
- CortisolDocument27 pagesCortisolCao YunNo ratings yet
- Adrenal InsufficiencyDocument2 pagesAdrenal InsufficiencyTracy NwanneNo ratings yet
- Clinical EndocrinologyDocument35 pagesClinical EndocrinologyBobskinny100% (1)
- 21 - Adrenal CrisisDocument5 pages21 - Adrenal CrisisLenard BangugNo ratings yet
- ENDODocument9 pagesENDOJohn denver FloresNo ratings yet
- Adrenal CrisisDocument4 pagesAdrenal CrisisRichie Marie BajaNo ratings yet
- Adrenal InsufficiencyDocument15 pagesAdrenal InsufficiencyJuvial DavidNo ratings yet
- Disease of Adrenal GlandDocument47 pagesDisease of Adrenal GlandgibreilNo ratings yet
- Endocrine System BulletsDocument28 pagesEndocrine System Bulletswinner gift flowersNo ratings yet
- Addison+conn+cush+feo+adr IncidentalomaDocument65 pagesAddison+conn+cush+feo+adr IncidentalomaMjn BausatNo ratings yet
- Click 2 Achieve BrochureDocument25 pagesClick 2 Achieve BrochureavisekgNo ratings yet
- Week 5: Endocrinology: I. Pituitary ControlDocument26 pagesWeek 5: Endocrinology: I. Pituitary ControlBenjamin NgNo ratings yet
- What Is Adrenal InsufficiencyDocument17 pagesWhat Is Adrenal InsufficiencygammuacNo ratings yet
- Chapter 45 Endocrine DosordersDocument50 pagesChapter 45 Endocrine DosordersShaun Gabriel AmpoNo ratings yet
- A Z Board ReviewDocument64 pagesA Z Board ReviewMohammed Seleam100% (1)
- Questions For Nle Auto Saved)Document32 pagesQuestions For Nle Auto Saved)Julie Ann MurilloNo ratings yet
- Endocrine Function Report Ncm114Document91 pagesEndocrine Function Report Ncm114abcde pwnjabiNo ratings yet
- NCMB316 Rle 2-10-7addison's DiseaseDocument4 pagesNCMB316 Rle 2-10-7addison's DiseaseMaica LectanaNo ratings yet
- Clobetasol CreamDocument9 pagesClobetasol CreamGiulianospharmacyNo ratings yet
- KENALOGDocument4 pagesKENALOGStefan Codrin CriclevitzNo ratings yet
- LL INDIA January 6th 2002 MD/MS Entrance Examination Questions With Suggested AnswersDocument26 pagesLL INDIA January 6th 2002 MD/MS Entrance Examination Questions With Suggested AnswersAnil KumarNo ratings yet
- (Download PDF) Endocrine Emergencies Recognition and Treatment Lynn Loriaux and Chaim Vanek Online Ebook All Chapter PDFDocument42 pages(Download PDF) Endocrine Emergencies Recognition and Treatment Lynn Loriaux and Chaim Vanek Online Ebook All Chapter PDFsherry.lanzo797100% (11)
- Notes: Adrenal HypofunctionDocument4 pagesNotes: Adrenal HypofunctionWiyosa RusdiNo ratings yet
- (Download PDF) Handbook of Diagnostic Endocrinology 3Rd Edition William E Winter Online Ebook All Chapter PDFDocument42 pages(Download PDF) Handbook of Diagnostic Endocrinology 3Rd Edition William E Winter Online Ebook All Chapter PDFwilliam.thomas775100% (11)
- Addison's DiseaseDocument9 pagesAddison's DiseaseEileen Xiao Tieng KhoNo ratings yet
- Chapter 128 - Thyroid and Adrenal Disorders: Episode OverviewDocument15 pagesChapter 128 - Thyroid and Adrenal Disorders: Episode OverviewIkenna EzeiloNo ratings yet











































































































Download as pptx, pdf, or txt
You might also like
- Clinical Chemistry 3: EndocrinologyDocument21 pagesClinical Chemistry 3: EndocrinologyRomie Solacito100% (3)
