Download as pptx, pdf, or txt
You might also like
- Care of ElderlyDocument130 pagesCare of Elderlyankita93% (14)
- Geriatric RehabilitationDocument57 pagesGeriatric Rehabilitationrejianil100% (5)
- OCCUPATIONAL DISEASES Clinical cases 2015 англ 2Document28 pagesOCCUPATIONAL DISEASES Clinical cases 2015 англ 2kjk100% (1)
- Hippo Emergency Medicine Board Review - Cram Section - MnemonicsDocument1 pageHippo Emergency Medicine Board Review - Cram Section - MnemonicslotskiNo ratings yet
- Atlas of Nuclear CardiologyDocument2 pagesAtlas of Nuclear CardiologyAmir FazelNo ratings yet
- Geriatric Rehabilitation: Prepared By: Floriza P. de Leon, PTRPDocument36 pagesGeriatric Rehabilitation: Prepared By: Floriza P. de Leon, PTRPFloriza de LeonNo ratings yet
- Care of Older Adult Finals IlgDocument77 pagesCare of Older Adult Finals IlgMiden AlbanoNo ratings yet
- Exercise Testin in GeriatricsDocument24 pagesExercise Testin in Geriatricsdr neha gaggarNo ratings yet
- Women HealthDocument6 pagesWomen HealthZayn KZtrikerNo ratings yet
- Healthy-Aging ImportantDocument98 pagesHealthy-Aging Importantmasterdoctor.clinicNo ratings yet
- Chronic IllnessDocument12 pagesChronic IllnessRegineCuasSulib100% (2)
- KP 1 Dasar-Dasar Kedokteran Gaya Hidup - Prof. Dr. Dr. Gusbakti SP - KKLPDocument19 pagesKP 1 Dasar-Dasar Kedokteran Gaya Hidup - Prof. Dr. Dr. Gusbakti SP - KKLPacalNo ratings yet
- Nursing and Rehabilitation of Residents of Old Age HomeDocument40 pagesNursing and Rehabilitation of Residents of Old Age HomeSnowdenNo ratings yet
- From Frail To Function To Fun: Section On Geriatrics American Physical Therapy AssociationDocument37 pagesFrom Frail To Function To Fun: Section On Geriatrics American Physical Therapy AssociationBal Mukund JhaNo ratings yet
- Activity and Exercise: Bornales, Michelle Chan, DarleneDocument14 pagesActivity and Exercise: Bornales, Michelle Chan, DarleneSophia Gayle RaagasNo ratings yet
- Geriatric NursingDocument46 pagesGeriatric NursingQuolette Constante100% (2)
- Exercise Prescription For Special PopulationDocument50 pagesExercise Prescription For Special PopulationMeera0% (1)
- DS Factors Influencing Motor Development Nov07Document28 pagesDS Factors Influencing Motor Development Nov07Arshad ShaikhNo ratings yet
- PPT-PEmodified 2Document53 pagesPPT-PEmodified 2ash hshsNo ratings yet
- Geriatrics IntroDocument15 pagesGeriatrics IntroAnanya KaurNo ratings yet
- GERIATRIC MEDICINE Lecture (Original)Document35 pagesGERIATRIC MEDICINE Lecture (Original)Dwi Wulandari100% (1)
- Student Week 6 - Physical HealthDocument47 pagesStudent Week 6 - Physical HealthikramNo ratings yet
- Age Related ChangesDocument34 pagesAge Related ChangesPoova RagavanNo ratings yet
- Eligrace Fabian, RN.: Clinical InstructorDocument35 pagesEligrace Fabian, RN.: Clinical Instructorsweetsai05No ratings yet
- CHN 2 ElderlyDocument25 pagesCHN 2 Elderlynimila gopiNo ratings yet
- Tiffanny Ocktivianie Tobing - Quiz of Physical Activity, Excercise and RehabilitationDocument3 pagesTiffanny Ocktivianie Tobing - Quiz of Physical Activity, Excercise and RehabilitationTiffanny Ocktivianie TobingNo ratings yet
- AGINGDocument113 pagesAGINGmalathi kotaNo ratings yet
- UNIT 3 Wellness IssuesDocument48 pagesUNIT 3 Wellness IssuesNicoleNo ratings yet
