
Estorgen
Estorgen
You might also like
- Revised New PTLLS Assignment 1 Levels 3 and 4 Nov 2011Document3 pagesRevised New PTLLS Assignment 1 Levels 3 and 4 Nov 2011dave_perry189218No ratings yet
- Pharm Shelf Big Boss Review Aka Pharmacology Shelf Study GuideDocument13 pagesPharm Shelf Big Boss Review Aka Pharmacology Shelf Study Guideemceelee100% (2)
- Starbucks - Targetting, Positioning and Marketing MixDocument7 pagesStarbucks - Targetting, Positioning and Marketing MixSreerag Gangadharan89% (19)
- Properties of Standard AtmosphereDocument6 pagesProperties of Standard AtmosphereErnesto D. AguirreNo ratings yet
- Drugs Affecting Reproduction: DR - R - PrameelaDocument76 pagesDrugs Affecting Reproduction: DR - R - PrameelaRamadi PrameelaNo ratings yet
- Steroids JenniferKettelDocument25 pagesSteroids JenniferKettelvinay0717No ratings yet
- Sex HarmoneDocument22 pagesSex Harmonesuyash jainNo ratings yet
- New Estrogen and ProgesteroneDocument56 pagesNew Estrogen and ProgesteroneHBr100% (1)
- Drugs Used in Reproductive Health: Estrogen and ProgestinDocument41 pagesDrugs Used in Reproductive Health: Estrogen and ProgestindrfatimarizNo ratings yet
- Gonadal Hormones 62594Document98 pagesGonadal Hormones 62594TES SENNo ratings yet
- Oestrogen, Progesterone, AndrogensDocument58 pagesOestrogen, Progesterone, AndrogensTandin Sonam100% (1)
- Sex Hormones PDFDocument54 pagesSex Hormones PDFmohsen mirdamadiNo ratings yet
- Female Hormonal TherapyDocument38 pagesFemale Hormonal TherapySA NodeNo ratings yet
- Sex HormonesDocument12 pagesSex Hormoneshadeelizedeen08No ratings yet
- Sex HormonesDocument11 pagesSex Hormonesharishmore596No ratings yet
- 2019 Gonadal Hormones-3Document197 pages2019 Gonadal Hormones-3Vishwajeet RaneNo ratings yet
- 01 Lecture 9 Gonadal Hormones and Drugs (Pod Pharm DR Thatcher 2022)Document46 pages01 Lecture 9 Gonadal Hormones and Drugs (Pod Pharm DR Thatcher 2022)sahilaminNo ratings yet
- 7 Sex HormonesDocument28 pages7 Sex Hormonesمشتاقة للجنةNo ratings yet
- Drugs Affecting The FemaleDocument32 pagesDrugs Affecting The FemaleLule Allan PhillipNo ratings yet
- DR - Shameem R.AlaasamDocument31 pagesDR - Shameem R.Alaasamhacker ammerNo ratings yet
- Estrogens and AndrogensDocument7 pagesEstrogens and AndrogensAlbert Francis BialaNo ratings yet
- Estrogens and AndrogensDocument26 pagesEstrogens and AndrogensGwenny DumpNo ratings yet
- Topic Objectives: by The End of This Topic, The Learner Should Be Able ToDocument21 pagesTopic Objectives: by The End of This Topic, The Learner Should Be Able ToKeith OmwoyoNo ratings yet
- Gonadal Hormones, Their Inhibitors and Fertility and Antifertility AgentsDocument29 pagesGonadal Hormones, Their Inhibitors and Fertility and Antifertility AgentsGopal Prasad DahalNo ratings yet
- Estrogen and AndrogenDocument32 pagesEstrogen and AndrogenkwennybiangNo ratings yet
- Hormones and Related Drugs: Mechanism of ActionDocument21 pagesHormones and Related Drugs: Mechanism of ActionaviraaworldNo ratings yet
- AdrenalsDocument28 pagesAdrenalsMona NasrNo ratings yet
