
Drug Interactions: DR Michelle Munyoro MBCHB, MCPH (Uz) 6 February 2019
Drug Interactions: DR Michelle Munyoro MBCHB, MCPH (Uz) 6 February 2019
You might also like
- Washington State University nrf2 Study Raises Health Promoting Factors-NotesDocument26 pagesWashington State University nrf2 Study Raises Health Promoting Factors-Notesapi-253513646100% (4)
- SNS and PNS Drugs (Cholinergics and Adrenergics)Document5 pagesSNS and PNS Drugs (Cholinergics and Adrenergics)Whitney Krabbenhoft100% (1)
- Pharmacology Medical Suffixes Cheat SheetDocument1 pagePharmacology Medical Suffixes Cheat SheetPattyNo ratings yet
- Case Study DM 2 PWDTDocument8 pagesCase Study DM 2 PWDTsantis_8No ratings yet
- BREX Pharmacy Review Module 1Document9 pagesBREX Pharmacy Review Module 1Kenneth DayritNo ratings yet
- Oman Pharmacist Licensing Exam McqsDocument186 pagesOman Pharmacist Licensing Exam McqsMuhammad Amin100% (6)
- Advanced Neuropharmacology: Sharmeen AsadDocument47 pagesAdvanced Neuropharmacology: Sharmeen Asadimtiajahmed fahimNo ratings yet
- AntiemeticsDocument16 pagesAntiemeticswalt65No ratings yet
- Drug Interactions HandoutDocument5 pagesDrug Interactions HandoutBhavin DesaiNo ratings yet
- Enzyme Inducers and Inhibitors TransDocument6 pagesEnzyme Inducers and Inhibitors TransLeonallee MayorNo ratings yet
- Adrenergic AgentsDocument57 pagesAdrenergic AgentsAn Lo100% (1)
- 3 Treatment of HypertensionDocument7 pages3 Treatment of HypertensiontiaraNo ratings yet
- Design of Dosage Regimens:: 1. Introduction To Clinical PharmacokineticsDocument1 pageDesign of Dosage Regimens:: 1. Introduction To Clinical PharmacokineticsYuppie RajNo ratings yet
- Mu 002Document10 pagesMu 002chandanNo ratings yet
- Pharmacotherapy of HTNDocument57 pagesPharmacotherapy of HTNAbera JamboNo ratings yet
- Pharmacodynamics 4Document28 pagesPharmacodynamics 4علي المحترفNo ratings yet
- MSPH Biostatistics FlyerDocument2 pagesMSPH Biostatistics FlyerJoyce MalitNo ratings yet
- Anti EmeticsDocument29 pagesAnti EmeticsBezawit TsigeNo ratings yet
- AntiemeticsDocument25 pagesAntiemeticsPridho GaziansyahNo ratings yet
- 07 Dosage RegimenDocument44 pages07 Dosage Regimenzetttttttttt100% (3)
- Prefix Suffix MnemonicsDocument5 pagesPrefix Suffix MnemonicsPj MontecilloNo ratings yet
- Factors Affecting Drug AbsorptionDocument11 pagesFactors Affecting Drug AbsorptionClarilaine JavierNo ratings yet
- Pharmaco DynamicsDocument7 pagesPharmaco DynamicsDavid NicholasNo ratings yet
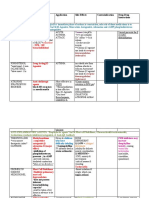
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDocument3 pagesDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinNo ratings yet
- Study Guide PNS and CNSDocument7 pagesStudy Guide PNS and CNSsquicciariniNo ratings yet
- Central Nervous System Pharmacology: Elly Nurus SakinahDocument64 pagesCentral Nervous System Pharmacology: Elly Nurus Sakinahkareem92No ratings yet
- Clinical Toxicology Principles and MechanismsDocument4 pagesClinical Toxicology Principles and MechanismsLyadelou Fortu0% (1)
