Download as pptx, pdf, or txt
You might also like
- Dlp-Triangle CongruenceDocument8 pagesDlp-Triangle CongruenceJoan B. Basco100% (3)
- Financial Time Series Analysis and Prediction With Feature Engineering and Support Vector Machines - Newton - LinchenDocument5 pagesFinancial Time Series Analysis and Prediction With Feature Engineering and Support Vector Machines - Newton - LinchenNewton Linchen100% (1)
- Differential Diagnosis of Flank PainDocument43 pagesDifferential Diagnosis of Flank PainDrArish Mahmood78% (9)
- Q3 G11 Physical Science Module 7Document19 pagesQ3 G11 Physical Science Module 7Lebz RicaramNo ratings yet
- Introduction To Trauma: LSU Medical Student Clerkship, New Orleans, LADocument31 pagesIntroduction To Trauma: LSU Medical Student Clerkship, New Orleans, LAnandangNo ratings yet
- Diagnosis & Treament: ShockDocument52 pagesDiagnosis & Treament: ShockasepNo ratings yet
- Poisoning & BitesDocument12 pagesPoisoning & BitesJudy HandlyNo ratings yet
- DR TahirDocument61 pagesDR TahirRohail GulNo ratings yet
- TRIAGEDocument55 pagesTRIAGELaveena AswaleNo ratings yet
- Cervical Cancer ScreeningDocument25 pagesCervical Cancer Screening6ixSideCreate MNo ratings yet
- BurnsDocument58 pagesBurnsMarie MayNo ratings yet
- Emergency Trauma CareDocument49 pagesEmergency Trauma Careandrei neagNo ratings yet
- Guidelines For Management of Head InjuryDocument18 pagesGuidelines For Management of Head InjuryChellamani UmakanthanNo ratings yet
- 10 AsthmaDocument39 pages10 AsthmaAkash MishraNo ratings yet
- NG and Foley Cath M2 2009Document54 pagesNG and Foley Cath M2 2009aditi268100% (1)
- Bites & Stings PressDocument4 pagesBites & Stings PressNikki CoplandNo ratings yet
- Abc of Burns: Kanwal Khan Lecturer ZCPTDocument35 pagesAbc of Burns: Kanwal Khan Lecturer ZCPTKanwal KhanNo ratings yet
- Day Case Surgery 1LDocument21 pagesDay Case Surgery 1LdrhiwaomerNo ratings yet
- Chest InjuriesDocument19 pagesChest InjuriesAbdi Kumala100% (1)
- Et IntubateDocument47 pagesEt IntubatectuagentNo ratings yet
- WK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TideDocument43 pagesWK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TidePotato PceeNo ratings yet
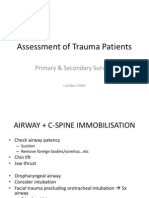
- Primary SurveyDocument19 pagesPrimary SurveyCaroline ChauNo ratings yet
- Cardiac TestsDocument17 pagesCardiac TestsGiorgiana pNo ratings yet
- Cold InjuryDocument50 pagesCold InjurySnehanshNo ratings yet
- ShockDocument21 pagesShockMin-Joo Esther ParkNo ratings yet
- 633815699386510632Document123 pages633815699386510632Muhammad FarisNo ratings yet
- 780 Adult Cardio Resp Assess DSTDocument10 pages780 Adult Cardio Resp Assess DSTGursangeet Kaur100% (1)
- Urinary Tract InfectionsDocument20 pagesUrinary Tract Infectionsbgfhnfg100% (1)
- PS FREL 5 LiftingAndMovingPatientsPowerPointDocument18 pagesPS FREL 5 LiftingAndMovingPatientsPowerPointVirjhon MachsunNo ratings yet
- Antidotes in Opioid Toxicity and Substance Dependence: MIMS Summary TableDocument1 pageAntidotes in Opioid Toxicity and Substance Dependence: MIMS Summary TableJake CaballoNo ratings yet
- Operating Room Preparation: Philipp Acaso Ralph ArcoDocument158 pagesOperating Room Preparation: Philipp Acaso Ralph ArcoTiffany Luv Adrias100% (1)
- Fat Embolism SyndromeDocument26 pagesFat Embolism SyndromeAzni MokhtarNo ratings yet
- BurnsDocument65 pagesBurnsdhainey100% (1)
