Download as pptx, pdf, or txt
You might also like
- Esther ParksDocument6 pagesEsther ParksMyrnaivette Pierson63% (19)
- Part 1 SAQs Specimen QuestionsDocument79 pagesPart 1 SAQs Specimen Questionsخولة رشيد العيسى100% (2)
- Second TrimesterDocument11 pagesSecond Trimestermardsz100% (2)
- Vomiting in ChildrenDocument44 pagesVomiting in ChildrenAstri Faluna SheylavontiaNo ratings yet
- Nursing Care of DiarrheaDocument30 pagesNursing Care of DiarrheayustiNo ratings yet
- Necrotizing Enterocolitis (NEC) : Intensive Care Nursery House Staff ManualDocument3 pagesNecrotizing Enterocolitis (NEC) : Intensive Care Nursery House Staff ManualJovvitaNo ratings yet
- Acute and Chronic DiarrhoeaDocument20 pagesAcute and Chronic DiarrhoeaVipul Nagnesia100% (2)
- Case HirschsprungDocument29 pagesCase HirschsprungPriscila StevanniNo ratings yet
- Presentation Acute Epigastric PainDocument31 pagesPresentation Acute Epigastric Painnajeeb.arbani027No ratings yet
- History PerformaDocument5 pagesHistory PerformaHariharan NarendranNo ratings yet
- Gastro NephroDocument93 pagesGastro Nephrohasanatiya41No ratings yet
- GIT DisordersDocument171 pagesGIT DisordersKatrina PonceNo ratings yet
- Nursing Patho CardsDocument195 pagesNursing Patho Cardsgiogmail100% (1)
- Gi NclexDocument14 pagesGi NclexYoke W Khoo100% (3)
- 4 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns FinalDocument35 pages4 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns Finalevren yilmazNo ratings yet
- Definition and Etiology: PancreatitisDocument24 pagesDefinition and Etiology: PancreatitisAliyah Tofani PawelloiNo ratings yet
- Nursing MGT of PT With Lower Git DisordersDocument65 pagesNursing MGT of PT With Lower Git DisordersCarlos LorenzoNo ratings yet
- VomitingDocument59 pagesVomitingزياد سعيدNo ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Cholecystitis Viva TopicDocument4 pagesCholecystitis Viva TopicSalma NazarNo ratings yet
- Plenary 2B Group 13Document132 pagesPlenary 2B Group 13Obet Agung 天No ratings yet
- Young Lady With Severe Generalized Abdominal Pain (2Document33 pagesYoung Lady With Severe Generalized Abdominal Pain (2najeeb.arbani027No ratings yet
- Acute Abdomen SummaryDocument3 pagesAcute Abdomen SummaryAbdul Ghaffar AbdullahNo ratings yet
- NCM 116 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns PDFDocument35 pagesNCM 116 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns PDFKathlyn Joy DulayNo ratings yet
- PEPTIC ULCER DISEASE 2018 EdittedDocument43 pagesPEPTIC ULCER DISEASE 2018 EdittedJumbe MohamedNo ratings yet
- Gastroenteritis in ChildrenDocument48 pagesGastroenteritis in ChildrenKelsingra FitzChivalry FarseerNo ratings yet
- 2300 - Module 8 - Gastrointestinal and Genitourinary EmergenciesDocument14 pages2300 - Module 8 - Gastrointestinal and Genitourinary Emergenciesmegan.abbinkNo ratings yet
- Pathophysiology of GooDocument2 pagesPathophysiology of GooTania Noviza100% (1)
- 4 Examining Gastrointestinal SystemDocument75 pages4 Examining Gastrointestinal SystemSafi MohammedNo ratings yet
- Gastroenterology UPDATEDDocument21 pagesGastroenterology UPDATEDmuradkhanNo ratings yet
- Assessment and Management of Patients With Lower GI Tract DisordersDocument43 pagesAssessment and Management of Patients With Lower GI Tract DisordersAilyn LoroNo ratings yet