- Pharmaceutical Care Plan and Documentaion of Pharmacotherapy Intervention (MTM)Document67 pagesPharmaceutical Care Plan and Documentaion of Pharmacotherapy Intervention (MTM)CAROL ANN PATITICONo ratings yet
- Therapeutic Drug Monitoring in The ElderlyDocument3 pagesTherapeutic Drug Monitoring in The ElderlyKristine BaringNo ratings yet
- Anticancer Drugs: Pharmacology 2Document74 pagesAnticancer Drugs: Pharmacology 2Hannah Laput100% (1)
- AnxietyDocument5 pagesAnxietyJohn HolmesNo ratings yet
- Pharmacology of The GITDocument31 pagesPharmacology of The GITmarviecute22No ratings yet
- Respiratory Stimulants, Expectorants and Anti-TussivesDocument16 pagesRespiratory Stimulants, Expectorants and Anti-TussivesAshish Mittal0% (3)
- Pharmacology CNS DrugsDocument15 pagesPharmacology CNS DrugsM Youssif Elkady100% (1)
- Journal Club Presentation On Pancreatic CancerDocument1 pageJournal Club Presentation On Pancreatic Cancercusom34No ratings yet
- Psycho PharmaDocument8 pagesPsycho PharmaMark JosephNo ratings yet
- Beta Lactam AntibioticsDocument94 pagesBeta Lactam AntibioticsHely PatelNo ratings yet
- Drugs Interaction1Document13 pagesDrugs Interaction1Akshay MandhotraNo ratings yet
- CNS Pharmacology: Abebe Ejigu Departmenet of PharmacologyDocument358 pagesCNS Pharmacology: Abebe Ejigu Departmenet of PharmacologyMulugeta TesfayNo ratings yet
- Antiparkinsonian Drugs: Dr. Jahid Senior Lecturer KuinDocument51 pagesAntiparkinsonian Drugs: Dr. Jahid Senior Lecturer KuinfahmiNo ratings yet
- Drugs Acting On The Gastrointestinal TractDocument27 pagesDrugs Acting On The Gastrointestinal TractJames PerianayagamNo ratings yet
- Antimalarial DrugsDocument53 pagesAntimalarial DrugsAmitKumar0% (1)
- NHS Antibiotice PDFDocument2 pagesNHS Antibiotice PDFHoratiu OanaNo ratings yet
- 3 NeurotransmissionDocument31 pages3 Neurotransmissionsarahcho12152No ratings yet
- Pharmacology Case StudyDocument4 pagesPharmacology Case StudyRichard S. RoxasNo ratings yet
- PharmecogenomicsDocument21 pagesPharmecogenomicsRatan Ratan100% (1)
- Pharm Drug Outline AdrDocument1 pagePharm Drug Outline AdrCess Lagera YbanezNo ratings yet
- Antiviral Drugs Acting Against RNA Viruses: HIV: PHRM 412Document57 pagesAntiviral Drugs Acting Against RNA Viruses: HIV: PHRM 412Apurba Sarker ApuNo ratings yet
- Clinical PharmacokineticsDocument36 pagesClinical PharmacokineticsWalaa Yousef100% (1)
- Antibiotic Summary - DraftDocument10 pagesAntibiotic Summary - DraftStrept Pneumonia100% (1)
- Autocoids and Their AntagonistsDocument19 pagesAutocoids and Their AntagonistsHossein Sehati100% (1)
- General Pharmacology - Sources of Drugs and Routes of AdministrationDocument48 pagesGeneral Pharmacology - Sources of Drugs and Routes of AdministrationDhriti Brahma78% (9)
- AntiemeticDocument36 pagesAntiemeticravannofanizza100% (1)
- PHARMACOLOGY Students WorkbookDocument87 pagesPHARMACOLOGY Students WorkbookPABLO, JACKSON P.No ratings yet
- Adverse Reactions SlideshowDocument40 pagesAdverse Reactions SlideshowGary MaoNo ratings yet
- GIT DrugsDocument180 pagesGIT DrugsMaria Linevel Balderamos Dalida100% (2)
