Download as pptx, pdf, or txt
You might also like
- EASA Air Law PDFDocument17 pagesEASA Air Law PDFMiyachita Tagahachi100% (5)
- Ogl 482 Thematic Analysis MauldinkDocument34 pagesOgl 482 Thematic Analysis Mauldinkapi-504223947100% (1)
- An Analysis of Consumer Satisfaction Towards Online Food-Ordering AppsDocument8 pagesAn Analysis of Consumer Satisfaction Towards Online Food-Ordering Appsno directionNo ratings yet
- Chapter 4 MalwaDocument33 pagesChapter 4 MalwahoneyNo ratings yet
- Buku Publikasi FKep UH TW II 2021 CompressedDocument118 pagesBuku Publikasi FKep UH TW II 2021 CompressedmakhenNo ratings yet
- The Barbados Drug Information Network: Findings From The 2017 & 2018 ReportsDocument49 pagesThe Barbados Drug Information Network: Findings From The 2017 & 2018 Reportsterrod gangstaNo ratings yet
- A Study To Assess The Effectiveness of Foot Reflexology On Reducing Pain Among Post Caesarean Mother in Smi Hospital, DehradunDocument5 pagesA Study To Assess The Effectiveness of Foot Reflexology On Reducing Pain Among Post Caesarean Mother in Smi Hospital, DehradunIJAR JOURNALNo ratings yet
- xxx-ILC 4.2-024 Poster-Shahed Hossain Bangladesh-2 PDFDocument22 pagesxxx-ILC 4.2-024 Poster-Shahed Hossain Bangladesh-2 PDFRahen Rangan100% (1)
- A Comparative Study To Analyze The Choice For Utilize Public or Private Healthcare Sector of Gandhinagar Residents"Document26 pagesA Comparative Study To Analyze The Choice For Utilize Public or Private Healthcare Sector of Gandhinagar Residents"Pooja ShotriyaNo ratings yet
- Publication - Patients' Awareness Towards Promotional Activities Implemented in HospitalDocument10 pagesPublication - Patients' Awareness Towards Promotional Activities Implemented in HospitalanuNo ratings yet
- GER Bangladesh EngDocument12 pagesGER Bangladesh Engfarhan.anjum20032004No ratings yet
- GER Indonesia EngDocument8 pagesGER Indonesia EngSamuel OlamNo ratings yet
- A Study On Passengers Satisfaction of Private Omni Bus Services in Tenkasi DistrictDocument6 pagesA Study On Passengers Satisfaction of Private Omni Bus Services in Tenkasi DistrictShanmugapriya commerceNo ratings yet
- NGOs Landscape in IndiaDocument1 pageNGOs Landscape in IndiaArvind GopalakrishnanNo ratings yet
- Buying Preferences of Customers For Agri-Inputs From Organized Rural Retail StoresDocument6 pagesBuying Preferences of Customers For Agri-Inputs From Organized Rural Retail StoresDrashtiNo ratings yet
- 15-10-2022-1665819963-8-IJHSS-21.Knowledge and Attitude of The Beneficiaries Towards Activities of Baif Development Research FoundationDocument10 pages15-10-2022-1665819963-8-IJHSS-21.Knowledge and Attitude of The Beneficiaries Towards Activities of Baif Development Research Foundationiaset123No ratings yet
- YAFS5 VisMin DisseminationDocument80 pagesYAFS5 VisMin Disseminationreyesahlette1127No ratings yet
- Ben Elyon Project FinalDocument37 pagesBen Elyon Project FinalRupaNo ratings yet
- Hubungan Peran Kader Posyandu Dalam Meningkatkan Kesehatan Dengan Status Gizi Balita Di Desa Tegaltirto Berbah SlemanDocument11 pagesHubungan Peran Kader Posyandu Dalam Meningkatkan Kesehatan Dengan Status Gizi Balita Di Desa Tegaltirto Berbah SlemanAGHNIANo ratings yet
- BBBP Guidelines 2019Document103 pagesBBBP Guidelines 2019State Resource Centre for Women Andhra PradeshNo ratings yet
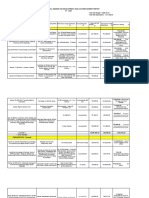
- 2023 Accomplishment ReportDocument14 pages2023 Accomplishment ReportJohn Benedict AquinoNo ratings yet