- Pharmacology 4th Semester BSN Notes, Educational PlatformDocument985 pagesPharmacology 4th Semester BSN Notes, Educational PlatformPen N PapersNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (3)
- Route of AdministrationDocument48 pagesRoute of AdministrationFranchesca LugoNo ratings yet
- Endocrine DisordersDocument77 pagesEndocrine Disordersahmad100% (2)
- Endocrine Vety PharmaDocument16 pagesEndocrine Vety PharmaSunilNo ratings yet
- Endocrine System 2016Document58 pagesEndocrine System 2016museayana5271No ratings yet
- Insulin and Oral Hypoglycemic AgentsDocument27 pagesInsulin and Oral Hypoglycemic Agentsapi-19916399100% (1)
- Anti AsthmaDocument34 pagesAnti AsthmaDRx Raju ChandranNo ratings yet
- Endocrine Drug: T4 Is Secreted in Excess To T3Document10 pagesEndocrine Drug: T4 Is Secreted in Excess To T3emmanuelNo ratings yet
- Module 3.4 - EndocrineDocument5 pagesModule 3.4 - EndocrineCatherine Sinen ObinqueNo ratings yet
- Endocrine Pharmacology by DR - Mayur SaytaDocument27 pagesEndocrine Pharmacology by DR - Mayur Saytasahilthakker2012No ratings yet
- Lecture16 Anti Diabetic DrugsDocument61 pagesLecture16 Anti Diabetic Drugsharis.18No ratings yet
- Management and Medications in Thyroid Strom and Myxoedema ComaDocument41 pagesManagement and Medications in Thyroid Strom and Myxoedema ComaBhavesh kunvarNo ratings yet
- Shaina Dionisia Palacol Candice Guillermo Gelzan RoldanDocument55 pagesShaina Dionisia Palacol Candice Guillermo Gelzan RoldanEdelrose LapitanNo ratings yet
- Ch-10 Endocrine PharmacologyDocument16 pagesCh-10 Endocrine PharmacologyAyro Business CenterNo ratings yet
- Thyroid CrisisDocument34 pagesThyroid CrisisRidyah Ning TyasNo ratings yet
- All Endocrine PharmacologyDocument143 pagesAll Endocrine PharmacologyabenezergebrekirstosNo ratings yet
- Antidiabetic Drugs. Nurse 2024Document32 pagesAntidiabetic Drugs. Nurse 2024Ayro Business CenterNo ratings yet
- Pharmacology Volume 1 Unit 6 EndocrineDocument76 pagesPharmacology Volume 1 Unit 6 EndocrineAkhilesh TiwariNo ratings yet
- The Thyroid Gland PRINT 2021Document9 pagesThe Thyroid Gland PRINT 2021abcde990075No ratings yet
- 05 Chapter Endrocrine SystemDocument40 pages05 Chapter Endrocrine SystemMSKCNo ratings yet
- Pharmacology LectureDocument5 pagesPharmacology LectureAbdullahayad farouqNo ratings yet
- Insulin and Oral HypoglycemicsDocument38 pagesInsulin and Oral HypoglycemicsEdwin GithogeNo ratings yet
- Pancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyDocument69 pagesPancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyRalf EmoteroNo ratings yet
- Seminar 6 - Psychopharmacology - EctDocument108 pagesSeminar 6 - Psychopharmacology - EctA. TivieanNo ratings yet
- Antidiabetic Drugs. 12 May Modified 2016 of 2015 - 2017 11 17 MayDocument54 pagesAntidiabetic Drugs. 12 May Modified 2016 of 2015 - 2017 11 17 Mayblue sapphireNo ratings yet
- Thyroid & Antithyroid Drugs - 2020Document7 pagesThyroid & Antithyroid Drugs - 2020ireneNo ratings yet
- Thyroid DrugsDocument6 pagesThyroid DrugsThe Real UploaderNo ratings yet
- Lecture 9 Endocrine HormonesDocument18 pagesLecture 9 Endocrine HormonesKC PalattaoNo ratings yet