- Week 7 - Pediatric GI DisturbancesDocument59 pagesWeek 7 - Pediatric GI DisturbancesLeyla GalyanoNo ratings yet
- Hirschprung DiseaseDocument10 pagesHirschprung DiseaseRichard S. RoxasNo ratings yet
- Case Presentation: Group 3-BDocument39 pagesCase Presentation: Group 3-BKenneth NuñezNo ratings yet
- Urinary Tract DisordersDocument54 pagesUrinary Tract Disorderssharon ocharaNo ratings yet
- ConstipationDocument38 pagesConstipationAZNo ratings yet
- Nausea VomitingDocument36 pagesNausea VomitingDian Fitri100% (1)
- Week 8 Pedia Pediatric GI DisturbancesDocument110 pagesWeek 8 Pedia Pediatric GI DisturbancesJaja ManezNo ratings yet
- DiarrheaDocument23 pagesDiarrheayadavmanas808No ratings yet
- PreeclampsiaDocument179 pagesPreeclampsiaJohn Wilbert Birung100% (3)
- PP T 16 Absorption Elimination Sir RudyDocument50 pagesPP T 16 Absorption Elimination Sir RudyJelaisa PallasigueNo ratings yet
- Concept For Abdominal BloatingDocument1 pageConcept For Abdominal BloatingChiomaDabrinze-AmosNwankwoNo ratings yet
- Nursing Care of Patient With Digestive IndexDocument28 pagesNursing Care of Patient With Digestive IndexAngela FerrerNo ratings yet
- Common Laboratory ProceduresDocument4 pagesCommon Laboratory ProceduresrahafNo ratings yet
- Gi SMB - Clin MedDocument5 pagesGi SMB - Clin MedSohil PatelNo ratings yet
- PancreatitisDocument18 pagesPancreatitisMihir PatelNo ratings yet
- Responsesm To Metabolic Gi and Liver AlterationsDocument62 pagesResponsesm To Metabolic Gi and Liver AlterationsEdelen GaleNo ratings yet
- SOAP AbdominalDocument12 pagesSOAP Abdominalnakblan4No ratings yet
- Abdominal Pain - Royal Children HospitalDocument4 pagesAbdominal Pain - Royal Children HospitalMehrdad IraniNo ratings yet
- Acute DiarrheaDocument28 pagesAcute DiarrheaAyubNo ratings yet
- Hypertrophic Pyloric StenosisDocument3 pagesHypertrophic Pyloric StenosisCandice ChengNo ratings yet
- Gastric Outlet ObstructionDocument42 pagesGastric Outlet ObstructionSouvikNo ratings yet
- Hyperemesis Gravidarum: Dr. Irene Maria Elena, SP - OG Departemen Obstetri Dan Ginekologi FK UkridaDocument38 pagesHyperemesis Gravidarum: Dr. Irene Maria Elena, SP - OG Departemen Obstetri Dan Ginekologi FK UkridaAndhyka TumimomorNo ratings yet
- Gastro 1 ReviewDocument50 pagesGastro 1 ReviewJohnny BNo ratings yet
- Abdominal Pain - IBS ChecklistDocument3 pagesAbdominal Pain - IBS Checklistsalwakh266No ratings yet
- Abdominal TB Causing Intestinal ObstructionDocument10 pagesAbdominal TB Causing Intestinal ObstructionCleoanne GallegosNo ratings yet
- Abdominal PainDocument6 pagesAbdominal PainMatthieu FortinNo ratings yet
- INTUSSUSCEPTIONDocument3 pagesINTUSSUSCEPTIONS GNo ratings yet
- Group 4 Case Presentation DiarrheaDocument46 pagesGroup 4 Case Presentation DiarrheaEphraim John QuichoNo ratings yet
- Approach To Vomiting: DR Vivek JhaDocument23 pagesApproach To Vomiting: DR Vivek JhaMukesh ThakurNo ratings yet
- 2 Common Congenital Anomalies of The GI TractDocument27 pages2 Common Congenital Anomalies of The GI TractZyke NovenoNo ratings yet
- Antituberculous DrugDocument29 pagesAntituberculous DrugMalueth AnguiNo ratings yet
