Download as ppt, pdf, or txt
You might also like
- Powerpoint AlergyDocument43 pagesPowerpoint AlergywitariNo ratings yet
- SAASP - Pocket Guide To Antibiotic Prescribing For Adults in SA 2015Document60 pagesSAASP - Pocket Guide To Antibiotic Prescribing For Adults in SA 2015PhaimNo ratings yet
- Allergy FDADocument29 pagesAllergy FDASaad Abdul WahabNo ratings yet
- Diaignosis Alergi Blok 20 Maret 2014Document26 pagesDiaignosis Alergi Blok 20 Maret 2014VionNtsNo ratings yet
- Ajol File Journals - 246 - Articles - 170174 - Submission - Proof - 170174 2929 437393 1 10 20180423Document6 pagesAjol File Journals - 246 - Articles - 170174 - Submission - Proof - 170174 2929 437393 1 10 20180423demiana shawkyNo ratings yet
- Pedia - Food AllergyDocument62 pagesPedia - Food Allergyapi-3856051100% (1)
- Referat Alergi Susu SapiDocument20 pagesReferat Alergi Susu Sapibadi akmalNo ratings yet
- Cow Milk AllergyDocument15 pagesCow Milk AllergyAmina Ch100% (1)
- Cows Milk Protein Allergy (CMPA) Road To ManagementDocument66 pagesCows Milk Protein Allergy (CMPA) Road To Managementshalini tanejaNo ratings yet
- Principles of Drug AllergiesDocument31 pagesPrinciples of Drug Allergiesapi-748345558No ratings yet
- Skin Rashes Seen After Eating in A Seafood RestaurantDocument2 pagesSkin Rashes Seen After Eating in A Seafood RestaurantNathaniel SimNo ratings yet
- Jurnal Reading AlergiDocument29 pagesJurnal Reading AlergiRilie ArmeiliaNo ratings yet
- Intolerance ?: Find Out, Order A Test Today!Document7 pagesIntolerance ?: Find Out, Order A Test Today!vyasakandarpNo ratings yet
- Allergy Overview: - Nomenclature - Pathophysiology - Diagnosis - ManagementDocument96 pagesAllergy Overview: - Nomenclature - Pathophysiology - Diagnosis - ManagementPhaimNo ratings yet
- Food Allergy Vs Food Intolerance 1684503076Document33 pagesFood Allergy Vs Food Intolerance 1684503076Kevin AlexNo ratings yet
- Metro Allergy Collateral LBLDocument2 pagesMetro Allergy Collateral LBLSnig KavNo ratings yet
- Skin Prick Testing Guide For GPs NPLDocument5 pagesSkin Prick Testing Guide For GPs NPLniyatihopesNo ratings yet
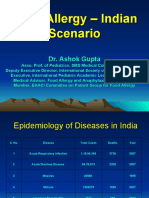
- Food Allergy - Indian ScenarioDocument28 pagesFood Allergy - Indian ScenarioAman BansalNo ratings yet
- Ige-Mediated Cow'S Milk Protein Allergy in Singaporean ChildrenDocument7 pagesIge-Mediated Cow'S Milk Protein Allergy in Singaporean ChildrenZakirNo ratings yet
- Zakiudin Munasir - Food Allergy and ManifestationDocument32 pagesZakiudin Munasir - Food Allergy and ManifestationernitaNo ratings yet
- Food AllergyDocument27 pagesFood AllergyAbabii GhenadieNo ratings yet
- Allergen-Screening 2022Document4 pagesAllergen-Screening 2022Lee SyeNo ratings yet
- Aard 3 139Document6 pagesAard 3 139GinaNo ratings yet
- Food Alergi 13Document58 pagesFood Alergi 13elvira mirandaNo ratings yet
- 16-Food Allergy Arató A.Document39 pages16-Food Allergy Arató A.Gor AdanNo ratings yet
- Appropiate Allergic Testing and The Interpretation - Dr. Deshinta Putri Mulya, SP - PD (K) KAIDocument40 pagesAppropiate Allergic Testing and The Interpretation - Dr. Deshinta Putri Mulya, SP - PD (K) KAIEllenNo ratings yet
- Egg Allergy: Are All Childhood Food Allergies The Same?: Review ArticleDocument6 pagesEgg Allergy: Are All Childhood Food Allergies The Same?: Review ArticlekaяLa яojasNo ratings yet
- A Guide To Performing Skin-Prick Testing in Practice: Tips and Tricks of The TradeDocument5 pagesA Guide To Performing Skin-Prick Testing in Practice: Tips and Tricks of The TradeAningtyas KusumadewiNo ratings yet
