
Physiology DES: Biruk A. (Balemaye@sgu - Edu) & Sami Ahmed. (Sahmed10@sgu - Edu)
Physiology DES: Biruk A. (Balemaye@sgu - Edu) & Sami Ahmed. (Sahmed10@sgu - Edu)
You might also like
- Examine Com Stack Guide Libido and Sexual EnhancementDocument16 pagesExamine Com Stack Guide Libido and Sexual Enhancementrichard100% (1)
- Abdomen (Inguinal Hernia) : Anatomy II Block 3 NotesDocument39 pagesAbdomen (Inguinal Hernia) : Anatomy II Block 3 NotesJoseph KimNo ratings yet
- DiGeorge Case Fall 2016 PDFDocument2 pagesDiGeorge Case Fall 2016 PDFJoseph KimNo ratings yet
- DiGeorge Case Fall 2016 PDFDocument2 pagesDiGeorge Case Fall 2016 PDFJoseph KimNo ratings yet
- HeartDocument50 pagesHeartmmm479cb4kNo ratings yet
- Physiology of HeartDocument74 pagesPhysiology of Heartmadeha goharNo ratings yet
- CardiovascularDocument40 pagesCardiovascularÁñèsh Kåøs100% (1)
- CVS Physiology FinalDocument21 pagesCVS Physiology FinalVondNo ratings yet
- Physiology of Heart in DetailDocument101 pagesPhysiology of Heart in Detailakanksha sharmaNo ratings yet
- Cardiovascular System Study SheetDocument8 pagesCardiovascular System Study SheetTkNo ratings yet
- Cardiovasular SystemDocument26 pagesCardiovasular SystemPhai KoemhienNo ratings yet
- 11 - CardiophysiologyDocument68 pages11 - CardiophysiologyRohit K YNo ratings yet
- Cardiovascular System: (Review)Document42 pagesCardiovascular System: (Review)Leichel AlbertoNo ratings yet
- Lecture - 3 Properties of Cardiac MuscleDocument35 pagesLecture - 3 Properties of Cardiac MuscleMRM7MDNo ratings yet
- CVS PhysiologyDocument43 pagesCVS Physiologyapi-3705050100% (1)
- Cardiology Ebook Notes PDFDocument26 pagesCardiology Ebook Notes PDFsugisweNo ratings yet
- 02 AntiarrhythmicAgentsDocument83 pages02 AntiarrhythmicAgentsSiddhant BanwatNo ratings yet
- Or Cardiac Physiology, Pathophysiology, and Some PharmacologyDocument58 pagesOr Cardiac Physiology, Pathophysiology, and Some PharmacologyJacob StoneNo ratings yet
- Hemodynamics: Ncmb418 - Critical Care Nursing Rle Midterm LectureDocument7 pagesHemodynamics: Ncmb418 - Critical Care Nursing Rle Midterm LectureKyle Saberon100% (1)
- Physio CardioDocument36 pagesPhysio Cardiopooh7No ratings yet
- What Is ArrhythmiaDocument14 pagesWhat Is ArrhythmiaSharan MurugaboopathyNo ratings yet
- Heart Muscle: The Heart As A Pump and FunctionDocument4 pagesHeart Muscle: The Heart As A Pump and Functionmcwnotes100% (1)
- Cardiovascular SystemDocument50 pagesCardiovascular Systemkintan kamila100% (1)
- Cardiovascular Physiology & Urine Formation: Biology 25 A. SantiagoDocument39 pagesCardiovascular Physiology & Urine Formation: Biology 25 A. Santiagoapi-3826751No ratings yet
- Electrical Conduction in The HeartDocument35 pagesElectrical Conduction in The HeartNormasnizam Mohd NoorNo ratings yet
- Functional Human Physiology: For The Exercise and Sport Sciences The Cardiovascular System: Cardiac FunctionDocument186 pagesFunctional Human Physiology: For The Exercise and Sport Sciences The Cardiovascular System: Cardiac FunctionBery Agana F. PurbaNo ratings yet