- Other Anti-HivDocument24 pagesOther Anti-HivMalueth AnguiNo ratings yet
- Med II Antihelminthics and Antiprotozoal Agents 2008Document31 pagesMed II Antihelminthics and Antiprotozoal Agents 2008Malueth AnguiNo ratings yet
- Antiviral TherapyDocument19 pagesAntiviral TherapyMalueth AnguiNo ratings yet
- Nnrtis: Nonnucleoside Reverse Trancriptase InhibitorsDocument12 pagesNnrtis: Nonnucleoside Reverse Trancriptase InhibitorsMalueth AnguiNo ratings yet
- Protease Inhibitors (Pi) : Anyika CelpherDocument22 pagesProtease Inhibitors (Pi) : Anyika CelpherMalueth AnguiNo ratings yet
- Antiviral DrugsDocument13 pagesAntiviral DrugsMalueth AnguiNo ratings yet
- Antiretroviral Therapy: Dr. Samuel Mwaniki (Bpharm., MSC Tid, Uon)Document22 pagesAntiretroviral Therapy: Dr. Samuel Mwaniki (Bpharm., MSC Tid, Uon)Malueth AnguiNo ratings yet
- Antiretroviral Therapy: Pharmacology: Cristina Gruta, PharmdDocument47 pagesAntiretroviral Therapy: Pharmacology: Cristina Gruta, PharmdMalueth AnguiNo ratings yet
- Antimalarial DrugsDocument49 pagesAntimalarial DrugsMalueth Angui50% (2)
- Human Immunodeficiency VirusDocument24 pagesHuman Immunodeficiency VirusMalueth AnguiNo ratings yet
- Hiv HaartDocument12 pagesHiv HaartMalueth AnguiNo ratings yet
- Antifungal DrugsDocument66 pagesAntifungal DrugsMalueth AnguiNo ratings yet
- Adrenal DisordersDocument36 pagesAdrenal DisordersMalueth AnguiNo ratings yet
- Head & Neck TumoursDocument15 pagesHead & Neck TumoursMalueth AnguiNo ratings yet
- Hypoparathyroidism: DR GwerDocument14 pagesHypoparathyroidism: DR GwerMalueth AnguiNo ratings yet
- Cytogenetics PresentationDocument11 pagesCytogenetics PresentationMalueth AnguiNo ratings yet
- Ambiguous Genitalia (Disorders of Sexual Differentiation) : DR GwerDocument18 pagesAmbiguous Genitalia (Disorders of Sexual Differentiation) : DR GwerMalueth AnguiNo ratings yet
- Chemotherapy: Chemotherapy, in Its Most General Sense, Refers To Treatment of Disease byDocument42 pagesChemotherapy: Chemotherapy, in Its Most General Sense, Refers To Treatment of Disease byMalueth AnguiNo ratings yet
- K 17 Colorectal CarcinomaDocument63 pagesK 17 Colorectal CarcinomaMalueth AnguiNo ratings yet
- Targeted Therapy: Specific Targeted Molecules Needed For Carcinogenesis and Tumor GrowthDocument9 pagesTargeted Therapy: Specific Targeted Molecules Needed For Carcinogenesis and Tumor GrowthMalueth AnguiNo ratings yet
- Prostate CancerDocument67 pagesProstate CancerMalueth AnguiNo ratings yet
- Hepatocellular CarcinomaDocument10 pagesHepatocellular CarcinomaMalueth AnguiNo ratings yet
- 2 LOCAL ANAESTHETICS EgertonDocument24 pages2 LOCAL ANAESTHETICS EgertonMalueth AnguiNo ratings yet
- 2 INTRAVENOUS ANESTHESIA EgertonDocument21 pages2 INTRAVENOUS ANESTHESIA EgertonMalueth AnguiNo ratings yet
- Constitutional Growth DelayDocument23 pagesConstitutional Growth DelayMalueth AnguiNo ratings yet
- ABDOMINAL AND PELVIC MASSES IN PEDIATRICS - Level 4Document26 pagesABDOMINAL AND PELVIC MASSES IN PEDIATRICS - Level 4Malueth AnguiNo ratings yet
- Immunization:: DR Wamalwa DDocument45 pagesImmunization:: DR Wamalwa DMalueth Angui0% (1)
- Child Abuse & Neglect: MBCHB Iv 2006Document24 pagesChild Abuse & Neglect: MBCHB Iv 2006Malueth AnguiNo ratings yet