- Chapter 5 Geri ADocument15 pagesChapter 5 Geri ARhea Mae QuiñaNo ratings yet
- Old AgeDocument58 pagesOld AgeBEISAL BABY P100% (1)
- Geriatric Medicine Lecture UploadDocument35 pagesGeriatric Medicine Lecture UploadDoni MarthenNo ratings yet
- Geriatric Nursing Lecture 2020Document163 pagesGeriatric Nursing Lecture 2020Edgar RebuyasNo ratings yet
- Ageing PhysiologyDocument37 pagesAgeing Physiologyeyob kaseyeNo ratings yet
- Rontological NursingDocument8 pagesRontological Nursingec-bsNo ratings yet
- Needs of Elderly: Presentation byDocument51 pagesNeeds of Elderly: Presentation bymithiii123No ratings yet
- Geriatric Age Specific Author UCLA HealthDocument20 pagesGeriatric Age Specific Author UCLA HealthSHERIF ZAHERNo ratings yet
- Care of ElderlyDocument118 pagesCare of Elderlyabdullah almataryNo ratings yet
- PE 02 Chapter-1Document9 pagesPE 02 Chapter-1Milk BrotherNo ratings yet
- Exercise and Rehab OldDocument71 pagesExercise and Rehab OldAyyappan JayavelNo ratings yet
- Benefits On Physical ActivityDocument18 pagesBenefits On Physical ActivitySueBatNo ratings yet
- Old AgeDocument36 pagesOld AgeosamaNo ratings yet
- Toddle 77ae7850 Dd00 4d26 89fc 500fe365d87c Unit 5 Healthy Life StyleDocument14 pagesToddle 77ae7850 Dd00 4d26 89fc 500fe365d87c Unit 5 Healthy Life Style76t8n6vdg7No ratings yet
- Care For Critically Ill and The Elderly (Midterm)Document42 pagesCare For Critically Ill and The Elderly (Midterm)Hannah SchwartzNo ratings yet
- CCIE CombinedDocument100 pagesCCIE Combinedlevel3irregularsNo ratings yet
- Presented By: DR - Shilpa K PrajapatiDocument46 pagesPresented By: DR - Shilpa K PrajapatijothiNo ratings yet
- Multiple SclerosisDocument13 pagesMultiple SclerosisgopikaNo ratings yet
- Nursing Care For ElderlyDocument7 pagesNursing Care For ElderlyNeenu Rajput85% (13)
- PWU NCM 114 - Care of The Older Person 3Document34 pagesPWU NCM 114 - Care of The Older Person 3Ira AnuddinNo ratings yet
- Notes-Unit 3Document15 pagesNotes-Unit 3Aditya SharmaNo ratings yet
- Exercises and Use of Assistive DeicesDocument15 pagesExercises and Use of Assistive DeicesParul ThakurNo ratings yet
- Exercise PrescriptionDocument42 pagesExercise PrescriptionJoshua Diao100% (1)
- Fitness Training: Danish LatifDocument26 pagesFitness Training: Danish LatifShimmering MoonNo ratings yet
- Activity and Exercise: Shurouq Qadose 4/3/2008Document55 pagesActivity and Exercise: Shurouq Qadose 4/3/2008with_uNo ratings yet
- MidtermDocument4 pagesMidtermJennica BubanNo ratings yet
- 2.lecture-2, Physical Aspects of AgeingDocument49 pages2.lecture-2, Physical Aspects of AgeinglujainNo ratings yet
- Aging-Related Changes: Farhad Zargari, MD, PHDDocument47 pagesAging-Related Changes: Farhad Zargari, MD, PHDcj bariasNo ratings yet
- Physical and Psychological Changes in Older PersonDocument8 pagesPhysical and Psychological Changes in Older Personjanna mae patriarcaNo ratings yet
- Health Related Fitness PPT WEEK 3 4Document17 pagesHealth Related Fitness PPT WEEK 3 4Ash LeyNo ratings yet
- Musculoskeletal Wps OfficeDocument27 pagesMusculoskeletal Wps OfficeSteffanie TalaueNo ratings yet
- Lecture Notes - MobilityDocument9 pagesLecture Notes - MobilityAileen DonahueNo ratings yet