- Pharmacology - Anti-Inflammatory Drugs - Corticosteroid, NSAID, Leukotriene (Eicosanoids)Document9 pagesPharmacology - Anti-Inflammatory Drugs - Corticosteroid, NSAID, Leukotriene (Eicosanoids)Itharshan IndreswaranNo ratings yet
- Drug InteractionDocument23 pagesDrug Interactionsinghjsanjay885100% (1)
- Patient CouncellingDocument21 pagesPatient Councellingkeerthana100% (1)
- Bronchodilator & Other Drugs Used in AsthmaDocument15 pagesBronchodilator & Other Drugs Used in AsthmaGenta JagadNo ratings yet
- Opioids: Zainab Sabrie Pharmd MpharmDocument32 pagesOpioids: Zainab Sabrie Pharmd MpharmCabdiladif Ahmed McrfNo ratings yet
- Pharmacotherapeutics UNIT1Document44 pagesPharmacotherapeutics UNIT1Bharti ChauhanNo ratings yet
- Pharmacogenomics of Human Drug Transporters: Clinical ImpactsFrom EverandPharmacogenomics of Human Drug Transporters: Clinical ImpactsNo ratings yet
- ART Treatment 1406failure Interdepartmental PresentationDocument43 pagesART Treatment 1406failure Interdepartmental PresentationStanley Tatenda MukonoNo ratings yet
- Antiretroviral TreatmentDocument32 pagesAntiretroviral TreatmentStanley Tatenda MukonoNo ratings yet
- Drug Use in Pregnancy and Breast FeedingDocument28 pagesDrug Use in Pregnancy and Breast FeedingStanley Tatenda MukonoNo ratings yet
- Drugs and Sports: Drug Doping CfbnhachiDocument40 pagesDrugs and Sports: Drug Doping CfbnhachiStanley Tatenda MukonoNo ratings yet
- Drugs and Renal DiseasesDocument31 pagesDrugs and Renal DiseasesStanley Tatenda MukonoNo ratings yet
- Pharmacology StudentnotesDocument55 pagesPharmacology StudentnotesPasalau Daria VasilicaNo ratings yet
- 8 Principles of Drug Metabolism, With An Emphasis On Psychiatric DrugsDocument32 pages8 Principles of Drug Metabolism, With An Emphasis On Psychiatric Drugstaro0% (1)
- XenobioticsDocument2 pagesXenobioticsKarthik SNo ratings yet
- Farmaco LectureDocument117 pagesFarmaco LectureanaNo ratings yet
- Ecotoxicology, The History and Present Direction (Document9 pagesEcotoxicology, The History and Present Direction (Gonzalo Martínez ParadaNo ratings yet
- Liver As Endocrine - Stuart WhiteDocument53 pagesLiver As Endocrine - Stuart WhitechicanahenoNo ratings yet
- Pediatric Drug DirectoryDocument404 pagesPediatric Drug DirectoryAlfitra Halil100% (1)
- UntitledDocument964 pagesUntitledMarie GdlNo ratings yet
- Ketamine (INN) : Update Review ReportDocument46 pagesKetamine (INN) : Update Review ReportJeremia AnkesaNo ratings yet
- The Protein: Presented by Dr. Shazzad Hosain Asst. Prof. EECS, NSUDocument157 pagesThe Protein: Presented by Dr. Shazzad Hosain Asst. Prof. EECS, NSUAlimushwan AdnanNo ratings yet
- The Liver's Role in Hormone BalanceDocument6 pagesThe Liver's Role in Hormone Balancegraceenggint8799No ratings yet
- MC I Lesson Plan SRDDocument22 pagesMC I Lesson Plan SRDbijoy82No ratings yet
- LifeWave X39 Pilot Demuestra Cambios Ligeros ActivadosDocument12 pagesLifeWave X39 Pilot Demuestra Cambios Ligeros Activadosave_fenix_mileniumNo ratings yet
- Basic Principles of Pharmacology Handout PDFDocument111 pagesBasic Principles of Pharmacology Handout PDFRazel Kinette AzotesNo ratings yet
- PharmacogeneticsDocument36 pagesPharmacogeneticsAmy YuenNo ratings yet