- 23mba336 RahulripDocument54 pages23mba336 RahulripAjay PandianNo ratings yet
- GAD Accomplishment Report 4th QDocument14 pagesGAD Accomplishment Report 4th QCristine Viernes Gaspar Batay-anNo ratings yet
- 221-Article Text-614-1-10-20210830Document5 pages221-Article Text-614-1-10-20210830Bảo Nhien NguyễnNo ratings yet
- Compliance of Cabagan Slaughterhouse To Health and Environmental Standards2Document42 pagesCompliance of Cabagan Slaughterhouse To Health and Environmental Standards2Freya LytchNo ratings yet
- 23mba336 RipDocument48 pages23mba336 RipAjay PandianNo ratings yet
- Research Project On Women EmpowermentDocument11 pagesResearch Project On Women EmpowermentAnkitNo ratings yet
- g20 Women@Work Ilo OecdDocument11 pagesg20 Women@Work Ilo Oecdkunal sengarNo ratings yet
- Komin Et Al 2020 COVID 19 and Its Impact On Informal Sector Workers A Case Study of ThailandDocument10 pagesKomin Et Al 2020 COVID 19 and Its Impact On Informal Sector Workers A Case Study of ThailandNURUL HAZWANI BINTI ABU BAKARNo ratings yet
- Project Proposal: Total Beneficiaries Include The FollowingDocument7 pagesProject Proposal: Total Beneficiaries Include The FollowingJonalyn MancioNo ratings yet
- Live Project MarketingDocument17 pagesLive Project MarketingShambhunath PaulNo ratings yet
- Gender Dimension in Health and Sustainable Development Goal: NepalDocument24 pagesGender Dimension in Health and Sustainable Development Goal: NepalADBI Events100% (1)
- 2018 ENNS Provincial Dissemination MaguindanaoDocument144 pages2018 ENNS Provincial Dissemination MaguindanaoRheii EstandarteNo ratings yet
- Research PresentationDocument19 pagesResearch Presentation1975samanbandaraNo ratings yet
- Dr. Nili's Scientific Publication (Original Article)Document6 pagesDr. Nili's Scientific Publication (Original Article)kmahmuda2024No ratings yet
- Tennessee Recovery Navigators FY20 ReportDocument11 pagesTennessee Recovery Navigators FY20 ReportAnonymous GF8PPILW5100% (1)
- Accomplishment Report 2022Document3 pagesAccomplishment Report 2022Lyndon Moguad100% (1)
- 4.0 Results and DiscussionsDocument11 pages4.0 Results and Discussionssamra rafiqNo ratings yet
- Viability of Village Dressmaking As An Industry Amidst An Era of Ready-To-Wear GarmentsDocument5 pagesViability of Village Dressmaking As An Industry Amidst An Era of Ready-To-Wear GarmentsKomal sharmaNo ratings yet
- Report Cbeds Sifcomparison 12626790109975 20161101Document2 pagesReport Cbeds Sifcomparison 12626790109975 20161101api-341407707No ratings yet
- 23mba336 - Rahulrip - 1 (1) (1) finalLLLLDocument67 pages23mba336 - Rahulrip - 1 (1) (1) finalLLLLAjay PandianNo ratings yet
- RB Promo For CompaniesDocument19 pagesRB Promo For CompaniesMayank ChadhaNo ratings yet
- A Study On Women Empowerment in The Participation of Activities With Reference To Y.S.R (Kadapa) District, Andhra PradeshDocument10 pagesA Study On Women Empowerment in The Participation of Activities With Reference To Y.S.R (Kadapa) District, Andhra PradeshIAEME PublicationNo ratings yet
- Research Methodology ExampleDocument8 pagesResearch Methodology Exampletrueguyme0825No ratings yet
- Provincial Social Welfare and Development OfficeDocument47 pagesProvincial Social Welfare and Development OfficeJudy Ramos De GuzmanNo ratings yet