- Drugs Used For Women and Men'S Health: CC (Clomiphene Citrate)Document3 pagesDrugs Used For Women and Men'S Health: CC (Clomiphene Citrate)Clarissa MaglalangNo ratings yet
- New Estrogen and ProgesteroneDocument39 pagesNew Estrogen and ProgesteroneWegrimel AriegaraNo ratings yet
- Menopauz 1Document11 pagesMenopauz 1Nada CesarNo ratings yet
- Gonadal HormonesDocument40 pagesGonadal HormonesJoyce VillanuevaNo ratings yet
- Azathioprine DrugDocument18 pagesAzathioprine DrugteritohahaNo ratings yet
- علم السمومDocument4 pagesعلم السمومBouna BounaNo ratings yet
- Anterior Pituitary AgentsDocument4 pagesAnterior Pituitary AgentsGab SanchezNo ratings yet
- Male and Female HormonesDocument26 pagesMale and Female HormonesZuha HundalNo ratings yet
- Gonadal Hormones and InhibitorsDocument14 pagesGonadal Hormones and InhibitorsbluesumNo ratings yet
- Lecture 9: Drugs Effecting Function of UterusDocument22 pagesLecture 9: Drugs Effecting Function of UterusRtxGaming Zone 73No ratings yet
- 3 EndocrinologyDocument4 pages3 EndocrinologyJessa MayNo ratings yet
- March 22, 2007Document9 pagesMarch 22, 2007api-26938624No ratings yet
- Drugs 2 (Gyneac)Document103 pagesDrugs 2 (Gyneac)Aman Shaikh100% (2)
- 5 ProgestogensDocument33 pages5 Progestogensmhmtrgnn67No ratings yet
- 10-Gonadal HormonesDocument9 pages10-Gonadal Hormonesmedical.student.messiNo ratings yet
- HormonesDocument55 pagesHormonesAvinashNo ratings yet
- 1 - Endocrine 1 (Introduction) - MedicineDocument36 pages1 - Endocrine 1 (Introduction) - MedicineBHUWAN BASKOTANo ratings yet
- Drug Acting On Reproductive SystemDocument3 pagesDrug Acting On Reproductive SystemRoshann Marcus MamaysonNo ratings yet
- Hormonal ContraceptivesDocument25 pagesHormonal Contraceptivesmd easarur rahmanNo ratings yet
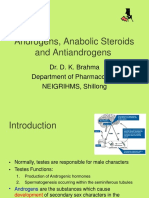
- Androgens, Anabolic Steroids and Antiandrogens: Dr. D. K. Brahma Department of Pharmacology NEIGRIHMS, ShillongDocument16 pagesAndrogens, Anabolic Steroids and Antiandrogens: Dr. D. K. Brahma Department of Pharmacology NEIGRIHMS, ShillongAbhijeet BhagatNo ratings yet
- EstrogensDocument15 pagesEstrogensАнна ВарданянNo ratings yet
- Female Sex HormonesDocument29 pagesFemale Sex Hormonesdhainey100% (5)
- Bp503t Pcol Unit-VDocument46 pagesBp503t Pcol Unit-VAakkkNo ratings yet
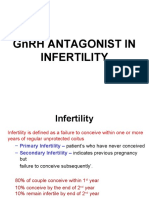
- GNRH Antagonist in InfertilityDocument70 pagesGNRH Antagonist in InfertilityBrijesh MishraNo ratings yet
- DR SR Agatha ShinyalaDocument60 pagesDR SR Agatha ShinyalaCLEMENTNo ratings yet
- Estrogens and Antiestrogens: Dr. D. K. Brahma Associate Professor of Pharmacology NEIGRIHMS, ShillongDocument24 pagesEstrogens and Antiestrogens: Dr. D. K. Brahma Associate Professor of Pharmacology NEIGRIHMS, ShillongdrfatimarizNo ratings yet
- Biosintesis Dan Mekanisme Kerja Hormon Repro Wanita PDFDocument39 pagesBiosintesis Dan Mekanisme Kerja Hormon Repro Wanita PDFsallynorcelinaNo ratings yet
- Pharmacology of Androgens and Other Anabolic SteroidsDocument19 pagesPharmacology of Androgens and Other Anabolic SteroidsAmanuel MaruNo ratings yet
- Hormone Replacement Therapy (HRT) :: DR - FatinDocument32 pagesHormone Replacement Therapy (HRT) :: DR - FatinAmmarNo ratings yet