- FORMAT (Case Study PPS 3)Document2 pagesFORMAT (Case Study PPS 3)Angel FiloteoNo ratings yet
- Increased Serum Glucose Level (Hyperglycemia) 278.14 MG/DL (Normal: 70-100 MG/DL)Document3 pagesIncreased Serum Glucose Level (Hyperglycemia) 278.14 MG/DL (Normal: 70-100 MG/DL)Angel FiloteoNo ratings yet
- Key Issues Desired Outcome Independent Intervention Actual Outcome March 5, 2015Document4 pagesKey Issues Desired Outcome Independent Intervention Actual Outcome March 5, 2015Angel FiloteoNo ratings yet
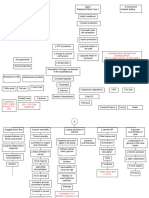
- Filoteo, Angel Hannah A. BSN 3B: Pathophysiologic Process - RHEUMATOID ARTHRITISDocument1 pageFiloteo, Angel Hannah A. BSN 3B: Pathophysiologic Process - RHEUMATOID ARTHRITISAngel FiloteoNo ratings yet
- PRJ prj0000253Document30 pagesPRJ prj0000253Angel FiloteoNo ratings yet
- Name: Filoteo, Angel Hannah A. Date: Sept. 7,2020Document3 pagesName: Filoteo, Angel Hannah A. Date: Sept. 7,2020Angel FiloteoNo ratings yet
- Pathophysiology - Rheumatoid ArthritisDocument1 pagePathophysiology - Rheumatoid ArthritisAngel FiloteoNo ratings yet
- Neuro Coa 2 - Otter - AiDocument4 pagesNeuro Coa 2 - Otter - AiAngel FiloteoNo ratings yet
- Safety and Safe MedicationDocument92 pagesSafety and Safe MedicationAngel FiloteoNo ratings yet
- Neurological Function: Mark Ebony SumalinogDocument51 pagesNeurological Function: Mark Ebony SumalinogAngel FiloteoNo ratings yet
- ReadingDocument45 pagesReadingAngel FiloteoNo ratings yet
- ListeningDocument64 pagesListeningAngel FiloteoNo ratings yet
- Rest and Sleep: Week 4 Mr. Mark Ebony C. Sumalinog, RN MSNDocument80 pagesRest and Sleep: Week 4 Mr. Mark Ebony C. Sumalinog, RN MSNAngel Filoteo100% (1)
- Preschool & School-AgeDocument4 pagesPreschool & School-AgeAngel FiloteoNo ratings yet
- 4 Cardiovascular HealthDocument79 pages4 Cardiovascular HealthAngel FiloteoNo ratings yet
- Chapter 28: Virology: Poxvirus Herpes Virus Adenovirus Papovavirus Hepatitis BDocument2 pagesChapter 28: Virology: Poxvirus Herpes Virus Adenovirus Papovavirus Hepatitis BAngel FiloteoNo ratings yet
- Integumentary: Mark Ebony C. SumalinogDocument89 pagesIntegumentary: Mark Ebony C. SumalinogAngel FiloteoNo ratings yet
- Motor 1Document3 pagesMotor 1Angel FiloteoNo ratings yet
- HACVD PathoDocument1 pageHACVD PathoAngel FiloteoNo ratings yet
- Death Can Occur From The Misuse of Cough and Cold Medicines in Very Young ChildrenDocument4 pagesDeath Can Occur From The Misuse of Cough and Cold Medicines in Very Young ChildrenAngel FiloteoNo ratings yet
- Key Issues Desired Outcomes Interventions Actual OutcomesDocument4 pagesKey Issues Desired Outcomes Interventions Actual OutcomesAngel FiloteoNo ratings yet
- Velez College College of Nursing F. Ramos St. Cebu CityDocument3 pagesVelez College College of Nursing F. Ramos St. Cebu CityAngel FiloteoNo ratings yet
- Sodium Imbalances (Hyponatremia Vs Hypernatremia)Document17 pagesSodium Imbalances (Hyponatremia Vs Hypernatremia)Angel FiloteoNo ratings yet
- Guidelines For The Management of COVID-19 in Health FacilitiesDocument35 pagesGuidelines For The Management of COVID-19 in Health FacilitiesherathhmasNo ratings yet
- Jurding DR SaugiDocument44 pagesJurding DR SaugiDian FitriNo ratings yet