- Pharmacokinetics 2Document62 pagesPharmacokinetics 2Dr. SaniaNo ratings yet
- Tutorial Work, 217 Questions and Answers - MCQ's Tutorial Work, 217 Questions and Answers - MCQ'sDocument32 pagesTutorial Work, 217 Questions and Answers - MCQ's Tutorial Work, 217 Questions and Answers - MCQ'syusser77.No ratings yet
- Pharma Gujjjju IndiaDocument241 pagesPharma Gujjjju IndiaHarsh NimavatNo ratings yet
- M.Sc. Semester IV Syllabus DISTRIBUTIONDocument16 pagesM.Sc. Semester IV Syllabus DISTRIBUTIONSuvNo ratings yet
- Fate of The Drug: Joanne Katherine T. Manlusoc, MSCDocument29 pagesFate of The Drug: Joanne Katherine T. Manlusoc, MSCChinenye AkwueNo ratings yet
- Pharmacokinetics: The Absorption, Distribution, and Excretion of DrugsDocument14 pagesPharmacokinetics: The Absorption, Distribution, and Excretion of DrugsAriiNo ratings yet
- Xenobiotic Metabolism PDFDocument50 pagesXenobiotic Metabolism PDFroxy8marie8chanNo ratings yet
- PHM 3471 Merged Week (1-6)Document303 pagesPHM 3471 Merged Week (1-6)Lisa MuthiniNo ratings yet
- 3.2. Biochemical Biomarkers in Algae and Marine PollutionDocument15 pages3.2. Biochemical Biomarkers in Algae and Marine Pollutionteddy_constantinNo ratings yet
- Seminar On Chronopharmacokinetics: Visit For More Ppt's & MaterialDocument38 pagesSeminar On Chronopharmacokinetics: Visit For More Ppt's & MaterialGANESH KUMAR JELLANo ratings yet
- Lecture 2 Drug Metabolism Phase IIDocument27 pagesLecture 2 Drug Metabolism Phase IIfeegame7No ratings yet
- 1 Principles of Toxicology PDFDocument85 pages1 Principles of Toxicology PDFMariefe BlayaNo ratings yet





























































































Download as pptx, pdf, or txt
You might also like
- Washington State University nrf2 Study Raises Health Promoting Factors-NotesDocument26 pagesWashington State University nrf2 Study Raises Health Promoting Factors-Notesapi-253513646100% (4)
- SNS and PNS Drugs (Cholinergics and Adrenergics)Document5 pagesSNS and PNS Drugs (Cholinergics and Adrenergics)Whitney Krabbenhoft100% (1)
- Pharmacology Medical Suffixes Cheat SheetDocument1 pagePharmacology Medical Suffixes Cheat SheetPattyNo ratings yet
- Case Study DM 2 PWDTDocument8 pagesCase Study DM 2 PWDTsantis_8No ratings yet
- BREX Pharmacy Review Module 1Document9 pagesBREX Pharmacy Review Module 1Kenneth DayritNo ratings yet
- Oman Pharmacist Licensing Exam McqsDocument186 pagesOman Pharmacist Licensing Exam McqsMuhammad Amin100% (6)
- Advanced Neuropharmacology: Sharmeen AsadDocument47 pagesAdvanced Neuropharmacology: Sharmeen Asadimtiajahmed fahimNo ratings yet
- AntiemeticsDocument16 pagesAntiemeticswalt65No ratings yet
- Drug Interactions HandoutDocument5 pagesDrug Interactions HandoutBhavin DesaiNo ratings yet
- Enzyme Inducers and Inhibitors TransDocument6 pagesEnzyme Inducers and Inhibitors TransLeonallee MayorNo ratings yet
- Adrenergic AgentsDocument57 pagesAdrenergic AgentsAn Lo100% (1)
- 3 Treatment of HypertensionDocument7 pages3 Treatment of HypertensiontiaraNo ratings yet