- HRTDocument62 pagesHRTArpita ArpitaNo ratings yet
- Reproductive SystemDocument4 pagesReproductive SystemDenise Marienne MendezNo ratings yet
- Ap 2Document29 pagesAp 2Nikita NehaNo ratings yet
- Gonadal Hormones and InhibitorsDocument10 pagesGonadal Hormones and InhibitorsCarlos NiñoNo ratings yet
- Overview of Endocrine SystemDocument16 pagesOverview of Endocrine System2023ph17No ratings yet
- Endocrinology 1st TrimesterDocument16 pagesEndocrinology 1st TrimesteriwennieNo ratings yet
- AndrogenDocument19 pagesAndrogenTamam JauharNo ratings yet
- Hormone Balance How To Reclaim Hormone Balance, Sex Drive, Sleep & Lose Weight Now: The BasicsFrom EverandHormone Balance How To Reclaim Hormone Balance, Sex Drive, Sleep & Lose Weight Now: The BasicsRating: 3 out of 5 stars3/5 (2)
- Anticholinesterases and Anticholinergic Drugs: V Priya Nair MB Bs Frca Jennifer M Hunter MB CHB PHD FRCADocument5 pagesAnticholinesterases and Anticholinergic Drugs: V Priya Nair MB Bs Frca Jennifer M Hunter MB CHB PHD FRCAAbubakar JallohNo ratings yet
- Subcutaneous Mycosis: DR Sulaiman ContehDocument17 pagesSubcutaneous Mycosis: DR Sulaiman ContehAbubakar JallohNo ratings yet
- Class 5 - The Prophet As A Husband PDFDocument12 pagesClass 5 - The Prophet As A Husband PDFAbubakar JallohNo ratings yet
- Class 10 Polygyny PDFDocument17 pagesClass 10 Polygyny PDFAbubakar JallohNo ratings yet
- Interacting With Society As A Couple: ChildrenDocument9 pagesInteracting With Society As A Couple: ChildrenAbubakar JallohNo ratings yet
- Class 9 - PDFDocument11 pagesClass 9 - PDFAbubakar JallohNo ratings yet
- Fatty Liver in Protein Calorie Malnutrition : Depar:ments ofDocument4 pagesFatty Liver in Protein Calorie Malnutrition : Depar:ments ofAbubakar JallohNo ratings yet
- Class 6 - PDFDocument11 pagesClass 6 - PDFAbubakar JallohNo ratings yet
- Class 4 - RIGHTS OF THE HUSBAND AND WIFEDocument12 pagesClass 4 - RIGHTS OF THE HUSBAND AND WIFEAbubakar JallohNo ratings yet
- Thalassemia: by DR PP GevaoDocument46 pagesThalassemia: by DR PP GevaoAbubakar JallohNo ratings yet
- Iron Deficiency AnemiaDocument88 pagesIron Deficiency AnemiaAbubakar JallohNo ratings yet
- Cestodes Lecture: Dr. Sulaiman LakohDocument53 pagesCestodes Lecture: Dr. Sulaiman LakohAbubakar JallohNo ratings yet
- Chapter 5 Endocrinology 1Document53 pagesChapter 5 Endocrinology 1Abubakar JallohNo ratings yet
- Class 3 - Intimacy in Islam PDFDocument13 pagesClass 3 - Intimacy in Islam PDFAbubakar JallohNo ratings yet
- Introduction To NematodesDocument25 pagesIntroduction To NematodesAbubakar JallohNo ratings yet
- Chapter I Iodine Metabolism in ManDocument19 pagesChapter I Iodine Metabolism in ManAbubakar JallohNo ratings yet
- Class 2 - Who To Marry PDFDocument13 pagesClass 2 - Who To Marry PDFAbubakar JallohNo ratings yet
- Malaria: DR Sulaiman Conteh Medical StudentsDocument36 pagesMalaria: DR Sulaiman Conteh Medical StudentsAbubakar JallohNo ratings yet
- Eng PDFDocument232 pagesEng PDFAbubakar JallohNo ratings yet