- Celiac Disease: DR Ajeet Kumar Lohana Senior Registrar Gastroenterology AtmcDocument59 pagesCeliac Disease: DR Ajeet Kumar Lohana Senior Registrar Gastroenterology AtmcAjeet LohanaNo ratings yet
- Koletzko Allergy Prevention Singapore 2011Document8 pagesKoletzko Allergy Prevention Singapore 2011Enny AndrianiNo ratings yet
- Allergen Detection MethodsDocument16 pagesAllergen Detection MethodsMoch Iqbal SufyanNo ratings yet
- Establishing Food Allergens Thresholds (Simon Brooke-Taylor PHD)Document40 pagesEstablishing Food Allergens Thresholds (Simon Brooke-Taylor PHD)ARdian RizkyNo ratings yet
- Food Allergy-1Document27 pagesFood Allergy-1donald duckNo ratings yet
- Allergy Diagnostics and Treatment 2022Document44 pagesAllergy Diagnostics and Treatment 2022Rohan TejaNo ratings yet
- Allergo-Immunology Hour: Food AllergyDocument32 pagesAllergo-Immunology Hour: Food AllergyJill PNo ratings yet
- Scientific Meetings 012Document1 pageScientific Meetings 012Singey LhendupNo ratings yet
- Pediatric Allergy Immunology - 2020 - Foong - Biomarkers of Diagnosis and Resolution of Food AllergyDocument11 pagesPediatric Allergy Immunology - 2020 - Foong - Biomarkers of Diagnosis and Resolution of Food AllergyAlfred AlfredNo ratings yet
- Food Allergies in Children: DR C Macaulay DR C Lemer DR R BhattDocument11 pagesFood Allergies in Children: DR C Macaulay DR C Lemer DR R BhattSameer KhanNo ratings yet
- Kesler LoganDocument26 pagesKesler Loganapi-648714317No ratings yet
- Factores de Riesgo Asociados Al Diagnóstico de Alergia Al Huevo Ige Mediada en PediatríaDocument4 pagesFactores de Riesgo Asociados Al Diagnóstico de Alergia Al Huevo Ige Mediada en PediatríaDean DaveNo ratings yet
- AR IR by NRDocument96 pagesAR IR by NRnaveen05051996No ratings yet
- Advancements in Diagnostic Tests For Food AlllergensDocument8 pagesAdvancements in Diagnostic Tests For Food Alllergensvspandey27No ratings yet
- Skin TestDocument23 pagesSkin TestpraptiwiNo ratings yet
- Predictive Value of The Sulfi Doleukotriene Release Assay in Oral Allergy Syndrome To Celery, Hazelnut, and CarrotDocument7 pagesPredictive Value of The Sulfi Doleukotriene Release Assay in Oral Allergy Syndrome To Celery, Hazelnut, and CarrotWilly AlendaNo ratings yet
- Allergic RhinitisDocument96 pagesAllergic Rhinitisnaveen05051996No ratings yet
- Food AllergensDocument49 pagesFood AllergensBareera MunirNo ratings yet
- Food Allergy in Children: Hugo Van Bever Department of Pediatrics National University SingaporeDocument30 pagesFood Allergy in Children: Hugo Van Bever Department of Pediatrics National University SingaporeSoni Aditia AbdullahNo ratings yet
- Food Allergies: Annasari MustafaDocument29 pagesFood Allergies: Annasari Mustafanatasya febrianaNo ratings yet
- Food Challenge 03.20.2019Document17 pagesFood Challenge 03.20.2019Emily EresumaNo ratings yet
- Pi Is 0091674903015343Document6 pagesPi Is 0091674903015343anon_213205814No ratings yet
- Main Allergens Diagnosis of Allergic Diseases - Skin Prick Tests 2022Document52 pagesMain Allergens Diagnosis of Allergic Diseases - Skin Prick Tests 2022SePeHR SHNo ratings yet
- Placebo Reactions in Double-Blind, Placebo-Controlled Food Challenges in ChildrenDocument16 pagesPlacebo Reactions in Double-Blind, Placebo-Controlled Food Challenges in ChildrenyuliawatiluthfiNo ratings yet
- How To Optimize Nutrition Management For Allergic Pediatric Patients? Nutrition Point of ViewDocument39 pagesHow To Optimize Nutrition Management For Allergic Pediatric Patients? Nutrition Point of ViewriamamsNo ratings yet
