
Farmakologi Sindrom Metablik Citra
Farmakologi Sindrom Metablik Citra
You might also like
- S.T.E.M Education Strategies For Teachin PDFDocument249 pagesS.T.E.M Education Strategies For Teachin PDFRian100% (3)
- Department of Medicine: Presented byDocument50 pagesDepartment of Medicine: Presented byArsh Surendra SinghNo ratings yet
- Metabolic Syndrome: Dr. Bratasena Mkedpd, SPPD Dept. of Internal Medicine Medical Faculty of Batam UniversityDocument46 pagesMetabolic Syndrome: Dr. Bratasena Mkedpd, SPPD Dept. of Internal Medicine Medical Faculty of Batam UniversityFitri Rahmayani100% (1)
- Metabolic Syndrome: Dr. Bratasena Mkedpd, SPPD Dept. of Internal Medicine Rs Budi Kemuliaan BatamDocument46 pagesMetabolic Syndrome: Dr. Bratasena Mkedpd, SPPD Dept. of Internal Medicine Rs Budi Kemuliaan BatamAnnisa Syafei100% (1)
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodDocument62 pagesCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaNo ratings yet
- Dyslipedemia ShortDocument5 pagesDyslipedemia Shortذوالفقار أحمدNo ratings yet
- Division of Endocrinology and Metabolism Department of Internal Medicine Faculty of Medicine University of Sebelas Maret SurakartaDocument51 pagesDivision of Endocrinology and Metabolism Department of Internal Medicine Faculty of Medicine University of Sebelas Maret SurakartaDeboraMargaPangestikaNo ratings yet
- Metabolic Syndrome - ClinicalKeyDocument7 pagesMetabolic Syndrome - ClinicalKeyJairo Vergara CorenaNo ratings yet
- Metabolic Syndrome JhdjkwhekuhfdhjkewDocument48 pagesMetabolic Syndrome Jhdjkwhekuhfdhjkewkiki luhita sariNo ratings yet
- ENDO - Metabolic SyndromeDocument3 pagesENDO - Metabolic SyndromeHajime NakaegawaNo ratings yet
- Syndrome X (High Risk For CHD)Document4 pagesSyndrome X (High Risk For CHD)Hendricus Novaldo Widodo PutraNo ratings yet
- HyperlipidemiaDocument38 pagesHyperlipidemiaAadhan ArveeNo ratings yet
- Management of Dyslipidemia and The Prevention of Cardiovascular DiseaseDocument2 pagesManagement of Dyslipidemia and The Prevention of Cardiovascular DiseaseBenny TrisaktyariNo ratings yet
- Metabolic DR - RehabDocument24 pagesMetabolic DR - RehabMohammed Saad NabhanNo ratings yet
- Saint Louis University College of Nursing Baguio CityDocument10 pagesSaint Louis University College of Nursing Baguio CityrenleanNo ratings yet
- 2nd Case Session ToT CPG HPTDocument127 pages2nd Case Session ToT CPG HPThakimahsNo ratings yet
- Summary of IMBR-Saud Alzahrani-08-2020Document30 pagesSummary of IMBR-Saud Alzahrani-08-2020AHMAD ALROWAILYNo ratings yet
- Clinical Practice Guidelines For Diabetes ManagementDocument5 pagesClinical Practice Guidelines For Diabetes ManagementIqbal Fida MaulanaNo ratings yet
- Case Study 4Document14 pagesCase Study 4api-437387942No ratings yet
- Hyprlipdemia 2020 4th EditionDocument24 pagesHyprlipdemia 2020 4th EditionLillian KrazemNo ratings yet
- 2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"Document51 pages2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"dr_yasserNo ratings yet
- Metabolic Syndrome: Denz Marc Ray T. Alea First Year ResidentDocument38 pagesMetabolic Syndrome: Denz Marc Ray T. Alea First Year ResidentDenz Marc Ray Alea100% (2)
- Clinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Document61 pagesClinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Bassant Ahmed Mahmoud Ragab Abdallah AyaadNo ratings yet