- Class 3 - Intimacy in Islam PDFDocument13 pagesClass 3 - Intimacy in Islam PDFAbubakar JallohNo ratings yet
- What's Next?: Career & College Readiness Lesson PlanDocument12 pagesWhat's Next?: Career & College Readiness Lesson PlanAsh BakerNo ratings yet
- Action Plan in Science Jaja VersionDocument4 pagesAction Plan in Science Jaja VersionJaja Carlina100% (1)
- Arthropod Borne Infections - MHA (12 Files Merged)Document377 pagesArthropod Borne Infections - MHA (12 Files Merged)MariaNo ratings yet
- How To Write Your ReusmeDocument7 pagesHow To Write Your ReusmeBrian Israel Avila FloresNo ratings yet
- Sub Test Mole Concept PDFDocument7 pagesSub Test Mole Concept PDFVIKAS GARGNo ratings yet
- Koç İlaç KatalogDocument40 pagesKoç İlaç KatalogMedina JusmaniNo ratings yet
- Voice and Accent TrainingDocument26 pagesVoice and Accent TrainingDiana Andreea100% (1)
- Performance of BSIT Students in Their OJDocument13 pagesPerformance of BSIT Students in Their OJJohn Michael SernadillaNo ratings yet
- Meetings With Remarkable Men: Commentary by Terry Winter OwensDocument7 pagesMeetings With Remarkable Men: Commentary by Terry Winter OwensManjushree777No ratings yet
- Upre111E Qcourt: 3republir Toe F) Dilippine%Document13 pagesUpre111E Qcourt: 3republir Toe F) Dilippine%Ian San AndresNo ratings yet
- Reading Hormonal Changes During PregnancyDocument6 pagesReading Hormonal Changes During PregnancyKlinik Asy syifaNo ratings yet
- TafubobunopozomigomasoDocument2 pagesTafubobunopozomigomasoPriyanshusamratNo ratings yet
- Bosch Project 2020 PDFDocument1 pageBosch Project 2020 PDFAvi LimerNo ratings yet
- Property - Bar Ops 2009.combined - Atty - BatacanDocument36 pagesProperty - Bar Ops 2009.combined - Atty - BatacandavaounionNo ratings yet
- Consideration of Magnetizing Inrush Current Characteristics For Transformer Protection - 190510Document8 pagesConsideration of Magnetizing Inrush Current Characteristics For Transformer Protection - 190510p m yadavNo ratings yet
- Big Eng Level4 Test TSDocument4 pagesBig Eng Level4 Test TSNoelia LatronicoNo ratings yet
- Check-In Assistance Butler ServiceDocument3 pagesCheck-In Assistance Butler ServiceGoldy Grace Panganiban EstradaNo ratings yet
- Information Sheet: Ab Means A × B A ADocument5 pagesInformation Sheet: Ab Means A × B A ARaideru DielenNo ratings yet
- Rama Tirtha Quotes Collection 1Document4 pagesRama Tirtha Quotes Collection 1LeSublimeNo ratings yet
- FusionAE - Case Study 1Document9 pagesFusionAE - Case Study 1FredNo ratings yet
- Buying Behavior of Consumer For Sanitary ProductsDocument65 pagesBuying Behavior of Consumer For Sanitary ProductsfxvsfvNo ratings yet
- Response Letter 2Document3 pagesResponse Letter 2api-707692565No ratings yet
- SOALDocument7 pagesSOALMahar Catur FernizaNo ratings yet
- Andromeda ConstellationDocument3 pagesAndromeda ConstellationBoss CuencaNo ratings yet
- Minerals Engineering: Nenad DjordjevicDocument8 pagesMinerals Engineering: Nenad DjordjevicErvita MahendryNo ratings yet
- Top 14 Decisive Ancient Battles in HistoryDocument7 pagesTop 14 Decisive Ancient Battles in HistoryjamesNo ratings yet










































































