- Design of Dosage Regimens:: 1. Introduction To Clinical PharmacokineticsDocument1 pageDesign of Dosage Regimens:: 1. Introduction To Clinical PharmacokineticsYuppie RajNo ratings yet
- Mu 002Document10 pagesMu 002chandanNo ratings yet
- Pharmacotherapy of HTNDocument57 pagesPharmacotherapy of HTNAbera JamboNo ratings yet
- Pharmacodynamics 4Document28 pagesPharmacodynamics 4علي المحترفNo ratings yet
- MSPH Biostatistics FlyerDocument2 pagesMSPH Biostatistics FlyerJoyce MalitNo ratings yet
- Anti EmeticsDocument29 pagesAnti EmeticsBezawit TsigeNo ratings yet
- AntiemeticsDocument25 pagesAntiemeticsPridho GaziansyahNo ratings yet
- 07 Dosage RegimenDocument44 pages07 Dosage Regimenzetttttttttt100% (3)
- Prefix Suffix MnemonicsDocument5 pagesPrefix Suffix MnemonicsPj MontecilloNo ratings yet
- Factors Affecting Drug AbsorptionDocument11 pagesFactors Affecting Drug AbsorptionClarilaine JavierNo ratings yet
- Pharmaco DynamicsDocument7 pagesPharmaco DynamicsDavid NicholasNo ratings yet
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDocument3 pagesDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinNo ratings yet
- Study Guide PNS and CNSDocument7 pagesStudy Guide PNS and CNSsquicciariniNo ratings yet
- Central Nervous System Pharmacology: Elly Nurus SakinahDocument64 pagesCentral Nervous System Pharmacology: Elly Nurus Sakinahkareem92No ratings yet
- Clinical Toxicology Principles and MechanismsDocument4 pagesClinical Toxicology Principles and MechanismsLyadelou Fortu0% (1)
- Pharmaceutical Care Plan and Documentaion of Pharmacotherapy Intervention (MTM)Document67 pagesPharmaceutical Care Plan and Documentaion of Pharmacotherapy Intervention (MTM)CAROL ANN PATITICONo ratings yet
- Therapeutic Drug Monitoring in The ElderlyDocument3 pagesTherapeutic Drug Monitoring in The ElderlyKristine BaringNo ratings yet
- Anticancer Drugs: Pharmacology 2Document74 pagesAnticancer Drugs: Pharmacology 2Hannah Laput100% (1)
- AnxietyDocument5 pagesAnxietyJohn HolmesNo ratings yet
- Pharmacology of The GITDocument31 pagesPharmacology of The GITmarviecute22No ratings yet
- Respiratory Stimulants, Expectorants and Anti-TussivesDocument16 pagesRespiratory Stimulants, Expectorants and Anti-TussivesAshish Mittal0% (3)
- Pharmacology CNS DrugsDocument15 pagesPharmacology CNS DrugsM Youssif Elkady100% (1)
- Journal Club Presentation On Pancreatic CancerDocument1 pageJournal Club Presentation On Pancreatic Cancercusom34No ratings yet
- Psycho PharmaDocument8 pagesPsycho PharmaMark JosephNo ratings yet
- Beta Lactam AntibioticsDocument94 pagesBeta Lactam AntibioticsHely PatelNo ratings yet
- Drugs Interaction1Document13 pagesDrugs Interaction1Akshay MandhotraNo ratings yet
- CNS Pharmacology: Abebe Ejigu Departmenet of PharmacologyDocument358 pagesCNS Pharmacology: Abebe Ejigu Departmenet of PharmacologyMulugeta TesfayNo ratings yet
- Antiparkinsonian Drugs: Dr. Jahid Senior Lecturer KuinDocument51 pagesAntiparkinsonian Drugs: Dr. Jahid Senior Lecturer KuinfahmiNo ratings yet
- Drugs Acting On The Gastrointestinal TractDocument27 pagesDrugs Acting On The Gastrointestinal TractJames PerianayagamNo ratings yet
- Antimalarial DrugsDocument53 pagesAntimalarial DrugsAmitKumar0% (1)