- FO-Antidiabetic-27042020-Blok 7Document64 pagesFO-Antidiabetic-27042020-Blok 7Indah NurhalizaNo ratings yet
- لقطة شاشة ٢٠٢١-٠٢-٠٥ في ١.٤٦.٥٧ مDocument2 pagesلقطة شاشة ٢٠٢١-٠٢-٠٥ في ١.٤٦.٥٧ مDr. Emad Elbadawy د عماد البدويNo ratings yet
- Drug Study On Agents Used Thyroid and Glucose MetabolismDocument18 pagesDrug Study On Agents Used Thyroid and Glucose Metabolismaeliusz19No ratings yet
- Thyroid and Antithyroid DrugsDocument38 pagesThyroid and Antithyroid DrugsbrkbsnNo ratings yet
- What Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsDocument9 pagesWhat Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsIshaani GargNo ratings yet
- Chapter 34 Insulin & Oral Antidiabetic DrugsDocument24 pagesChapter 34 Insulin & Oral Antidiabetic DrugsIlham RamadhanNo ratings yet
- Immunosuppressants NotesDocument20 pagesImmunosuppressants NotesmadcalNo ratings yet
- Pituitary &thyroid NotesDocument7 pagesPituitary &thyroid NotesAli salimNo ratings yet
- Endocrine PharmacologyDocument42 pagesEndocrine PharmacologyAhmed El SharkawyNo ratings yet
- Disease Spotlight: Diabetes Mellitus: Insulin Insulin Is A Drug That Is Used To ControlDocument7 pagesDisease Spotlight: Diabetes Mellitus: Insulin Insulin Is A Drug That Is Used To ControlMIR SARTAJNo ratings yet
- 11 - Drugs For Thyroid Problems2Document51 pages11 - Drugs For Thyroid Problems2nica velanoNo ratings yet
- Diabetes Mellitus-1 3Document18 pagesDiabetes Mellitus-1 3Narmeen RahimNo ratings yet
- 10 Endocrine PharmacologyDocument34 pages10 Endocrine PharmacologyNaol TolchaNo ratings yet
- I. Title: Drugs Affecting The Endocrine System Ii. ReferencesDocument14 pagesI. Title: Drugs Affecting The Endocrine System Ii. ReferencesGenierose YantoNo ratings yet
- Clinical Pharmacy Chapter Seven Thyroid Disorders: Rowa' Al-RamahiDocument16 pagesClinical Pharmacy Chapter Seven Thyroid Disorders: Rowa' Al-Ramahiabdelrhman aboodaNo ratings yet
- Antidiabetic HerbsDocument21 pagesAntidiabetic HerbsUsamaNo ratings yet
- Unit 1 Antidiabetic Drugs Pharmacy-IIDocument69 pagesUnit 1 Antidiabetic Drugs Pharmacy-IIAsad MirajNo ratings yet
- Insulin, Oral Hypoglycemic Agents-1Document23 pagesInsulin, Oral Hypoglycemic Agents-1IbrahimNo ratings yet
- M3 - Lesson 1bDocument20 pagesM3 - Lesson 1bLhara MañoNo ratings yet
- Drugs Used To Treat Diabetes - MellitusDocument37 pagesDrugs Used To Treat Diabetes - MellitusjisooNo ratings yet
- An Overview On Tirzepatide, Dual-Targeted Treatment For Diabetes and ObesityDocument6 pagesAn Overview On Tirzepatide, Dual-Targeted Treatment For Diabetes and ObesityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Endocrine DrugsDocument42 pagesEndocrine DrugsSolaNo ratings yet
- Pharmacology ResearchDocument20 pagesPharmacology ResearchaagalhazmiNo ratings yet
- anaes&DMDocument11 pagesanaes&DMMohamed Satti AbdalsadigNo ratings yet
- 14) Drugs For Thyroid DisordersDocument13 pages14) Drugs For Thyroid DisordersLatiNo ratings yet
- Common Anti-Diabetics and AnticoagulantsDocument14 pagesCommon Anti-Diabetics and AnticoagulantsemmanuelmkibuniNo ratings yet
- Pharmacology LectureDocument6 pagesPharmacology LectureAbdullahayad farouqNo ratings yet