- Customers' Attitude Towards ICICI Bank Services A Study With Special Reference To Udumalpet Branch C 1203Document5 pagesCustomers' Attitude Towards ICICI Bank Services A Study With Special Reference To Udumalpet Branch C 1203Ashish MOHARENo ratings yet
- Factors Affecting Consumer's Brand Preference of Small Cars: K. Anandh, Dr. K. Shyama SundarDocument5 pagesFactors Affecting Consumer's Brand Preference of Small Cars: K. Anandh, Dr. K. Shyama SundarJhon RayNo ratings yet
- Medicines Profile Ban EngDocument4 pagesMedicines Profile Ban EngMd K IslamNo ratings yet
- Description of Geta Grant AgencyDocument7 pagesDescription of Geta Grant AgencyQuennee Ronquillo EscobilloNo ratings yet
- Broad Unexposed Skills of Transgender EntrepreneursDocument8 pagesBroad Unexposed Skills of Transgender EntrepreneursIAEME PublicationNo ratings yet
- Revised Guidelines BBBP - 26th April, 2018 - 1Document111 pagesRevised Guidelines BBBP - 26th April, 2018 - 1PIYUSH KUMAR 9D 31No ratings yet
- GAD Plan and Budget - 2020Document4 pagesGAD Plan and Budget - 2020Norma CanoyNo ratings yet
- 4Ps RADDocument9 pages4Ps RADDick Jefferson Ocampo PatingNo ratings yet
- Population, Labour Force and Employment: HapterDocument30 pagesPopulation, Labour Force and Employment: Hapteratiqa aslamNo ratings yet
- Yafs5 Deped Cse Review FinalDocument24 pagesYafs5 Deped Cse Review FinalJervin CeriboNo ratings yet
- 4Document30 pages4api-183349736No ratings yet
- Analysis of Bed Occupancy Rate BOR in Terms of IntDocument8 pagesAnalysis of Bed Occupancy Rate BOR in Terms of IntAnisaNo ratings yet
- Customer Perception Towards Services Provided by Public Sector and Private Sector Banks: A Comparative StudyDocument9 pagesCustomer Perception Towards Services Provided by Public Sector and Private Sector Banks: A Comparative StudyÂáfàąq Ķhąň MăhäđįķNo ratings yet
- A Study On Customer Satisfaction Towards Fast Food Retailers in Madurai City V. KarthigiselvanDocument5 pagesA Study On Customer Satisfaction Towards Fast Food Retailers in Madurai City V. Karthigiselvanrameshbabu1984100% (1)
- A Study On Digital Marketing and Its Impact: March 2024Document5 pagesA Study On Digital Marketing and Its Impact: March 2024മിന്നൽ പാലാ സജിNo ratings yet
- A Study On Customers Perception Towards House Loan: AbstractDocument6 pagesA Study On Customers Perception Towards House Loan: Abstractsenthilkumar SNo ratings yet
- Poverty, Vulnerability, and Fiscal Sustainability in the People’s Republic of ChinaFrom EverandPoverty, Vulnerability, and Fiscal Sustainability in the People’s Republic of ChinaNo ratings yet
- Presentation - Gender and DevelopmentDocument20 pagesPresentation - Gender and DevelopmentrezaNo ratings yet
- Reasons and Solutions For The Syrian Refugee CrisisDocument13 pagesReasons and Solutions For The Syrian Refugee CrisisrezaNo ratings yet
- Social Welfare System in BangladeshDocument14 pagesSocial Welfare System in BangladeshrezaNo ratings yet
- Declining NeighborhoodDocument15 pagesDeclining NeighborhoodrezaNo ratings yet
- Contribution of DR Muthulakshmi Reddy To Women Empowerment A Historical StudyDocument11 pagesContribution of DR Muthulakshmi Reddy To Women Empowerment A Historical StudyPve ANo ratings yet
- Educational Values' Analysis Related To KHD'S Principle in The Ron Clark Story MovieDocument5 pagesEducational Values' Analysis Related To KHD'S Principle in The Ron Clark Story MovieJamuna raiNo ratings yet