- DD Metabolic SyndromeDocument5 pagesDD Metabolic SyndromeEluNo ratings yet
- Dyslipidemia: Signs and SymptomsDocument24 pagesDyslipidemia: Signs and Symptomschrissanto chandraNo ratings yet
- Diabetes: in All Asymptomatic People Whose Initial Result Suggests A Diagnosis of Diabetes, A ConfirmatoryDocument3 pagesDiabetes: in All Asymptomatic People Whose Initial Result Suggests A Diagnosis of Diabetes, A ConfirmatorytothomileNo ratings yet
- Metabolic Syndrome - Overview and Current GuidelinesDocument12 pagesMetabolic Syndrome - Overview and Current GuidelinessserggiosNo ratings yet
- Causes & Prevention of Coronary Artery DiseaseDocument41 pagesCauses & Prevention of Coronary Artery DiseaseeenagpurcongNo ratings yet
- From This Age in What Patient Group? Start Screening For With Test FrequencyDocument7 pagesFrom This Age in What Patient Group? Start Screening For With Test Frequencyphoenix24601No ratings yet
- Alanine Aminotransferase Alt, GPT, SGPT: Iu/L Kat/lDocument8 pagesAlanine Aminotransferase Alt, GPT, SGPT: Iu/L Kat/lLuis Ferdinand Dacera-Gabronino Gamponia-NonanNo ratings yet
- At OvaDocument5 pagesAt OvaA B Siddiq MizanNo ratings yet
- DiabetesDocument11 pagesDiabetestasneem.salah92No ratings yet
- 10SindromeMeta2006 PDFDocument16 pages10SindromeMeta2006 PDFChristian Eliud Galindo SalazarNo ratings yet
- 10SindromeMeta2006 PDFDocument16 pages10SindromeMeta2006 PDFChristian Eliud Galindo SalazarNo ratings yet
- Diabetes Case PresentationDocument3 pagesDiabetes Case Presentationdeb haart100% (1)
- Diabetes Mellitus CPGDocument90 pagesDiabetes Mellitus CPGKristine-Joy Legaspi FrancoNo ratings yet
- Prof Salman 12 Feb 2015Document25 pagesProf Salman 12 Feb 2015untia_sariNo ratings yet
- Metabolic Syndrome: Internal Medicine Departement MF Gmu/Sardjito Hospital YogyakartaDocument53 pagesMetabolic Syndrome: Internal Medicine Departement MF Gmu/Sardjito Hospital YogyakartaJipeeZed100% (1)
- LipidsupdateDocument23 pagesLipidsupdatedrshekarforyouNo ratings yet
- Term Metabolic Syndrome and Common Cause: Hipertensi ObesitasDocument5 pagesTerm Metabolic Syndrome and Common Cause: Hipertensi ObesitasJohanna FreddaNo ratings yet
- MetabolicsyndDocument37 pagesMetabolicsyndShanooha MansoorNo ratings yet
- Presentation On CHEMICALDocument12 pagesPresentation On CHEMICALOkpetah Chioma christabelNo ratings yet
- Screening and Management of Lipids: Patient Population: ObjectiveDocument20 pagesScreening and Management of Lipids: Patient Population: ObjectiveKatie Kroll BradyNo ratings yet
- Met 2008 0065 PDFDocument10 pagesMet 2008 0065 PDFDeedee RenovaldiNo ratings yet
- Hyperlipidemia: Brian V. Reamy, MD, Colonel, USAF, MC Chair - Department of Family Medicine Uniformed Services UniversityDocument58 pagesHyperlipidemia: Brian V. Reamy, MD, Colonel, USAF, MC Chair - Department of Family Medicine Uniformed Services Universityayloleh87No ratings yet
- Hyperlipidemia: Revised: October 4, 2019Document7 pagesHyperlipidemia: Revised: October 4, 2019HannaNo ratings yet
- Dyslipidemia ATP4 GUIDLINESDocument9 pagesDyslipidemia ATP4 GUIDLINESSandy GunawanNo ratings yet
- Dyslipidemia: Dr. Sohail AhmadDocument36 pagesDyslipidemia: Dr. Sohail AhmadChong Zhi LinNo ratings yet