- Thyroid Disorders - 2023Document82 pagesThyroid Disorders - 2023JEPHTHAH KWASI DANSONo ratings yet
- AntiDiabetic Drugs 2 BDocument50 pagesAntiDiabetic Drugs 2 BAvinash RajNo ratings yet
- Insulin and Oral AntidiabeticsDocument24 pagesInsulin and Oral AntidiabeticsMirza Shaharyar Baig100% (1)
- Natural Hormones and Their Synthetic Analogues 2. Hormone Like Substances 3. Drugs That Stimulate or Suppress Hormone SecretionDocument6 pagesNatural Hormones and Their Synthetic Analogues 2. Hormone Like Substances 3. Drugs That Stimulate or Suppress Hormone SecretionMarianne CruzNo ratings yet
- THYROIDDocument24 pagesTHYROIDanaya khan StudentNo ratings yet
- 04 Psych Crash CourseDocument33 pages04 Psych Crash CourseFranchesca LugoNo ratings yet
- What Is The Difference Between Sign and Symptom?Document7 pagesWhat Is The Difference Between Sign and Symptom?Franchesca LugoNo ratings yet
- 2018 UPlink NMAT Review Social Science LectureDocument133 pages2018 UPlink NMAT Review Social Science LectureFranchesca LugoNo ratings yet
- C-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Document11 pagesC-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Franchesca LugoNo ratings yet
- Presented By: VIVEK DEVDocument38 pagesPresented By: VIVEK DEVFranchesca LugoNo ratings yet
- Ishac M2 Cardio Antihypertensives 2010Document16 pagesIshac M2 Cardio Antihypertensives 2010Franchesca LugoNo ratings yet
- Chief Pharmacist Supervising PharmacistDocument3 pagesChief Pharmacist Supervising PharmacistFranchesca LugoNo ratings yet
- Name: Sex: Age:: Waist Hip RatioDocument2 pagesName: Sex: Age:: Waist Hip RatioFranchesca LugoNo ratings yet
- Pharmacy Policies and Procedures Manual: Last Updated: Month, Day, Year Last Reviewed: Month, Day, YearDocument53 pagesPharmacy Policies and Procedures Manual: Last Updated: Month, Day, Year Last Reviewed: Month, Day, YearFranchesca LugoNo ratings yet
- GC 9 Rizal Module 4 Jose Rizals FamilyDocument9 pagesGC 9 Rizal Module 4 Jose Rizals FamilyFranchesca LugoNo ratings yet
- Ethics: Lugo, Franchesca Nicole Y. BSP 3A Mr. Kenneth SungaDocument10 pagesEthics: Lugo, Franchesca Nicole Y. BSP 3A Mr. Kenneth SungaFranchesca LugoNo ratings yet
- Ethics Module 4 - Lugo, F.N.Document3 pagesEthics Module 4 - Lugo, F.N.Franchesca LugoNo ratings yet
- C-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Document8 pagesC-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Franchesca LugoNo ratings yet
- Tertiary SourcesDocument55 pagesTertiary SourcesFranchesca LugoNo ratings yet
- C-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Document13 pagesC-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Franchesca LugoNo ratings yet
- Angeles University FoundationDocument2 pagesAngeles University FoundationFranchesca LugoNo ratings yet
- C-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Document11 pagesC-Gec9 Life and Works of Rizal First Semester - AY 2020-2021Franchesca LugoNo ratings yet
- Solve THE Following: Write Down The Formula and Include Your Solution and THE UNIT USED. (20 Points) 1 Whole Sheet of Pad PaperDocument3 pagesSolve THE Following: Write Down The Formula and Include Your Solution and THE UNIT USED. (20 Points) 1 Whole Sheet of Pad PaperFranchesca LugoNo ratings yet