- Child Abuse and NeglectDocument25 pagesChild Abuse and NeglectMalueth Angui100% (1)
- 2121-Article Text-9456-1-10-20230131Document8 pages2121-Article Text-9456-1-10-20230131Çağdaş BaytarNo ratings yet
- Edgar CayceDocument15 pagesEdgar CayceAlenka VenišnikNo ratings yet
- Due Date Calculator: Are You Counting Weeks, Months and Trimesters? Use Our Due Date Birthday!Document6 pagesDue Date Calculator: Are You Counting Weeks, Months and Trimesters? Use Our Due Date Birthday!Sanjay Kumar SanjuNo ratings yet
- 2015 Critical Care Ultrasound PDFDocument527 pages2015 Critical Care Ultrasound PDFAlan Espíndola Cruz100% (1)
- Penn John Doe CVDocument6 pagesPenn John Doe CVerphansNo ratings yet
- Nursing Care PlanDocument9 pagesNursing Care PlanRenea Joy ArruejoNo ratings yet
- Rome III Diagnostic Questionnaire For The Pediatric Functional GI DisordersDocument30 pagesRome III Diagnostic Questionnaire For The Pediatric Functional GI DisordersAmelia YendraNo ratings yet
- Nursing DiagnosisDocument3 pagesNursing DiagnosislesternNo ratings yet
- Post Traumatic Stress DisorderDocument7 pagesPost Traumatic Stress Disordersomebody_maNo ratings yet
- Pilates: in Prevention ("Pilates Studio") and Physiotherapy ("Pilates For Rehabilitation")Document1 pagePilates: in Prevention ("Pilates Studio") and Physiotherapy ("Pilates For Rehabilitation")Rubén LópezNo ratings yet
- AANMC - The 6 PrinciplesDocument1 pageAANMC - The 6 Principlesregencap6358No ratings yet
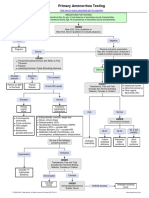
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- 2020 Eating DisordersDocument13 pages2020 Eating DisordersNathália CristimannNo ratings yet
- DrugDocument4 pagesDrugApril Daye B. AsuncionNo ratings yet
- ReportingDocument4 pagesReportingErika MarieNo ratings yet
- Prothrombin Time and International Normalized Ratio (PT - INR) - Lab Tests OnlineDocument11 pagesProthrombin Time and International Normalized Ratio (PT - INR) - Lab Tests OnlineAlyaNo ratings yet
- Hafnia AlveiDocument5 pagesHafnia AlveiluisNo ratings yet
- Prescribing in ChildrenDocument4 pagesPrescribing in ChildrenArkopal GuptaNo ratings yet
- Ophthalmology Clinical Cases pixOpOpDocument61 pagesOphthalmology Clinical Cases pixOpOpUsman ImtiazNo ratings yet
- Case The Levacor Heart PumpDocument2 pagesCase The Levacor Heart PumpJohn Aaron De GuiaNo ratings yet
- 22 - Atypical Squamous Cells in Liquid-Based CervicalDocument6 pages22 - Atypical Squamous Cells in Liquid-Based CervicalRenan RodriguesNo ratings yet
- Job InterviewDocument4 pagesJob InterviewERICATHENANo ratings yet
- NCM 112 TH (12F)Document24 pagesNCM 112 TH (12F)Justine April YbanezNo ratings yet
- NLIC Reimbursement Claim Form PDFDocument1 pageNLIC Reimbursement Claim Form PDFJowel MercadoNo ratings yet
- Natural History of Chronic Subdural Haematoma: K.-S.LEEDocument8 pagesNatural History of Chronic Subdural Haematoma: K.-S.LEEAngelSosaNo ratings yet
- Sindrom Uko Ene Osobe (Moersch-Woltman) : Lije Vjesn 2010 132:110-114Document5 pagesSindrom Uko Ene Osobe (Moersch-Woltman) : Lije Vjesn 2010 132:110-114bimtolaNo ratings yet
- Hyderabad: Cortico-Basal Implantology CourseDocument6 pagesHyderabad: Cortico-Basal Implantology CourseYousuf AdamNo ratings yet