- Early Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac ArrestDocument9 pagesEarly Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac ArrestHammad AjaNo ratings yet
- Burn ManagementDocument64 pagesBurn Managementabdullah100% (1)
- Preoperative Preparation of The Surgical PatientDocument33 pagesPreoperative Preparation of The Surgical PatientPrincewill SeiyefaNo ratings yet
- Pneumothorax: DR - Naveen Vennilavan R Pg-IiiDocument95 pagesPneumothorax: DR - Naveen Vennilavan R Pg-Iiinaveen vennilavanNo ratings yet
- Examination of Chronic AbdomenDocument43 pagesExamination of Chronic AbdomendrrajeshpsmsNo ratings yet
- Dka Vs Hhs Edit 1Document25 pagesDka Vs Hhs Edit 1Razeen RiyasatNo ratings yet
- First Aid For BurnsDocument21 pagesFirst Aid For Burnsgashbin MahdyNo ratings yet
- Epiglottitis - AMBOSSDocument10 pagesEpiglottitis - AMBOSSSadikNo ratings yet
- Bls Dewasa PKDJB 2022Document74 pagesBls Dewasa PKDJB 2022Halawatul ImanNo ratings yet
- Terminology Causes of Cardiac Arrest C.P.R. For The Adult, Child & Baby Stroke & Stroke ManagementDocument28 pagesTerminology Causes of Cardiac Arrest C.P.R. For The Adult, Child & Baby Stroke & Stroke Managementbusiness911No ratings yet
- Head Injury 5Document68 pagesHead Injury 5drvishal bhattNo ratings yet
- Head Injury 1Document33 pagesHead Injury 1drvishal bhattNo ratings yet
- Assessment and Initial Management of The Trauma Patient: Courtesy of BTLS OntarioDocument42 pagesAssessment and Initial Management of The Trauma Patient: Courtesy of BTLS OntarioAlexandria100% (1)
- Man Age Men T of CancerDocument14 pagesMan Age Men T of CancerKoRnflakesNo ratings yet
- Prepared By: Ailyn AntoqueDocument24 pagesPrepared By: Ailyn Antoquelhyn100% (1)
- Shock: Not Enough Blood Flow?Document3 pagesShock: Not Enough Blood Flow?Genevie GabrielNo ratings yet
- Systemic Inflammatory ResponseDocument2 pagesSystemic Inflammatory Responsesmithaanne20016923No ratings yet
- Chest DrainsDocument22 pagesChest DrainsNuru99100% (3)
- AnaphylaxisDocument1 pageAnaphylaxisLidya YudithNo ratings yet
- CPR 1Document12 pagesCPR 1Renju JoseNo ratings yet
- Burn NotesDocument5 pagesBurn NotespaulineorrNo ratings yet
- First Aid:: Bleedin GDocument20 pagesFirst Aid:: Bleedin GVielka Adap100% (1)
- Military TriageDocument23 pagesMilitary TriageKai CalbesNo ratings yet
- 8.the Atls ProtocolDocument57 pages8.the Atls ProtocolReuben DutiNo ratings yet
- Basic Trauma Life SupportDocument43 pagesBasic Trauma Life SupportperawatNo ratings yet
- Ostomy TrainingDocument37 pagesOstomy Trainingsophia hasanah100% (1)
- BASIC LIFE SUPPORT Basics IntroductionDocument27 pagesBASIC LIFE SUPPORT Basics IntroductionMUKESH SUNDARARAJANNo ratings yet
- Management of Patient With CancerDocument52 pagesManagement of Patient With CancerAru VermaNo ratings yet
- Snake Bite Medical ManagementDocument35 pagesSnake Bite Medical Managementsyarifah nurlailaNo ratings yet
- Septic ShockDocument11 pagesSeptic ShockJonna Mae Agcaoili SalameroNo ratings yet
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Case PresentationDocument21 pagesCase PresentationDrArish MahmoodNo ratings yet
- Management of Peptic UlcerDocument36 pagesManagement of Peptic UlcerDrArish Mahmood100% (1)
- Differential Diagnosis Pain Right HypochondriumDocument35 pagesDifferential Diagnosis Pain Right HypochondriumDrArish Mahmood100% (1)