- Smart Antibiotics Use in Children With SBI - HandoutDocument44 pagesSmart Antibiotics Use in Children With SBI - HandoutAlbertNo ratings yet
- Food Safety Training - UpdatedDocument37 pagesFood Safety Training - UpdatedAdrienne IngramNo ratings yet
- Atopic Dermatitis and Allergies: Pediatric & Gastrointestinal PerspectiveDocument25 pagesAtopic Dermatitis and Allergies: Pediatric & Gastrointestinal PerspectiveHeni PurwaningsihNo ratings yet
- Allergy: RecallDocument5 pagesAllergy: RecallNatalie LiNo ratings yet
- 802 1860 1 SMDocument6 pages802 1860 1 SMEmilEmsNo ratings yet
- Managing Cows' Milk Allergy in Children: Sian Ludman, Neil Shah, Adam T FoxDocument5 pagesManaging Cows' Milk Allergy in Children: Sian Ludman, Neil Shah, Adam T FoxSaha SampeanNo ratings yet
- All About Allergens Brochure FA PDFDocument9 pagesAll About Allergens Brochure FA PDFМиша МакухNo ratings yet
- Restart Collaboration - Effects of Antiplatelet Therapy After Stroke Due To Intracerebral Haemorrhage (RESTART) - OriginalDocument11 pagesRestart Collaboration - Effects of Antiplatelet Therapy After Stroke Due To Intracerebral Haemorrhage (RESTART) - OriginalPhaimNo ratings yet
- Beneteau-Burnat B - Serum ACE in Healthy and Sarcoidotic Children - Comparison With Reference Intervals For AdultsDocument3 pagesBeneteau-Burnat B - Serum ACE in Healthy and Sarcoidotic Children - Comparison With Reference Intervals For AdultsPhaimNo ratings yet
- Beneficial Ownership TemplateDocument69 pagesBeneficial Ownership TemplatePhaimNo ratings yet
- Mlxtran: The Model Coding Language For - MonolixDocument40 pagesMlxtran: The Model Coding Language For - MonolixPhaimNo ratings yet
- Hodson G - Methanol in WineDocument5 pagesHodson G - Methanol in WinePhaimNo ratings yet
- Antibiotic Stewardship and Returning Travellers For 6 YearsDocument123 pagesAntibiotic Stewardship and Returning Travellers For 6 YearsPhaimNo ratings yet
- Xie J - Evaluating The Intoxicating Degree of Liquor Products With Combinations of Fusel Alcohols, Acids & EstersDocument12 pagesXie J - Evaluating The Intoxicating Degree of Liquor Products With Combinations of Fusel Alcohols, Acids & EstersPhaimNo ratings yet
- Clinical Aspects of Palliative CareDocument71 pagesClinical Aspects of Palliative CarePhaimNo ratings yet
- Cardiac Arrhythmias 6th YearDocument108 pagesCardiac Arrhythmias 6th YearPhaimNo ratings yet
- Asthma, A Practical GuideDocument61 pagesAsthma, A Practical GuidePhaimNo ratings yet
- Clinical Immunology in Practise 2013 - 6th Years - Vula - 17mayDocument72 pagesClinical Immunology in Practise 2013 - 6th Years - Vula - 17mayPhaimNo ratings yet
- Approach To Neurological EmergenciesMAY2013Document69 pagesApproach To Neurological EmergenciesMAY2013PhaimNo ratings yet
- Drug Resistant TB - What Every Student Should Know: Elma de VriesDocument30 pagesDrug Resistant TB - What Every Student Should Know: Elma de VriesPhaimNo ratings yet
- Cerebral Palsy: C. AdnamsDocument54 pagesCerebral Palsy: C. AdnamsPhaimNo ratings yet
- Social Grants: Elma de Vries Division of Family MedicineDocument35 pagesSocial Grants: Elma de Vries Division of Family MedicinePhaimNo ratings yet
- Allergy Overview: - Nomenclature - Pathophysiology - Diagnosis - ManagementDocument96 pagesAllergy Overview: - Nomenclature - Pathophysiology - Diagnosis - ManagementPhaimNo ratings yet
- OPie HIV and Cytopenias, 2013 6th YrsDocument30 pagesOPie HIV and Cytopenias, 2013 6th YrsPhaimNo ratings yet
- OT Lecture HIV and Mental Health - No PicsDocument28 pagesOT Lecture HIV and Mental Health - No PicsPhaimNo ratings yet