- NON Communicable DiseasesDocument45 pagesNON Communicable DiseaseshemihemaNo ratings yet
- Clinic Running QuestionsDocument8 pagesClinic Running QuestionsDraykidNo ratings yet
- Hypertension in Special Population.Document25 pagesHypertension in Special Population.Anamta AshfaqNo ratings yet
- ATP IV HandoutDocument2 pagesATP IV Handouthafidzz1No ratings yet
- Hypertension & Diabetis MellitusDocument51 pagesHypertension & Diabetis MellitusSuma_Ramesan_5373100% (1)
- The Metabolic Syndrome-From Insulin Resistance To Obesity and DiabetesDocument19 pagesThe Metabolic Syndrome-From Insulin Resistance To Obesity and DiabetesLucho FerroNo ratings yet
- Metabolic Syndrome: SMF Ilmu Penyakit Dalam RSD Gunung Jati Kota CirebonDocument50 pagesMetabolic Syndrome: SMF Ilmu Penyakit Dalam RSD Gunung Jati Kota CirebonFina Sudarni SNo ratings yet
- Diabetes Mellitus in PediatricsDocument22 pagesDiabetes Mellitus in PediatricsKermaigne MirandaNo ratings yet
- Pediatric Patients (10-17 Years of Age)Document18 pagesPediatric Patients (10-17 Years of Age)asdwasdNo ratings yet
- Li 2017Document32 pagesLi 2017akshayNo ratings yet
- Sindrome Metabolico Med - Clin - North - Am 2011Document19 pagesSindrome Metabolico Med - Clin - North - Am 2011saraNo ratings yet
- Metabolic Syndrome Program: How to Lose Weight, Beat Heart Disease, Stop Insulin Resistance and MoreFrom EverandMetabolic Syndrome Program: How to Lose Weight, Beat Heart Disease, Stop Insulin Resistance and MoreRating: 4.5 out of 5 stars4.5/5 (2)
- Guidelines For PCB Layout DesignDocument5 pagesGuidelines For PCB Layout DesigncooksandNo ratings yet
- Individual Health Insurance Policy CISDocument3 pagesIndividual Health Insurance Policy CISGIJONo ratings yet
- 5 ElementosDocument3 pages5 ElementosHectorNo ratings yet
- Death RoadDocument12 pagesDeath RoadRodrigo Salgueiro LlanosNo ratings yet
- Liceo de Cagayan University Senior High School Department The Problem and Its ScopeDocument21 pagesLiceo de Cagayan University Senior High School Department The Problem and Its ScopeShane Khezia Abriol BaclayonNo ratings yet
- How To Hire, Manage, and Terminate Employees by Thomas Y. Mandler, Jennifer M. BallardDocument75 pagesHow To Hire, Manage, and Terminate Employees by Thomas Y. Mandler, Jennifer M. Ballardhuzefa7barodawalaNo ratings yet
- Open2023 OpenDocument13 pagesOpen2023 Openipsita lahiriNo ratings yet
- Capgemini Excelity Payroll FAQDocument16 pagesCapgemini Excelity Payroll FAQAbhijitNo ratings yet
- Lesson Plan 8 Supermarket ShopDocument10 pagesLesson Plan 8 Supermarket ShopJo GregoryNo ratings yet
- Refractory: Zoning of Kilns and Brick SelectionDocument26 pagesRefractory: Zoning of Kilns and Brick Selectionrupesh soni100% (2)
- Experiment 13 Ultrafiltration UnitDocument13 pagesExperiment 13 Ultrafiltration UnitKishen NaniNo ratings yet
- EpitheliumDocument48 pagesEpitheliumdrpankaj28100% (1)
- Soy Source: Polarity TherapyDocument2 pagesSoy Source: Polarity TherapyrooNo ratings yet
- REHS4987-02 Replacing Base Edge Assemblies in Large Wheel Loader BucketsDocument19 pagesREHS4987-02 Replacing Base Edge Assemblies in Large Wheel Loader BucketsCarlosNo ratings yet
- Cost of The DietDocument68 pagesCost of The DietSomao JoeNo ratings yet
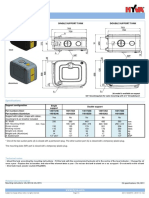
- Hyva Oil Tank: Single Support Tank Double Support TankDocument4 pagesHyva Oil Tank: Single Support Tank Double Support TankPutera Bumi NusantaraNo ratings yet