- NHS Antibiotice PDFDocument2 pagesNHS Antibiotice PDFHoratiu OanaNo ratings yet
- 3 NeurotransmissionDocument31 pages3 Neurotransmissionsarahcho12152No ratings yet
- Pharmacology Case StudyDocument4 pagesPharmacology Case StudyRichard S. RoxasNo ratings yet
- PharmecogenomicsDocument21 pagesPharmecogenomicsRatan Ratan100% (1)
- Pharm Drug Outline AdrDocument1 pagePharm Drug Outline AdrCess Lagera YbanezNo ratings yet
- Antiviral Drugs Acting Against RNA Viruses: HIV: PHRM 412Document57 pagesAntiviral Drugs Acting Against RNA Viruses: HIV: PHRM 412Apurba Sarker ApuNo ratings yet
- Clinical PharmacokineticsDocument36 pagesClinical PharmacokineticsWalaa Yousef100% (1)
- Antibiotic Summary - DraftDocument10 pagesAntibiotic Summary - DraftStrept Pneumonia100% (1)
- Autocoids and Their AntagonistsDocument19 pagesAutocoids and Their AntagonistsHossein Sehati100% (1)
- General Pharmacology - Sources of Drugs and Routes of AdministrationDocument48 pagesGeneral Pharmacology - Sources of Drugs and Routes of AdministrationDhriti Brahma78% (9)
- AntiemeticDocument36 pagesAntiemeticravannofanizza100% (1)
- PHARMACOLOGY Students WorkbookDocument87 pagesPHARMACOLOGY Students WorkbookPABLO, JACKSON P.No ratings yet
- Adverse Reactions SlideshowDocument40 pagesAdverse Reactions SlideshowGary MaoNo ratings yet
- GIT DrugsDocument180 pagesGIT DrugsMaria Linevel Balderamos Dalida100% (2)
- Pharmacology - Anti-Inflammatory Drugs - Corticosteroid, NSAID, Leukotriene (Eicosanoids)Document9 pagesPharmacology - Anti-Inflammatory Drugs - Corticosteroid, NSAID, Leukotriene (Eicosanoids)Itharshan IndreswaranNo ratings yet
- Drug InteractionDocument23 pagesDrug Interactionsinghjsanjay885100% (1)
- Patient CouncellingDocument21 pagesPatient Councellingkeerthana100% (1)
- Bronchodilator & Other Drugs Used in AsthmaDocument15 pagesBronchodilator & Other Drugs Used in AsthmaGenta JagadNo ratings yet
- Opioids: Zainab Sabrie Pharmd MpharmDocument32 pagesOpioids: Zainab Sabrie Pharmd MpharmCabdiladif Ahmed McrfNo ratings yet
- Pharmacotherapeutics UNIT1Document44 pagesPharmacotherapeutics UNIT1Bharti ChauhanNo ratings yet
- Pharmacogenomics of Human Drug Transporters: Clinical ImpactsFrom EverandPharmacogenomics of Human Drug Transporters: Clinical ImpactsNo ratings yet
- ART Treatment 1406failure Interdepartmental PresentationDocument43 pagesART Treatment 1406failure Interdepartmental PresentationStanley Tatenda MukonoNo ratings yet
- Antiretroviral TreatmentDocument32 pagesAntiretroviral TreatmentStanley Tatenda MukonoNo ratings yet
- Drug Use in Pregnancy and Breast FeedingDocument28 pagesDrug Use in Pregnancy and Breast FeedingStanley Tatenda MukonoNo ratings yet
- Drugs and Sports: Drug Doping CfbnhachiDocument40 pagesDrugs and Sports: Drug Doping CfbnhachiStanley Tatenda MukonoNo ratings yet
- Drugs and Renal DiseasesDocument31 pagesDrugs and Renal DiseasesStanley Tatenda MukonoNo ratings yet
- Pharmacology StudentnotesDocument55 pagesPharmacology StudentnotesPasalau Daria VasilicaNo ratings yet