- Paediatric Palliative CareDocument38 pagesPaediatric Palliative CarePhaimNo ratings yet
- Psychosocial Guidelines 2012-1Document20 pagesPsychosocial Guidelines 2012-1PhaimNo ratings yet
- Overdose & PoisoningDocument56 pagesOverdose & PoisoningPhaimNo ratings yet
- DR Peter Smith OT II - May 2012Document23 pagesDR Peter Smith OT II - May 2012PhaimNo ratings yet
- Drug Information Handbook 17 Edition, Lexi-Comp For The AmericanDocument4 pagesDrug Information Handbook 17 Edition, Lexi-Comp For The AmericanVerina Widianti PutriNo ratings yet
- Shamsuddin - Prevention of PE E Including Community Level Intervention in BangladeshDocument26 pagesShamsuddin - Prevention of PE E Including Community Level Intervention in BangladeshDhaka2012No ratings yet
- Postnatal Care PDF 66142082148037Document64 pagesPostnatal Care PDF 66142082148037veronia widayantiNo ratings yet
- Neurological Disorders Practice Test QuestionsDocument6 pagesNeurological Disorders Practice Test QuestionsBenedict AlvarezNo ratings yet
- Cwu Ong TwinDocument14 pagesCwu Ong TwinAiman ArifinNo ratings yet
- Intrahepatic Cholestasis of PregnancyDocument19 pagesIntrahepatic Cholestasis of PregnancyAlexander Vasquez TorresNo ratings yet
- Anes Drugs TableDocument20 pagesAnes Drugs TableKathleen Grace ManiagoNo ratings yet
- Ecografo Aloka Modelo SSD-3500Document34 pagesEcografo Aloka Modelo SSD-3500EmilioPerezBallesterosNo ratings yet
- Nurs 3021 Reflective JournalDocument6 pagesNurs 3021 Reflective Journalapi-487456788No ratings yet
- Research ProposalDocument9 pagesResearch ProposalAbiola IbrahimNo ratings yet
- Noor Msallaty - 8 Pages of Research PaperDocument16 pagesNoor Msallaty - 8 Pages of Research Paperapi-445615356No ratings yet
- Makalah Bahasa Inggris FixDocument8 pagesMakalah Bahasa Inggris FixNila SarikkNo ratings yet
- Surgery 5th SEM MCQs AnsDocument75 pagesSurgery 5th SEM MCQs Anskthangjam21No ratings yet
- Use SimbicortDocument5 pagesUse SimbicortScholastica MaharaniNo ratings yet
- Tool and Resource Evaluation TemplateDocument4 pagesTool and Resource Evaluation Templatetimie_reyesNo ratings yet
- Gold Guidelines 2014 PDFDocument3 pagesGold Guidelines 2014 PDFKhalidNo ratings yet
- Recognized By:: MNR Homoeopathic Medical College & Hospital, SangareddyDocument21 pagesRecognized By:: MNR Homoeopathic Medical College & Hospital, SangareddyJahnaveeNo ratings yet
- General AnesthesiaDocument11 pagesGeneral AnesthesiaGERSON RYANTONo ratings yet
- TYRX BrochureDocument28 pagesTYRX Brochureleo chiuNo ratings yet
- Kitir Proposal Penelitian 2014 SIDocument32 pagesKitir Proposal Penelitian 2014 SIclarazettiraNo ratings yet
- Final Supply of Books PDFDocument49 pagesFinal Supply of Books PDFVijay SharmaNo ratings yet
- Cardinal SantosDocument1 pageCardinal SantosCherry EstradaNo ratings yet
- Pharmacoeconomics - Part IIDocument43 pagesPharmacoeconomics - Part IISima JabbariNo ratings yet
- Coronary Slow FlowDocument7 pagesCoronary Slow FlowradiomedicNo ratings yet
- HMIS User ManualDocument89 pagesHMIS User ManualDelelegn EmwodewNo ratings yet
- PATENT Annexure-A Domestic FilingDocument24 pagesPATENT Annexure-A Domestic FilingMulayam Singh YadavNo ratings yet
- Sistematik ReviewDocument8 pagesSistematik ReviewHesmi Rahmawati100% (1)
- Complete Repertory 2017 Rev I Info SheetDocument2 pagesComplete Repertory 2017 Rev I Info SheetSohail LatifNo ratings yet
- RoilsDocument4 pagesRoilsapi-585462575No ratings yet
- Journals-2 PDFDocument280 pagesJournals-2 PDFBhupendra Singh100% (1)