- Presentation - Education in EmergenciesDocument30 pagesPresentation - Education in EmergenciesSHERYL WYCOCONo ratings yet
- Agrismart's Farm Water Solution An Alternative To Mains WaterDocument3 pagesAgrismart's Farm Water Solution An Alternative To Mains WaterPR.comNo ratings yet
- Managing People - AssignmentDocument10 pagesManaging People - AssignmentayeshaNo ratings yet
- From Gathering To Growing Food: Neinuo's LunchDocument10 pagesFrom Gathering To Growing Food: Neinuo's Lunchsoumya KavdiaNo ratings yet
- Top 10 Tips From ZOE Science and NutritionDocument5 pagesTop 10 Tips From ZOE Science and NutritionGabaNo ratings yet
- Gas Pressure Regulator Series 240Pl: Serving The Gas Industry WorldwideDocument11 pagesGas Pressure Regulator Series 240Pl: Serving The Gas Industry WorldwideSandro RuizNo ratings yet
- 11 SMAW Q4 Module 2Document11 pages11 SMAW Q4 Module 2Mark Johnson VillaronNo ratings yet
- Gerby - RAHA CaresDocument4 pagesGerby - RAHA CaresGerard CariñoNo ratings yet
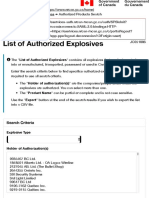
- NRCan's Explosives Eservices - Authorized Products SearchDocument5 pagesNRCan's Explosives Eservices - Authorized Products SearchDiego VilaNo ratings yet
- Ke-45-Ts Sds JPN EngDocument9 pagesKe-45-Ts Sds JPN Engsouradeepmukherjee20No ratings yet
- RisCo Firme Nou Infiintate 20190429Document127 pagesRisCo Firme Nou Infiintate 20190429Gazeta de MâineNo ratings yet
- FingerprintingDocument36 pagesFingerprintingapi-291003259100% (2)
- Desoldering Tool: Designed For Lead FreeDocument2 pagesDesoldering Tool: Designed For Lead FreeMarco Antonio Ortiz RomeroNo ratings yet
























































































Download as pptx, pdf, or txt
You might also like
- S.T.E.M Education Strategies For Teachin PDFDocument249 pagesS.T.E.M Education Strategies For Teachin PDFRian100% (3)
- Department of Medicine: Presented byDocument50 pagesDepartment of Medicine: Presented byArsh Surendra SinghNo ratings yet
- Metabolic Syndrome: Dr. Bratasena Mkedpd, SPPD Dept. of Internal Medicine Medical Faculty of Batam UniversityDocument46 pagesMetabolic Syndrome: Dr. Bratasena Mkedpd, SPPD Dept. of Internal Medicine Medical Faculty of Batam UniversityFitri Rahmayani100% (1)
- Metabolic Syndrome: Dr. Bratasena Mkedpd, SPPD Dept. of Internal Medicine Rs Budi Kemuliaan BatamDocument46 pagesMetabolic Syndrome: Dr. Bratasena Mkedpd, SPPD Dept. of Internal Medicine Rs Budi Kemuliaan BatamAnnisa Syafei100% (1)
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodDocument62 pagesCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaNo ratings yet
- Dyslipedemia ShortDocument5 pagesDyslipedemia Shortذوالفقار أحمدNo ratings yet
- Division of Endocrinology and Metabolism Department of Internal Medicine Faculty of Medicine University of Sebelas Maret SurakartaDocument51 pagesDivision of Endocrinology and Metabolism Department of Internal Medicine Faculty of Medicine University of Sebelas Maret SurakartaDeboraMargaPangestikaNo ratings yet
- Metabolic Syndrome - ClinicalKeyDocument7 pagesMetabolic Syndrome - ClinicalKeyJairo Vergara CorenaNo ratings yet
- Metabolic Syndrome JhdjkwhekuhfdhjkewDocument48 pagesMetabolic Syndrome Jhdjkwhekuhfdhjkewkiki luhita sariNo ratings yet