- Important Questions For Esic Staff Nurse Recruitment ExamDocument4 pagesImportant Questions For Esic Staff Nurse Recruitment ExamSuchitaNo ratings yet
- Steroid Hyperglycemia: Prevalence, Early Detection and Therapeutic Recommendations: A Narrative ReviewDocument10 pagesSteroid Hyperglycemia: Prevalence, Early Detection and Therapeutic Recommendations: A Narrative ReviewMade Dedy KusnawanNo ratings yet
- Immune Reconstitution Inflammatory SyndromeDocument8 pagesImmune Reconstitution Inflammatory SyndromeRafif Abdurrahman WijisaksonoNo ratings yet
- Continuous Positive Airway Pressure (CPAP)Document9 pagesContinuous Positive Airway Pressure (CPAP)yassen hassanNo ratings yet
- LEARNING DIARY FOR NCM 105n/L-Nutrition and Diet Therapy Date: Name: Topics: Guide QuestionsDocument3 pagesLEARNING DIARY FOR NCM 105n/L-Nutrition and Diet Therapy Date: Name: Topics: Guide QuestionsWendell Gian GolezNo ratings yet
- 643 1943 1 PBDocument10 pages643 1943 1 PBririsNo ratings yet
- Hyperuricemia XXXX XXXXX XxjeuneDocument32 pagesHyperuricemia XXXX XXXXX XxjeuneOziq Juga ReMa-eNo ratings yet
- Bioinstrument 7 (Respiratory System) 16-22Document7 pagesBioinstrument 7 (Respiratory System) 16-22vividmeNo ratings yet
- Hydration: Water's Role in The BodyDocument2 pagesHydration: Water's Role in The BodykarvizNo ratings yet
- Student Overview: # Question and Answer Choices Points CategoriesDocument17 pagesStudent Overview: # Question and Answer Choices Points CategoriesGabriel AndradeNo ratings yet
- EMNoteDocument1 pageEMNoteKC Dela RosaNo ratings yet
- 2nd Quarter ScienceDocument3 pages2nd Quarter Sciencesusan h. bucasasNo ratings yet
- Biotin Benefits PDFDocument8 pagesBiotin Benefits PDFRocco LamponeNo ratings yet
- Claves DX en DermapatologíaDocument420 pagesClaves DX en DermapatologíaFreddy RojasNo ratings yet
- NURSING PROCEDURES RT GI SYSTEMDocument226 pagesNURSING PROCEDURES RT GI SYSTEMMika SaldanaNo ratings yet
- Reasonable Accommodation Forms2Document4 pagesReasonable Accommodation Forms2DBHAAdminNo ratings yet
- Marasmus Down SyndromeDocument40 pagesMarasmus Down SyndromeKURBULDKNo ratings yet
- HypnotherapyDocument5 pagesHypnotherapyapi-585441161No ratings yet
- 6 Isometric ExerciseDocument10 pages6 Isometric ExerciseJohn MelichNo ratings yet
- Epidemiology and Pathogenesis of Neisseria Gonorrhoeae Infection - UpToDateDocument22 pagesEpidemiology and Pathogenesis of Neisseria Gonorrhoeae Infection - UpToDateCarina ColtuneacNo ratings yet
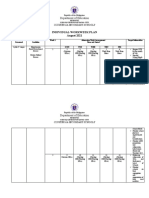
- Department of Education: Individual Workweek Plan August 2021Document5 pagesDepartment of Education: Individual Workweek Plan August 2021Jeffren P. MiguelNo ratings yet
- East Africa University Bosaso, Puntland Somalia Faculty of Medicine Communicable Disease MR Buruj Ali SaladDocument42 pagesEast Africa University Bosaso, Puntland Somalia Faculty of Medicine Communicable Disease MR Buruj Ali SaladShaimaa AbdulkadirNo ratings yet
- Graphic Organizer ExampleDocument1 pageGraphic Organizer Exampleapi-398530613No ratings yet
- Descriptive Research Regarding The COVID-19Document5 pagesDescriptive Research Regarding The COVID-19Mish Lei FranxhNo ratings yet
- AMETROPIADocument48 pagesAMETROPIARahul KirkNo ratings yet