- Liquid FormsDocument29 pagesLiquid FormsFranchesca LugoNo ratings yet
- Summery of Htma Theresa - VernonDocument5 pagesSummery of Htma Theresa - Vernonsisi marxNo ratings yet
- Endocrine SystemDocument10 pagesEndocrine SystemPeej Reyes100% (1)
- CortisolDocument27 pagesCortisolCao YunNo ratings yet
- Adrenal InsufficiencyDocument2 pagesAdrenal InsufficiencyTracy NwanneNo ratings yet
- Clinical EndocrinologyDocument35 pagesClinical EndocrinologyBobskinny100% (1)
- 21 - Adrenal CrisisDocument5 pages21 - Adrenal CrisisLenard BangugNo ratings yet
- ENDODocument9 pagesENDOJohn denver FloresNo ratings yet
- Adrenal CrisisDocument4 pagesAdrenal CrisisRichie Marie BajaNo ratings yet
- Adrenal InsufficiencyDocument15 pagesAdrenal InsufficiencyJuvial DavidNo ratings yet
- Disease of Adrenal GlandDocument47 pagesDisease of Adrenal GlandgibreilNo ratings yet
- Endocrine System BulletsDocument28 pagesEndocrine System Bulletswinner gift flowersNo ratings yet
- Addison+conn+cush+feo+adr IncidentalomaDocument65 pagesAddison+conn+cush+feo+adr IncidentalomaMjn BausatNo ratings yet
- Click 2 Achieve BrochureDocument25 pagesClick 2 Achieve BrochureavisekgNo ratings yet
- Week 5: Endocrinology: I. Pituitary ControlDocument26 pagesWeek 5: Endocrinology: I. Pituitary ControlBenjamin NgNo ratings yet
- What Is Adrenal InsufficiencyDocument17 pagesWhat Is Adrenal InsufficiencygammuacNo ratings yet
- Chapter 45 Endocrine DosordersDocument50 pagesChapter 45 Endocrine DosordersShaun Gabriel AmpoNo ratings yet
- A Z Board ReviewDocument64 pagesA Z Board ReviewMohammed Seleam100% (1)
- Questions For Nle Auto Saved)Document32 pagesQuestions For Nle Auto Saved)Julie Ann MurilloNo ratings yet
- Endocrine Function Report Ncm114Document91 pagesEndocrine Function Report Ncm114abcde pwnjabiNo ratings yet
- NCMB316 Rle 2-10-7addison's DiseaseDocument4 pagesNCMB316 Rle 2-10-7addison's DiseaseMaica LectanaNo ratings yet
- Clobetasol CreamDocument9 pagesClobetasol CreamGiulianospharmacyNo ratings yet
- KENALOGDocument4 pagesKENALOGStefan Codrin CriclevitzNo ratings yet
- LL INDIA January 6th 2002 MD/MS Entrance Examination Questions With Suggested AnswersDocument26 pagesLL INDIA January 6th 2002 MD/MS Entrance Examination Questions With Suggested AnswersAnil KumarNo ratings yet
- (Download PDF) Endocrine Emergencies Recognition and Treatment Lynn Loriaux and Chaim Vanek Online Ebook All Chapter PDFDocument42 pages(Download PDF) Endocrine Emergencies Recognition and Treatment Lynn Loriaux and Chaim Vanek Online Ebook All Chapter PDFsherry.lanzo797100% (11)
- Notes: Adrenal HypofunctionDocument4 pagesNotes: Adrenal HypofunctionWiyosa RusdiNo ratings yet
- (Download PDF) Handbook of Diagnostic Endocrinology 3Rd Edition William E Winter Online Ebook All Chapter PDFDocument42 pages(Download PDF) Handbook of Diagnostic Endocrinology 3Rd Edition William E Winter Online Ebook All Chapter PDFwilliam.thomas775100% (11)
- Addison's DiseaseDocument9 pagesAddison's DiseaseEileen Xiao Tieng KhoNo ratings yet
- Chapter 128 - Thyroid and Adrenal Disorders: Episode OverviewDocument15 pagesChapter 128 - Thyroid and Adrenal Disorders: Episode OverviewIkenna EzeiloNo ratings yet