Download as pptx, pdf, or txt
You might also like
- Revised New PTLLS Assignment 1 Levels 3 and 4 Nov 2011Document3 pagesRevised New PTLLS Assignment 1 Levels 3 and 4 Nov 2011dave_perry189218No ratings yet
- Pharm Shelf Big Boss Review Aka Pharmacology Shelf Study GuideDocument13 pagesPharm Shelf Big Boss Review Aka Pharmacology Shelf Study Guideemceelee100% (2)
- Starbucks - Targetting, Positioning and Marketing MixDocument7 pagesStarbucks - Targetting, Positioning and Marketing MixSreerag Gangadharan89% (19)
- Properties of Standard AtmosphereDocument6 pagesProperties of Standard AtmosphereErnesto D. AguirreNo ratings yet
- Drugs Affecting Reproduction: DR - R - PrameelaDocument76 pagesDrugs Affecting Reproduction: DR - R - PrameelaRamadi PrameelaNo ratings yet
- Steroids JenniferKettelDocument25 pagesSteroids JenniferKettelvinay0717No ratings yet
- Sex HarmoneDocument22 pagesSex Harmonesuyash jainNo ratings yet
- New Estrogen and ProgesteroneDocument56 pagesNew Estrogen and ProgesteroneHBr100% (1)
- Drugs Used in Reproductive Health: Estrogen and ProgestinDocument41 pagesDrugs Used in Reproductive Health: Estrogen and ProgestindrfatimarizNo ratings yet
- Gonadal Hormones 62594Document98 pagesGonadal Hormones 62594TES SENNo ratings yet
- Oestrogen, Progesterone, AndrogensDocument58 pagesOestrogen, Progesterone, AndrogensTandin Sonam100% (1)
- Sex Hormones PDFDocument54 pagesSex Hormones PDFmohsen mirdamadiNo ratings yet
- Female Hormonal TherapyDocument38 pagesFemale Hormonal TherapySA NodeNo ratings yet
- Sex HormonesDocument12 pagesSex Hormoneshadeelizedeen08No ratings yet
- Sex HormonesDocument11 pagesSex Hormonesharishmore596No ratings yet
- 2019 Gonadal Hormones-3Document197 pages2019 Gonadal Hormones-3Vishwajeet RaneNo ratings yet
- 01 Lecture 9 Gonadal Hormones and Drugs (Pod Pharm DR Thatcher 2022)Document46 pages01 Lecture 9 Gonadal Hormones and Drugs (Pod Pharm DR Thatcher 2022)sahilaminNo ratings yet
- 7 Sex HormonesDocument28 pages7 Sex Hormonesمشتاقة للجنةNo ratings yet
- Drugs Affecting The FemaleDocument32 pagesDrugs Affecting The FemaleLule Allan PhillipNo ratings yet
- DR - Shameem R.AlaasamDocument31 pagesDR - Shameem R.Alaasamhacker ammerNo ratings yet
- Estrogens and AndrogensDocument7 pagesEstrogens and AndrogensAlbert Francis BialaNo ratings yet
- Estrogens and AndrogensDocument26 pagesEstrogens and AndrogensGwenny DumpNo ratings yet
- Topic Objectives: by The End of This Topic, The Learner Should Be Able ToDocument21 pagesTopic Objectives: by The End of This Topic, The Learner Should Be Able ToKeith OmwoyoNo ratings yet
- Gonadal Hormones, Their Inhibitors and Fertility and Antifertility AgentsDocument29 pagesGonadal Hormones, Their Inhibitors and Fertility and Antifertility AgentsGopal Prasad DahalNo ratings yet
- Estrogen and AndrogenDocument32 pagesEstrogen and AndrogenkwennybiangNo ratings yet
- Hormones and Related Drugs: Mechanism of ActionDocument21 pagesHormones and Related Drugs: Mechanism of ActionaviraaworldNo ratings yet
