Download as ppt, pdf, or txt
You might also like
- Ebook PDF The Phlebotomy Textbook 4th Edition PDFDocument41 pagesEbook PDF The Phlebotomy Textbook 4th Edition PDFmelody.bowers405100% (37)
- COSHH Assessment TemplateDocument2 pagesCOSHH Assessment TemplaterichardNo ratings yet
- Users Guides To The Medical Literature III How ToDocument13 pagesUsers Guides To The Medical Literature III How ToFidzaNo ratings yet
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3No ratings yet
- The Mental Health of Jehovah WitnessesDocument5 pagesThe Mental Health of Jehovah WitnessesKreshnik HAJDARI100% (1)
- The Red EyeDocument71 pagesThe Red Eyehenok biruk80% (5)
- CONJUNCTIVITISDocument67 pagesCONJUNCTIVITISNauli Panjaitan86% (7)
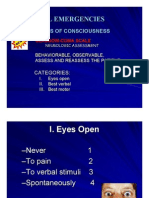
- Medical EmergenciesDocument81 pagesMedical EmergenciesKreshnik HAJDARINo ratings yet
- Red Eye Differential DiagnosisDocument70 pagesRed Eye Differential DiagnosisAdetz HaedetzNo ratings yet
- Konjungtivitis Dan KeratitisDocument117 pagesKonjungtivitis Dan KeratitisResti Puteri ApriyuslimNo ratings yet
- Eye Infection /inflammation: Presented byDocument49 pagesEye Infection /inflammation: Presented byPriya bhattiNo ratings yet
- Pemicu 2 "Ada Apa Dengan Mataku?": Adrian Pratama - 405100018 - Blok PenginderaanDocument82 pagesPemicu 2 "Ada Apa Dengan Mataku?": Adrian Pratama - 405100018 - Blok PenginderaanRilianda SimbolonNo ratings yet
- Eye Emergency: DR Abdelmoniem SaeedDocument63 pagesEye Emergency: DR Abdelmoniem SaeedYousef Al-AmeenNo ratings yet
- Mata Merah, Visus Normal - 1Document51 pagesMata Merah, Visus Normal - 1nashqonashNo ratings yet
- Conjunctivitis and Other Ocular Lesions Opthalmology ClassDocument43 pagesConjunctivitis and Other Ocular Lesions Opthalmology ClassJaikrit SinghNo ratings yet
- NAME:-Puspendu Maity. ROLL: - 16101717014. Reg. No: - 171611210014. Subject: - Corneal Ulcer. Semester: - 7 SemesterDocument15 pagesNAME:-Puspendu Maity. ROLL: - 16101717014. Reg. No: - 171611210014. Subject: - Corneal Ulcer. Semester: - 7 SemesterKumar jit MaityNo ratings yet
- ABC of Red EyeDocument5 pagesABC of Red Eyeakmar887No ratings yet
- Conjunctival Disorders OghreDocument59 pagesConjunctival Disorders Oghreteamtruth50No ratings yet
- Blefaritis EarlyDocument28 pagesBlefaritis EarlyPaomo Zhixia EarlyNo ratings yet
- Special Senses 2014 - 1Document91 pagesSpecial Senses 2014 - 1Winz DolleteNo ratings yet
- ConjunctivaDocument85 pagesConjunctivaMuhammad AboAlasaadNo ratings yet
- Bacterial ConjunctivitisDocument5 pagesBacterial ConjunctivitisBnB UsmleNo ratings yet
- Types of ConjunctivitisDocument20 pagesTypes of ConjunctivitisAnonymous 9lmlWQoDm8No ratings yet
- Red Eye Clinical Presentation: History and Physical ExaminationDocument11 pagesRed Eye Clinical Presentation: History and Physical ExaminationLaiba KhanNo ratings yet
- Keratitis KonjungtivitisDocument81 pagesKeratitis KonjungtivitisAngnes Dera MustikaNo ratings yet
- 4 Conjunctival Disorders OghreDocument104 pages4 Conjunctival Disorders OghreUyigue EuniceNo ratings yet