- 8 Principles of Drug Metabolism, With An Emphasis On Psychiatric DrugsDocument32 pages8 Principles of Drug Metabolism, With An Emphasis On Psychiatric Drugstaro0% (1)
- XenobioticsDocument2 pagesXenobioticsKarthik SNo ratings yet
- Farmaco LectureDocument117 pagesFarmaco LectureanaNo ratings yet
- Ecotoxicology, The History and Present Direction (Document9 pagesEcotoxicology, The History and Present Direction (Gonzalo Martínez ParadaNo ratings yet
- Liver As Endocrine - Stuart WhiteDocument53 pagesLiver As Endocrine - Stuart WhitechicanahenoNo ratings yet
- Pediatric Drug DirectoryDocument404 pagesPediatric Drug DirectoryAlfitra Halil100% (1)
- UntitledDocument964 pagesUntitledMarie GdlNo ratings yet
- Ketamine (INN) : Update Review ReportDocument46 pagesKetamine (INN) : Update Review ReportJeremia AnkesaNo ratings yet
- The Protein: Presented by Dr. Shazzad Hosain Asst. Prof. EECS, NSUDocument157 pagesThe Protein: Presented by Dr. Shazzad Hosain Asst. Prof. EECS, NSUAlimushwan AdnanNo ratings yet
- The Liver's Role in Hormone BalanceDocument6 pagesThe Liver's Role in Hormone Balancegraceenggint8799No ratings yet
- MC I Lesson Plan SRDDocument22 pagesMC I Lesson Plan SRDbijoy82No ratings yet
- LifeWave X39 Pilot Demuestra Cambios Ligeros ActivadosDocument12 pagesLifeWave X39 Pilot Demuestra Cambios Ligeros Activadosave_fenix_mileniumNo ratings yet
- Basic Principles of Pharmacology Handout PDFDocument111 pagesBasic Principles of Pharmacology Handout PDFRazel Kinette AzotesNo ratings yet
- PharmacogeneticsDocument36 pagesPharmacogeneticsAmy YuenNo ratings yet
- Pharmacokinetics 2Document62 pagesPharmacokinetics 2Dr. SaniaNo ratings yet
- Tutorial Work, 217 Questions and Answers - MCQ's Tutorial Work, 217 Questions and Answers - MCQ'sDocument32 pagesTutorial Work, 217 Questions and Answers - MCQ's Tutorial Work, 217 Questions and Answers - MCQ'syusser77.No ratings yet
- Pharma Gujjjju IndiaDocument241 pagesPharma Gujjjju IndiaHarsh NimavatNo ratings yet
- M.Sc. Semester IV Syllabus DISTRIBUTIONDocument16 pagesM.Sc. Semester IV Syllabus DISTRIBUTIONSuvNo ratings yet
- Fate of The Drug: Joanne Katherine T. Manlusoc, MSCDocument29 pagesFate of The Drug: Joanne Katherine T. Manlusoc, MSCChinenye AkwueNo ratings yet
- Pharmacokinetics: The Absorption, Distribution, and Excretion of DrugsDocument14 pagesPharmacokinetics: The Absorption, Distribution, and Excretion of DrugsAriiNo ratings yet
- Xenobiotic Metabolism PDFDocument50 pagesXenobiotic Metabolism PDFroxy8marie8chanNo ratings yet
- PHM 3471 Merged Week (1-6)Document303 pagesPHM 3471 Merged Week (1-6)Lisa MuthiniNo ratings yet
- 3.2. Biochemical Biomarkers in Algae and Marine PollutionDocument15 pages3.2. Biochemical Biomarkers in Algae and Marine Pollutionteddy_constantinNo ratings yet
- Seminar On Chronopharmacokinetics: Visit For More Ppt's & MaterialDocument38 pagesSeminar On Chronopharmacokinetics: Visit For More Ppt's & MaterialGANESH KUMAR JELLANo ratings yet
- Lecture 2 Drug Metabolism Phase IIDocument27 pagesLecture 2 Drug Metabolism Phase IIfeegame7No ratings yet
- 1 Principles of Toxicology PDFDocument85 pages1 Principles of Toxicology PDFMariefe BlayaNo ratings yet