- Differential Diagnosis of Neck SwellingsDocument24 pagesDifferential Diagnosis of Neck SwellingsDrArish Mahmood100% (3)
- J S Bachs Ornament TableDocument7 pagesJ S Bachs Ornament TableAlmeidaNo ratings yet
- Itch Mechanisms and ManagementDocument464 pagesItch Mechanisms and ManagementGaurav JaswalNo ratings yet
- Peek - POLYETHER ETHER KETONEDocument58 pagesPeek - POLYETHER ETHER KETONEBryan Jesher Dela Cruz100% (1)
- KaizenDocument8 pagesKaizenGigih SetijawanNo ratings yet
- Test Bank For Anatomy and Physiology 10th Edition by PattonDocument32 pagesTest Bank For Anatomy and Physiology 10th Edition by PattonCassandraDuncanmcytd100% (41)
- Swathi Final Project AnilDocument100 pagesSwathi Final Project AnilHussainNo ratings yet
- wst03 01 Que 20220611 1Document28 pageswst03 01 Que 20220611 1Rehan RagibNo ratings yet
- SOAL MID TERM ENGLISH 13 Tyad 1Document6 pagesSOAL MID TERM ENGLISH 13 Tyad 1ani julitaNo ratings yet
- Remembering and ForgettingDocument12 pagesRemembering and ForgettingChrstn BuenaventuraNo ratings yet
- Vizsgaanyag PDFDocument30 pagesVizsgaanyag PDFSipka GergőNo ratings yet
- NO Memo No. 21 S. 2018 Adherence To Training Policy PDFDocument10 pagesNO Memo No. 21 S. 2018 Adherence To Training Policy PDFKemberly Semaña PentonNo ratings yet
- Chapter 2 Indian Economy 1950-1990Document27 pagesChapter 2 Indian Economy 1950-1990Ajay pandeyNo ratings yet
- Denavit-Hartenberg Parameters - WikipediaDocument19 pagesDenavit-Hartenberg Parameters - Wikipediavikas16051998No ratings yet
- Cookie Experimental DesignDocument2 pagesCookie Experimental Designapi-293314791No ratings yet
- En 13237-2003 Terms and Definitions For Equipment and Protective Systems Intended For Use in Potentially Explosive AtmospheresDocument26 pagesEn 13237-2003 Terms and Definitions For Equipment and Protective Systems Intended For Use in Potentially Explosive AtmospheresGargiulo AnitaNo ratings yet
- Redistribution and PBRDocument1 pageRedistribution and PBRdibpalNo ratings yet
- 4J10 CHUNG KA CHUN 4J10 - Untitled DocumentDocument1 page4J10 CHUNG KA CHUN 4J10 - Untitled Document4J10 CHUNG KA CHUN 4J10No ratings yet
- MiddlemarchDocument2 pagesMiddlemarchKanad Prajna DasNo ratings yet
- How To Define A Chart of Accounts in Oracle Apps R12: Month End ProcessDocument18 pagesHow To Define A Chart of Accounts in Oracle Apps R12: Month End ProcessCGNo ratings yet
- Michael & Co. vs. Enriquez (33 Phil 87 (1915)Document3 pagesMichael & Co. vs. Enriquez (33 Phil 87 (1915)Analyn Grace Yongco BasayNo ratings yet
- 1.b Pin-P3.4-Of-8051-Microcontroller-Is-Known-As-Timer...Document5 pages1.b Pin-P3.4-Of-8051-Microcontroller-Is-Known-As-Timer...তানভীর তাঈনNo ratings yet
- The Autism Diagnostic Observation Schedule, Module 4: Application of The Revised Algorithms in An Independent, Well-Defined, Dutch Sample (N 93)Document11 pagesThe Autism Diagnostic Observation Schedule, Module 4: Application of The Revised Algorithms in An Independent, Well-Defined, Dutch Sample (N 93)Laura CamusNo ratings yet
- Atlas Engineering Bar Handbook Rev Jan 2005-Oct 2011Document136 pagesAtlas Engineering Bar Handbook Rev Jan 2005-Oct 2011carlosc19715043No ratings yet
- Scala AccesoriesDocument27 pagesScala AccesoriesZiggy BussyNo ratings yet
- Denman - On FortificationDocument17 pagesDenman - On FortificationkontarexNo ratings yet
- M1 - 02 Nature and Scope of BusinessDocument41 pagesM1 - 02 Nature and Scope of BusinessDiptendu RoyNo ratings yet