- The Red EyeDocument37 pagesThe Red EyeJan Marnie ReniedoNo ratings yet
- D.D of Red EyeDocument116 pagesD.D of Red Eyehassan daacadNo ratings yet
- SENSESDocument18 pagesSENSESJimlord GarciaNo ratings yet
- KeratitisDocument16 pagesKeratitisHarmin AliminNo ratings yet
- Common Eye Problems and DiagnosisDocument84 pagesCommon Eye Problems and Diagnosisvivekrajbhilai5850No ratings yet
- Conjunctivitis Hordeolum ChalazionDocument52 pagesConjunctivitis Hordeolum ChalazionPatricia May CruzNo ratings yet
- Conjunctiva Anatomy and PhysiologyDocument101 pagesConjunctiva Anatomy and PhysiologyPurva KeswaniNo ratings yet
- Microbialkeratitisbhatti 160607231414Document56 pagesMicrobialkeratitisbhatti 160607231414RanveerNo ratings yet
- James B &bron A. Lecture Notes: Ophthalmology. Ed 11. John Wiley & Sons. 2011Document9 pagesJames B &bron A. Lecture Notes: Ophthalmology. Ed 11. John Wiley & Sons. 2011qisthiNo ratings yet
- BlepharitisDocument15 pagesBlepharitisLatoya ShopNo ratings yet
- Disorders of The Eye LidsDocument33 pagesDisorders of The Eye Lidsc/risaaq yuusuf ColoowNo ratings yet
- Corneal Bacterial UlcerDocument48 pagesCorneal Bacterial UlcerAkansha Rastogi100% (1)
- Anatomi Dan Fisiologi KorneaDocument133 pagesAnatomi Dan Fisiologi KorneaAriyanie NurtaniaNo ratings yet
- Intervention For Clients With Eye and Vision Problems: Eyelid Disorders Blepharitis ChalazionDocument11 pagesIntervention For Clients With Eye and Vision Problems: Eyelid Disorders Blepharitis ChalazionDarius CrisostomoNo ratings yet
- Clinical App Red Eye Without Blurred VisionDocument38 pagesClinical App Red Eye Without Blurred VisionPriskila SamanthaNo ratings yet
- Conjunctivitis by Asma GulDocument36 pagesConjunctivitis by Asma GulAbdul SamadNo ratings yet
- PODocument47 pagesPOFidhiyahRNo ratings yet
- Eye Viva Pool SolvedDocument109 pagesEye Viva Pool SolvedhermionewolfgangNo ratings yet
- 09conjunctival Infections 13-12-07Document55 pages09conjunctival Infections 13-12-07ari rujatiNo ratings yet
- Adult BlepharitisDocument11 pagesAdult BlepharitistrisnatersinandaNo ratings yet
- Mata MerahDocument119 pagesMata MerahAzwanHamdiNo ratings yet
- Ophthalmology For 5th Year Exams: Visual AcuityDocument7 pagesOphthalmology For 5th Year Exams: Visual AcuitySaloni PatelNo ratings yet
- Eyelid Disorders: Ii. ChalazionDocument62 pagesEyelid Disorders: Ii. ChalazionFreeburn SimunchembuNo ratings yet
- Lit Review - Contact Lens Associated Pseudomonas KeratitisDocument8 pagesLit Review - Contact Lens Associated Pseudomonas KeratitisAlien4mearthNo ratings yet
- What Is Corneal Ulcer?Document23 pagesWhat Is Corneal Ulcer?Sol JoeNo ratings yet
- Infeksi Kelainan Kongenital Dan TumorDocument54 pagesInfeksi Kelainan Kongenital Dan Tumorniska darliantiNo ratings yet
- OphthoDocument27 pagesOphthoYavani KulasinghamNo ratings yet
- Neonatal ConjunctivitisDocument20 pagesNeonatal ConjunctivitisRumaiha SadiaNo ratings yet
- 3 Eyelid Disorders OghreDocument127 pages3 Eyelid Disorders OghreUyigue EuniceNo ratings yet