- ENDO - Metabolic SyndromeDocument3 pagesENDO - Metabolic SyndromeHajime NakaegawaNo ratings yet
- Syndrome X (High Risk For CHD)Document4 pagesSyndrome X (High Risk For CHD)Hendricus Novaldo Widodo PutraNo ratings yet
- HyperlipidemiaDocument38 pagesHyperlipidemiaAadhan ArveeNo ratings yet
- Management of Dyslipidemia and The Prevention of Cardiovascular DiseaseDocument2 pagesManagement of Dyslipidemia and The Prevention of Cardiovascular DiseaseBenny TrisaktyariNo ratings yet
- Metabolic DR - RehabDocument24 pagesMetabolic DR - RehabMohammed Saad NabhanNo ratings yet
- Saint Louis University College of Nursing Baguio CityDocument10 pagesSaint Louis University College of Nursing Baguio CityrenleanNo ratings yet
- 2nd Case Session ToT CPG HPTDocument127 pages2nd Case Session ToT CPG HPThakimahsNo ratings yet
- Summary of IMBR-Saud Alzahrani-08-2020Document30 pagesSummary of IMBR-Saud Alzahrani-08-2020AHMAD ALROWAILYNo ratings yet
- Clinical Practice Guidelines For Diabetes ManagementDocument5 pagesClinical Practice Guidelines For Diabetes ManagementIqbal Fida MaulanaNo ratings yet
- Case Study 4Document14 pagesCase Study 4api-437387942No ratings yet
- Hyprlipdemia 2020 4th EditionDocument24 pagesHyprlipdemia 2020 4th EditionLillian KrazemNo ratings yet
- 2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"Document51 pages2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"dr_yasserNo ratings yet
- Metabolic Syndrome: Denz Marc Ray T. Alea First Year ResidentDocument38 pagesMetabolic Syndrome: Denz Marc Ray T. Alea First Year ResidentDenz Marc Ray Alea100% (2)
- Clinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Document61 pagesClinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Bassant Ahmed Mahmoud Ragab Abdallah AyaadNo ratings yet
- DD Metabolic SyndromeDocument5 pagesDD Metabolic SyndromeEluNo ratings yet
- Dyslipidemia: Signs and SymptomsDocument24 pagesDyslipidemia: Signs and Symptomschrissanto chandraNo ratings yet
- Diabetes: in All Asymptomatic People Whose Initial Result Suggests A Diagnosis of Diabetes, A ConfirmatoryDocument3 pagesDiabetes: in All Asymptomatic People Whose Initial Result Suggests A Diagnosis of Diabetes, A ConfirmatorytothomileNo ratings yet
- Metabolic Syndrome - Overview and Current GuidelinesDocument12 pagesMetabolic Syndrome - Overview and Current GuidelinessserggiosNo ratings yet
- Causes & Prevention of Coronary Artery DiseaseDocument41 pagesCauses & Prevention of Coronary Artery DiseaseeenagpurcongNo ratings yet
- From This Age in What Patient Group? Start Screening For With Test FrequencyDocument7 pagesFrom This Age in What Patient Group? Start Screening For With Test Frequencyphoenix24601No ratings yet
- Alanine Aminotransferase Alt, GPT, SGPT: Iu/L Kat/lDocument8 pagesAlanine Aminotransferase Alt, GPT, SGPT: Iu/L Kat/lLuis Ferdinand Dacera-Gabronino Gamponia-NonanNo ratings yet
- At OvaDocument5 pagesAt OvaA B Siddiq MizanNo ratings yet
- DiabetesDocument11 pagesDiabetestasneem.salah92No ratings yet
- 10SindromeMeta2006 PDFDocument16 pages10SindromeMeta2006 PDFChristian Eliud Galindo SalazarNo ratings yet
- 10SindromeMeta2006 PDFDocument16 pages10SindromeMeta2006 PDFChristian Eliud Galindo SalazarNo ratings yet
- Diabetes Case PresentationDocument3 pagesDiabetes Case Presentationdeb haart100% (1)