- AdrenalsDocument28 pagesAdrenalsMona NasrNo ratings yet
- Drugs Used For Women and Men'S Health: CC (Clomiphene Citrate)Document3 pagesDrugs Used For Women and Men'S Health: CC (Clomiphene Citrate)Clarissa MaglalangNo ratings yet
- New Estrogen and ProgesteroneDocument39 pagesNew Estrogen and ProgesteroneWegrimel AriegaraNo ratings yet
- Menopauz 1Document11 pagesMenopauz 1Nada CesarNo ratings yet
- Gonadal HormonesDocument40 pagesGonadal HormonesJoyce VillanuevaNo ratings yet
- Azathioprine DrugDocument18 pagesAzathioprine DrugteritohahaNo ratings yet
- علم السمومDocument4 pagesعلم السمومBouna BounaNo ratings yet
- Anterior Pituitary AgentsDocument4 pagesAnterior Pituitary AgentsGab SanchezNo ratings yet
- Male and Female HormonesDocument26 pagesMale and Female HormonesZuha HundalNo ratings yet
- Gonadal Hormones and InhibitorsDocument14 pagesGonadal Hormones and InhibitorsbluesumNo ratings yet
- Lecture 9: Drugs Effecting Function of UterusDocument22 pagesLecture 9: Drugs Effecting Function of UterusRtxGaming Zone 73No ratings yet
- 3 EndocrinologyDocument4 pages3 EndocrinologyJessa MayNo ratings yet
- March 22, 2007Document9 pagesMarch 22, 2007api-26938624No ratings yet
- Drugs 2 (Gyneac)Document103 pagesDrugs 2 (Gyneac)Aman Shaikh100% (2)
- 5 ProgestogensDocument33 pages5 Progestogensmhmtrgnn67No ratings yet
- 10-Gonadal HormonesDocument9 pages10-Gonadal Hormonesmedical.student.messiNo ratings yet
- HormonesDocument55 pagesHormonesAvinashNo ratings yet
- 1 - Endocrine 1 (Introduction) - MedicineDocument36 pages1 - Endocrine 1 (Introduction) - MedicineBHUWAN BASKOTANo ratings yet
- Drug Acting On Reproductive SystemDocument3 pagesDrug Acting On Reproductive SystemRoshann Marcus MamaysonNo ratings yet
- Hormonal ContraceptivesDocument25 pagesHormonal Contraceptivesmd easarur rahmanNo ratings yet
- Androgens, Anabolic Steroids and Antiandrogens: Dr. D. K. Brahma Department of Pharmacology NEIGRIHMS, ShillongDocument16 pagesAndrogens, Anabolic Steroids and Antiandrogens: Dr. D. K. Brahma Department of Pharmacology NEIGRIHMS, ShillongAbhijeet BhagatNo ratings yet
- EstrogensDocument15 pagesEstrogensАнна ВарданянNo ratings yet
- Female Sex HormonesDocument29 pagesFemale Sex Hormonesdhainey100% (5)
- Bp503t Pcol Unit-VDocument46 pagesBp503t Pcol Unit-VAakkkNo ratings yet
- GNRH Antagonist in InfertilityDocument70 pagesGNRH Antagonist in InfertilityBrijesh MishraNo ratings yet
- DR SR Agatha ShinyalaDocument60 pagesDR SR Agatha ShinyalaCLEMENTNo ratings yet
- Estrogens and Antiestrogens: Dr. D. K. Brahma Associate Professor of Pharmacology NEIGRIHMS, ShillongDocument24 pagesEstrogens and Antiestrogens: Dr. D. K. Brahma Associate Professor of Pharmacology NEIGRIHMS, ShillongdrfatimarizNo ratings yet
- Biosintesis Dan Mekanisme Kerja Hormon Repro Wanita PDFDocument39 pagesBiosintesis Dan Mekanisme Kerja Hormon Repro Wanita PDFsallynorcelinaNo ratings yet
- Pharmacology of Androgens and Other Anabolic SteroidsDocument19 pagesPharmacology of Androgens and Other Anabolic SteroidsAmanuel MaruNo ratings yet