- Eyelid Disorders - Diagnosis and Management - AAFPDocument15 pagesEyelid Disorders - Diagnosis and Management - AAFPMufassiraturrahmahNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document48 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Nauli PanjaitanNo ratings yet
- Blepharitis - Medical Disability GuidelinesDocument3 pagesBlepharitis - Medical Disability GuidelinesFerni ArmantiNo ratings yet
- Conjunctivitis: by PGMI Jasleen MonrealDocument77 pagesConjunctivitis: by PGMI Jasleen MonrealJade MonrealNo ratings yet
- ConjunctivaDocument40 pagesConjunctivaSarahNo ratings yet
- OpthaDocument5 pagesOpthavarun2k6No ratings yet
- CLPC & ClpuDocument31 pagesCLPC & ClpuSunny jaiswalNo ratings yet
- Phatology The Eyelids, Lacrimal GlandsDocument62 pagesPhatology The Eyelids, Lacrimal GlandsGermanyNo ratings yet
- BIBLE BEFORE SCIENCE RevisedDocument32 pagesBIBLE BEFORE SCIENCE RevisedKreshnik HAJDARINo ratings yet
- How To Win Over WorryDocument9 pagesHow To Win Over WorryKreshnik HAJDARINo ratings yet
- UrinalysisDocument5 pagesUrinalysisKreshnik HAJDARINo ratings yet
- Liver TestsDocument17 pagesLiver TestsKreshnik HAJDARI100% (1)
- Child's HerniaDocument13 pagesChild's HerniaKreshnik HAJDARINo ratings yet
- Inspirimi I Bibles BIBLE INSPIRATIONDocument4 pagesInspirimi I Bibles BIBLE INSPIRATIONKreshnik HAJDARINo ratings yet
- Dobesimi I Shikimit VISION LOSSDocument7 pagesDobesimi I Shikimit VISION LOSSKreshnik HAJDARINo ratings yet
- A Hoax and Its ParadoxesDocument11 pagesA Hoax and Its ParadoxesKreshnik HAJDARINo ratings yet
- Evaluating The Febrile Patient With A RashDocument23 pagesEvaluating The Febrile Patient With A RashKreshnik HAJDARI100% (1)
- Benign or Harbinger of Sudden Death?: R. Oehm, MD, FACC, 10/26/06 With POTTS 10/20/08Document48 pagesBenign or Harbinger of Sudden Death?: R. Oehm, MD, FACC, 10/26/06 With POTTS 10/20/08Kreshnik HAJDARINo ratings yet
- Electrocardiogramm - Ecg InterpretationDocument56 pagesElectrocardiogramm - Ecg InterpretationKreshnik HAJDARI100% (1)
- Gastroenterology Function Bowel DisordersDocument12 pagesGastroenterology Function Bowel DisordersKreshnik HAJDARINo ratings yet
- Pruritus Ani, Hemorroidet EtjDocument4 pagesPruritus Ani, Hemorroidet EtjKreshnik HAJDARINo ratings yet
- Leukocytosis: Basics of Clinical Assessment: Production, Maturation and Survival of LeukocytesDocument9 pagesLeukocytosis: Basics of Clinical Assessment: Production, Maturation and Survival of LeukocytesKreshnik HAJDARINo ratings yet
- EliminationDocument20 pagesEliminationHasan A AsFour100% (2)
- 2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical UpdateDocument43 pages2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical UpdateLê Thị HươngNo ratings yet
- Community Survey ToolDocument10 pagesCommunity Survey ToolDranreb Berylle MasangkayNo ratings yet
- Dr. Ayushi Verma, BDS: Professtional SummaryDocument2 pagesDr. Ayushi Verma, BDS: Professtional SummaryAyushi VermaNo ratings yet
- Group 2 Saffola CaseDocument5 pagesGroup 2 Saffola CaseAmit KapoorNo ratings yet