- Ibt-Practice Paper Grade 7 Read The Extract and Answer The Following QuestionsDocument6 pagesIbt-Practice Paper Grade 7 Read The Extract and Answer The Following QuestionsArchi ArchiNo ratings yet
- Toys "R" Us, Inc. Is The World's Leading Dedicated Toy and Juvenile Products Retailer, Offering ADocument6 pagesToys "R" Us, Inc. Is The World's Leading Dedicated Toy and Juvenile Products Retailer, Offering Aakak00No ratings yet
- ToeflDocument7 pagesToeflNadia TussolehaNo ratings yet
- Answer Sheet: H'Wag Kalimutang Isulat Ang Buong Pangalan! Dito Na Mismo Magsasagot Sa Answer SheetDocument2 pagesAnswer Sheet: H'Wag Kalimutang Isulat Ang Buong Pangalan! Dito Na Mismo Magsasagot Sa Answer Sheetmae santosNo ratings yet
- Introductory Message: (Sample)Document5 pagesIntroductory Message: (Sample)Jayden EnzoNo ratings yet
- MATHEMATICA - Google SearchDocument3 pagesMATHEMATICA - Google SearchzoksiNo ratings yet
- Optimisation and Forecasting of Building Maintenance and Renewals For Various Types of Local Government BuildingsDocument143 pagesOptimisation and Forecasting of Building Maintenance and Renewals For Various Types of Local Government Buildingsmuhammad auliaNo ratings yet
- Marketing Case QuestionsDocument3 pagesMarketing Case QuestionsFaye WongNo ratings yet
- Core-Periphery ModelDocument11 pagesCore-Periphery ModelAndrzej KlimczukNo ratings yet
- SafeDocument3 pagesSafeManan WargeNo ratings yet
- Tomcat: VF-84 Jolly RogersDocument36 pagesTomcat: VF-84 Jolly RogersHenryk Szczaw100% (1)
- Research Design & Review of LiteratureDocument12 pagesResearch Design & Review of Literaturesunit dasNo ratings yet
- INTROandCh.1 Case4andAgainstMLM 6 1 11 PDFDocument21 pagesINTROandCh.1 Case4andAgainstMLM 6 1 11 PDFDarkoNo ratings yet
- Labour Law Lay Off RetrenchmentDocument13 pagesLabour Law Lay Off RetrenchmentosumNo ratings yet
- Lesson30-Our Class BandDocument10 pagesLesson30-Our Class BandPhan TrinhNo ratings yet
- Second Language Acquisition: General Course BooksDocument9 pagesSecond Language Acquisition: General Course BooksAbdullatif AlshattiNo ratings yet
- Manhole Pathdetection Major ProjectDocument68 pagesManhole Pathdetection Major ProjectPRAVEEN KATHULANo ratings yet
- GR No 231737 - Heirs of Tunged v. Sta Lucia Realty Development Corp PDFDocument7 pagesGR No 231737 - Heirs of Tunged v. Sta Lucia Realty Development Corp PDFKristela AdraincemNo ratings yet
- Smart Growth & Aging - Building Aging-Sensitive CommunitiesDocument16 pagesSmart Growth & Aging - Building Aging-Sensitive CommunitiestbeedleNo ratings yet
- Southern Davao National High School: Republic of The Philippines Department of Education Region XiDocument21 pagesSouthern Davao National High School: Republic of The Philippines Department of Education Region Xijanice may relampagosNo ratings yet
- Connectivity Onboard: AKKA Offers Its Comprehensive Connectivity Solution For Your AircraftDocument2 pagesConnectivity Onboard: AKKA Offers Its Comprehensive Connectivity Solution For Your AircraftDami HaNo ratings yet
- People Vs Dela CruzDocument1 pagePeople Vs Dela CruzSherby Mae BautistaNo ratings yet
- Final Report - December 2011 Banquet Hall: Project TeamDocument23 pagesFinal Report - December 2011 Banquet Hall: Project Teamwaqasfarooq75_396423No ratings yet
- Ruang LingkupDocument7 pagesRuang LingkupRiani MahalalitaNo ratings yet
- Customs Valuation System PrelimDocument26 pagesCustoms Valuation System Prelim2 BNo ratings yet
- Land LawsDocument202 pagesLand LawsmahabaleshNo ratings yet