- Diabetes Mellitus CPGDocument90 pagesDiabetes Mellitus CPGKristine-Joy Legaspi FrancoNo ratings yet
- Prof Salman 12 Feb 2015Document25 pagesProf Salman 12 Feb 2015untia_sariNo ratings yet
- Metabolic Syndrome: Internal Medicine Departement MF Gmu/Sardjito Hospital YogyakartaDocument53 pagesMetabolic Syndrome: Internal Medicine Departement MF Gmu/Sardjito Hospital YogyakartaJipeeZed100% (1)
- LipidsupdateDocument23 pagesLipidsupdatedrshekarforyouNo ratings yet
- Term Metabolic Syndrome and Common Cause: Hipertensi ObesitasDocument5 pagesTerm Metabolic Syndrome and Common Cause: Hipertensi ObesitasJohanna FreddaNo ratings yet
- MetabolicsyndDocument37 pagesMetabolicsyndShanooha MansoorNo ratings yet
- Presentation On CHEMICALDocument12 pagesPresentation On CHEMICALOkpetah Chioma christabelNo ratings yet
- Screening and Management of Lipids: Patient Population: ObjectiveDocument20 pagesScreening and Management of Lipids: Patient Population: ObjectiveKatie Kroll BradyNo ratings yet
- Met 2008 0065 PDFDocument10 pagesMet 2008 0065 PDFDeedee RenovaldiNo ratings yet
- Hyperlipidemia: Brian V. Reamy, MD, Colonel, USAF, MC Chair - Department of Family Medicine Uniformed Services UniversityDocument58 pagesHyperlipidemia: Brian V. Reamy, MD, Colonel, USAF, MC Chair - Department of Family Medicine Uniformed Services Universityayloleh87No ratings yet
- Hyperlipidemia: Revised: October 4, 2019Document7 pagesHyperlipidemia: Revised: October 4, 2019HannaNo ratings yet
- Dyslipidemia ATP4 GUIDLINESDocument9 pagesDyslipidemia ATP4 GUIDLINESSandy GunawanNo ratings yet
- Dyslipidemia: Dr. Sohail AhmadDocument36 pagesDyslipidemia: Dr. Sohail AhmadChong Zhi LinNo ratings yet
- NON Communicable DiseasesDocument45 pagesNON Communicable DiseaseshemihemaNo ratings yet
- Clinic Running QuestionsDocument8 pagesClinic Running QuestionsDraykidNo ratings yet
- Hypertension in Special Population.Document25 pagesHypertension in Special Population.Anamta AshfaqNo ratings yet
- ATP IV HandoutDocument2 pagesATP IV Handouthafidzz1No ratings yet
- Hypertension & Diabetis MellitusDocument51 pagesHypertension & Diabetis MellitusSuma_Ramesan_5373100% (1)
- The Metabolic Syndrome-From Insulin Resistance To Obesity and DiabetesDocument19 pagesThe Metabolic Syndrome-From Insulin Resistance To Obesity and DiabetesLucho FerroNo ratings yet
- Metabolic Syndrome: SMF Ilmu Penyakit Dalam RSD Gunung Jati Kota CirebonDocument50 pagesMetabolic Syndrome: SMF Ilmu Penyakit Dalam RSD Gunung Jati Kota CirebonFina Sudarni SNo ratings yet
- Diabetes Mellitus in PediatricsDocument22 pagesDiabetes Mellitus in PediatricsKermaigne MirandaNo ratings yet
- Pediatric Patients (10-17 Years of Age)Document18 pagesPediatric Patients (10-17 Years of Age)asdwasdNo ratings yet
- Li 2017Document32 pagesLi 2017akshayNo ratings yet
- Sindrome Metabolico Med - Clin - North - Am 2011Document19 pagesSindrome Metabolico Med - Clin - North - Am 2011saraNo ratings yet
- Metabolic Syndrome Program: How to Lose Weight, Beat Heart Disease, Stop Insulin Resistance and MoreFrom EverandMetabolic Syndrome Program: How to Lose Weight, Beat Heart Disease, Stop Insulin Resistance and MoreRating: 4.5 out of 5 stars4.5/5 (2)
- Guidelines For PCB Layout DesignDocument5 pagesGuidelines For PCB Layout DesigncooksandNo ratings yet