- The Diagnosis of Fibromyalgia Syndrome Guidelines - 1 - 0Document57 pagesThe Diagnosis of Fibromyalgia Syndrome Guidelines - 1 - 0Firstiafina TiffanyNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale Evaluation IndependentDocument3 pagesAssessment Nursing Diagnosis Planning Intervention Rationale Evaluation IndependentSHEILA MAE SACLOTNo ratings yet
- CHN Notes National Part 1Document39 pagesCHN Notes National Part 1Justine Ingrid O. FernandezNo ratings yet
- Stress ManagementDocument36 pagesStress ManagementShanky Jain100% (2)
- Migrant Health in The PhilippinesDocument6 pagesMigrant Health in The PhilippinesRenzo R. GuintoNo ratings yet
- Work-Related StressDocument16 pagesWork-Related StressCristina RicanNo ratings yet
- Make Today Count - The Secret of - Maxwell, John CDocument124 pagesMake Today Count - The Secret of - Maxwell, John CBoukary TiendNo ratings yet
- Dr. Daniel H. Bessesen: The Biology of ObesityDocument58 pagesDr. Daniel H. Bessesen: The Biology of ObesityNational Press FoundationNo ratings yet
- Chapter 27 ViolenceDocument28 pagesChapter 27 ViolenceSraddha PatelNo ratings yet
- March 2013 Board of Nursing NoticesDocument528 pagesMarch 2013 Board of Nursing NoticesJames LindonNo ratings yet
- Product List 23062023Document34 pagesProduct List 23062023SUGAM MEDICALNo ratings yet
- Aisbisf-Cir-04 Dated 19.04.2022-Uniform Transfer Policy For Award Staff (2022)Document7 pagesAisbisf-Cir-04 Dated 19.04.2022-Uniform Transfer Policy For Award Staff (2022)Mahesh GhsNo ratings yet
- Health Benefits of Dark ChocolateDocument16 pagesHealth Benefits of Dark Chocolatesahla amri100% (1)
- Proton Pump Inhibitors - AMBOSSDocument3 pagesProton Pump Inhibitors - AMBOSSRuva Oscass JimmyNo ratings yet
- UNDP TR HSHandbook - 2009 PDFDocument79 pagesUNDP TR HSHandbook - 2009 PDFLumbiwe MakunkaNo ratings yet
- Report of Vision 2020 IAPB Workshop IndonesiaDocument12 pagesReport of Vision 2020 IAPB Workshop IndonesiaAstidya Miranti100% (1)
- Novitasari R G2A009063 Bab8KTIDocument30 pagesNovitasari R G2A009063 Bab8KTIMas sobah SobahNo ratings yet
- Emergency Procedures and Primary Care in Physical Therapy: A Practice ManualDocument32 pagesEmergency Procedures and Primary Care in Physical Therapy: A Practice ManualBushra MehwishNo ratings yet
- High Blood Pressure Brochure WPRDocument4 pagesHigh Blood Pressure Brochure WPRChomang SutrisnaNo ratings yet
- Soil Transmitted HelminthiasisDocument34 pagesSoil Transmitted HelminthiasisDada BalateroNo ratings yet
- The Hospital For Sick Children Handbook of Pediatrics 12E May 12 2022 - 0323713408 - Elsevier 12Th Edition The Hospital For Sic Full ChapterDocument68 pagesThe Hospital For Sick Children Handbook of Pediatrics 12E May 12 2022 - 0323713408 - Elsevier 12Th Edition The Hospital For Sic Full Chapterlloyd.leos558100% (19)
- CEO Healthcare Nonprofit Organization in Rapid City SD Resume Keith BaileyDocument2 pagesCEO Healthcare Nonprofit Organization in Rapid City SD Resume Keith BaileyKeithBaileyNo ratings yet