- Hormone Replacement Therapy (HRT) :: DR - FatinDocument32 pagesHormone Replacement Therapy (HRT) :: DR - FatinAmmarNo ratings yet
- HRTDocument62 pagesHRTArpita ArpitaNo ratings yet
- Reproductive SystemDocument4 pagesReproductive SystemDenise Marienne MendezNo ratings yet
- Ap 2Document29 pagesAp 2Nikita NehaNo ratings yet
- Gonadal Hormones and InhibitorsDocument10 pagesGonadal Hormones and InhibitorsCarlos NiñoNo ratings yet
- Overview of Endocrine SystemDocument16 pagesOverview of Endocrine System2023ph17No ratings yet
- Endocrinology 1st TrimesterDocument16 pagesEndocrinology 1st TrimesteriwennieNo ratings yet
- AndrogenDocument19 pagesAndrogenTamam JauharNo ratings yet
- Hormone Balance How To Reclaim Hormone Balance, Sex Drive, Sleep & Lose Weight Now: The BasicsFrom EverandHormone Balance How To Reclaim Hormone Balance, Sex Drive, Sleep & Lose Weight Now: The BasicsRating: 3 out of 5 stars3/5 (2)
- Anticholinesterases and Anticholinergic Drugs: V Priya Nair MB Bs Frca Jennifer M Hunter MB CHB PHD FRCADocument5 pagesAnticholinesterases and Anticholinergic Drugs: V Priya Nair MB Bs Frca Jennifer M Hunter MB CHB PHD FRCAAbubakar JallohNo ratings yet
- Subcutaneous Mycosis: DR Sulaiman ContehDocument17 pagesSubcutaneous Mycosis: DR Sulaiman ContehAbubakar JallohNo ratings yet
- Class 5 - The Prophet As A Husband PDFDocument12 pagesClass 5 - The Prophet As A Husband PDFAbubakar JallohNo ratings yet
- Class 10 Polygyny PDFDocument17 pagesClass 10 Polygyny PDFAbubakar JallohNo ratings yet
- Interacting With Society As A Couple: ChildrenDocument9 pagesInteracting With Society As A Couple: ChildrenAbubakar JallohNo ratings yet
- Class 9 - PDFDocument11 pagesClass 9 - PDFAbubakar JallohNo ratings yet
- Fatty Liver in Protein Calorie Malnutrition : Depar:ments ofDocument4 pagesFatty Liver in Protein Calorie Malnutrition : Depar:ments ofAbubakar JallohNo ratings yet
- Class 6 - PDFDocument11 pagesClass 6 - PDFAbubakar JallohNo ratings yet
- Class 4 - RIGHTS OF THE HUSBAND AND WIFEDocument12 pagesClass 4 - RIGHTS OF THE HUSBAND AND WIFEAbubakar JallohNo ratings yet
- Thalassemia: by DR PP GevaoDocument46 pagesThalassemia: by DR PP GevaoAbubakar JallohNo ratings yet
- Iron Deficiency AnemiaDocument88 pagesIron Deficiency AnemiaAbubakar JallohNo ratings yet
- Cestodes Lecture: Dr. Sulaiman LakohDocument53 pagesCestodes Lecture: Dr. Sulaiman LakohAbubakar JallohNo ratings yet
- Chapter 5 Endocrinology 1Document53 pagesChapter 5 Endocrinology 1Abubakar JallohNo ratings yet
- Class 3 - Intimacy in Islam PDFDocument13 pagesClass 3 - Intimacy in Islam PDFAbubakar JallohNo ratings yet
- Introduction To NematodesDocument25 pagesIntroduction To NematodesAbubakar JallohNo ratings yet
- Chapter I Iodine Metabolism in ManDocument19 pagesChapter I Iodine Metabolism in ManAbubakar JallohNo ratings yet
- Class 2 - Who To Marry PDFDocument13 pagesClass 2 - Who To Marry PDFAbubakar JallohNo ratings yet
- Malaria: DR Sulaiman Conteh Medical StudentsDocument36 pagesMalaria: DR Sulaiman Conteh Medical StudentsAbubakar JallohNo ratings yet
- Eng PDFDocument232 pagesEng PDFAbubakar JallohNo ratings yet