- Individual Health Insurance Policy CISDocument3 pagesIndividual Health Insurance Policy CISGIJONo ratings yet
- 5 ElementosDocument3 pages5 ElementosHectorNo ratings yet
- Death RoadDocument12 pagesDeath RoadRodrigo Salgueiro LlanosNo ratings yet
- Liceo de Cagayan University Senior High School Department The Problem and Its ScopeDocument21 pagesLiceo de Cagayan University Senior High School Department The Problem and Its ScopeShane Khezia Abriol BaclayonNo ratings yet
- How To Hire, Manage, and Terminate Employees by Thomas Y. Mandler, Jennifer M. BallardDocument75 pagesHow To Hire, Manage, and Terminate Employees by Thomas Y. Mandler, Jennifer M. Ballardhuzefa7barodawalaNo ratings yet
- Open2023 OpenDocument13 pagesOpen2023 Openipsita lahiriNo ratings yet
- Capgemini Excelity Payroll FAQDocument16 pagesCapgemini Excelity Payroll FAQAbhijitNo ratings yet
- Lesson Plan 8 Supermarket ShopDocument10 pagesLesson Plan 8 Supermarket ShopJo GregoryNo ratings yet
- Refractory: Zoning of Kilns and Brick SelectionDocument26 pagesRefractory: Zoning of Kilns and Brick Selectionrupesh soni100% (2)
- Experiment 13 Ultrafiltration UnitDocument13 pagesExperiment 13 Ultrafiltration UnitKishen NaniNo ratings yet
- EpitheliumDocument48 pagesEpitheliumdrpankaj28100% (1)
- Soy Source: Polarity TherapyDocument2 pagesSoy Source: Polarity TherapyrooNo ratings yet
- REHS4987-02 Replacing Base Edge Assemblies in Large Wheel Loader BucketsDocument19 pagesREHS4987-02 Replacing Base Edge Assemblies in Large Wheel Loader BucketsCarlosNo ratings yet
- Cost of The DietDocument68 pagesCost of The DietSomao JoeNo ratings yet
- Hyva Oil Tank: Single Support Tank Double Support TankDocument4 pagesHyva Oil Tank: Single Support Tank Double Support TankPutera Bumi NusantaraNo ratings yet
- Presentation - Education in EmergenciesDocument30 pagesPresentation - Education in EmergenciesSHERYL WYCOCONo ratings yet
- Agrismart's Farm Water Solution An Alternative To Mains WaterDocument3 pagesAgrismart's Farm Water Solution An Alternative To Mains WaterPR.comNo ratings yet
- Managing People - AssignmentDocument10 pagesManaging People - AssignmentayeshaNo ratings yet
- From Gathering To Growing Food: Neinuo's LunchDocument10 pagesFrom Gathering To Growing Food: Neinuo's Lunchsoumya KavdiaNo ratings yet
- Top 10 Tips From ZOE Science and NutritionDocument5 pagesTop 10 Tips From ZOE Science and NutritionGabaNo ratings yet
- Gas Pressure Regulator Series 240Pl: Serving The Gas Industry WorldwideDocument11 pagesGas Pressure Regulator Series 240Pl: Serving The Gas Industry WorldwideSandro RuizNo ratings yet
- 11 SMAW Q4 Module 2Document11 pages11 SMAW Q4 Module 2Mark Johnson VillaronNo ratings yet
- Gerby - RAHA CaresDocument4 pagesGerby - RAHA CaresGerard CariñoNo ratings yet
- NRCan's Explosives Eservices - Authorized Products SearchDocument5 pagesNRCan's Explosives Eservices - Authorized Products SearchDiego VilaNo ratings yet
- Ke-45-Ts Sds JPN EngDocument9 pagesKe-45-Ts Sds JPN Engsouradeepmukherjee20No ratings yet
- RisCo Firme Nou Infiintate 20190429Document127 pagesRisCo Firme Nou Infiintate 20190429Gazeta de MâineNo ratings yet
- FingerprintingDocument36 pagesFingerprintingapi-291003259100% (2)
- Desoldering Tool: Designed For Lead FreeDocument2 pagesDesoldering Tool: Designed For Lead FreeMarco Antonio Ortiz RomeroNo ratings yet