- Class 3 - Intimacy in Islam PDFDocument13 pagesClass 3 - Intimacy in Islam PDFAbubakar JallohNo ratings yet
- What's Next?: Career & College Readiness Lesson PlanDocument12 pagesWhat's Next?: Career & College Readiness Lesson PlanAsh BakerNo ratings yet
- Action Plan in Science Jaja VersionDocument4 pagesAction Plan in Science Jaja VersionJaja Carlina100% (1)
- Arthropod Borne Infections - MHA (12 Files Merged)Document377 pagesArthropod Borne Infections - MHA (12 Files Merged)MariaNo ratings yet
- How To Write Your ReusmeDocument7 pagesHow To Write Your ReusmeBrian Israel Avila FloresNo ratings yet
- Sub Test Mole Concept PDFDocument7 pagesSub Test Mole Concept PDFVIKAS GARGNo ratings yet
- Koç İlaç KatalogDocument40 pagesKoç İlaç KatalogMedina JusmaniNo ratings yet
- Voice and Accent TrainingDocument26 pagesVoice and Accent TrainingDiana Andreea100% (1)
- Performance of BSIT Students in Their OJDocument13 pagesPerformance of BSIT Students in Their OJJohn Michael SernadillaNo ratings yet
- Meetings With Remarkable Men: Commentary by Terry Winter OwensDocument7 pagesMeetings With Remarkable Men: Commentary by Terry Winter OwensManjushree777No ratings yet
- Upre111E Qcourt: 3republir Toe F) Dilippine%Document13 pagesUpre111E Qcourt: 3republir Toe F) Dilippine%Ian San AndresNo ratings yet
- Reading Hormonal Changes During PregnancyDocument6 pagesReading Hormonal Changes During PregnancyKlinik Asy syifaNo ratings yet
- TafubobunopozomigomasoDocument2 pagesTafubobunopozomigomasoPriyanshusamratNo ratings yet
- Bosch Project 2020 PDFDocument1 pageBosch Project 2020 PDFAvi LimerNo ratings yet
- Property - Bar Ops 2009.combined - Atty - BatacanDocument36 pagesProperty - Bar Ops 2009.combined - Atty - BatacandavaounionNo ratings yet
- Consideration of Magnetizing Inrush Current Characteristics For Transformer Protection - 190510Document8 pagesConsideration of Magnetizing Inrush Current Characteristics For Transformer Protection - 190510p m yadavNo ratings yet
- Big Eng Level4 Test TSDocument4 pagesBig Eng Level4 Test TSNoelia LatronicoNo ratings yet
- Check-In Assistance Butler ServiceDocument3 pagesCheck-In Assistance Butler ServiceGoldy Grace Panganiban EstradaNo ratings yet
- Information Sheet: Ab Means A × B A ADocument5 pagesInformation Sheet: Ab Means A × B A ARaideru DielenNo ratings yet
- Rama Tirtha Quotes Collection 1Document4 pagesRama Tirtha Quotes Collection 1LeSublimeNo ratings yet
- FusionAE - Case Study 1Document9 pagesFusionAE - Case Study 1FredNo ratings yet
- Buying Behavior of Consumer For Sanitary ProductsDocument65 pagesBuying Behavior of Consumer For Sanitary ProductsfxvsfvNo ratings yet
- Response Letter 2Document3 pagesResponse Letter 2api-707692565No ratings yet
- SOALDocument7 pagesSOALMahar Catur FernizaNo ratings yet
- Andromeda ConstellationDocument3 pagesAndromeda ConstellationBoss CuencaNo ratings yet
- Minerals Engineering: Nenad DjordjevicDocument8 pagesMinerals Engineering: Nenad DjordjevicErvita MahendryNo ratings yet
- Top 14 Decisive Ancient Battles in HistoryDocument7 pagesTop 14 Decisive Ancient Battles in HistoryjamesNo ratings yet