- Fast Ap PhysioDocument3 pagesFast Ap PhysioAndrea de GuzmanNo ratings yet
- 11 Ant HEART MUSCLEDocument57 pages11 Ant HEART MUSCLEZuhaib AhmedNo ratings yet
- Introduction To Cardiovascular PhysiologyDocument29 pagesIntroduction To Cardiovascular PhysiologyMariuca MaryNo ratings yet
- The Cardiovascular SystemDocument4 pagesThe Cardiovascular SystemSharie Mae MataumNo ratings yet
- BLG111 Week2 Blood Heart 2Document74 pagesBLG111 Week2 Blood Heart 2phuongphuonganhanh171203No ratings yet
- C9Document15 pagesC9SLKNo ratings yet
- Conducting System of The HeartDocument68 pagesConducting System of The HeartNilay PatelNo ratings yet
- Physiology - Rhythmical Excitation of Heart by Dr. Mudassar Ali RoomiDocument18 pagesPhysiology - Rhythmical Excitation of Heart by Dr. Mudassar Ali RoomiMudassar Roomi100% (2)
- Conducting System of The HeartDocument27 pagesConducting System of The HeartMuhammadNo ratings yet
- Physiology of CardiovascularDocument74 pagesPhysiology of CardiovascularStevan SalosaNo ratings yet
- Cardiac PhysioDocument9 pagesCardiac Physiosakuragi jakeNo ratings yet
- Cardiovascular IntroductionDocument27 pagesCardiovascular Introductiontehillahkabwe100No ratings yet
- Cardiac Cycle Electrical Mechanical EventsDocument49 pagesCardiac Cycle Electrical Mechanical EventsJardee Datsima100% (1)
- Physio Mod 16-17Document7 pagesPhysio Mod 16-17mjdangca0111No ratings yet
- Prof DR Najneen AkhterDocument62 pagesProf DR Najneen Akhterislamamirul0487No ratings yet
- Cardiovascular PhysiologyDocument7 pagesCardiovascular PhysiologyHabib UllahNo ratings yet
- Lecture 2: The Heart: Prof. Magidah Alaudi, M.SCDocument62 pagesLecture 2: The Heart: Prof. Magidah Alaudi, M.SCMonicaNo ratings yet
- Cardiac PacemakersDocument49 pagesCardiac PacemakersMohammad AliNo ratings yet
- MCB136 SP 22 MT2 Study GuideDocument4 pagesMCB136 SP 22 MT2 Study GuideJeffrey JèwNo ratings yet
- Cardiology Summary PDFDocument62 pagesCardiology Summary PDFSyamsuriWahyuNo ratings yet
- Cardiovascular SystemDocument35 pagesCardiovascular Systemdelacruzchristinejoie.kldNo ratings yet
- 03 Cardiopulmonary PhysiologyDocument17 pages03 Cardiopulmonary Physiologyice cream1000791100% (1)
- CVS 1 Cardiac CycleDocument29 pagesCVS 1 Cardiac CycleDedani MakakaNo ratings yet
- Electrical Activity of Heart CellsDocument37 pagesElectrical Activity of Heart Cellsspdharanimaran001No ratings yet
- Cardio-Physiology Exam QuestionsDocument17 pagesCardio-Physiology Exam Questionsjimmy100% (2)
- Pharmacotherapy of ArrythmiasDocument68 pagesPharmacotherapy of ArrythmiasABREHAM BUKULONo ratings yet
- Cardiac PhysiologDocument30 pagesCardiac PhysiologKannan GNo ratings yet
- MD-7 HearttDocument28 pagesMD-7 HearttvincenzoNo ratings yet
- Cardiac Arrhythmia: Prepared By: Charina Gail O. Baloy, RPH, Msc. (C.)Document44 pagesCardiac Arrhythmia: Prepared By: Charina Gail O. Baloy, RPH, Msc. (C.)Chinenye Akwue100% (1)
- Cardiac AssessmentDocument54 pagesCardiac AssessmentAthira PSNo ratings yet
- Cvs Physiology 1Document18 pagesCvs Physiology 1Thayalan AllanNo ratings yet
- First Session-Dr - Maryam MalekiDocument49 pagesFirst Session-Dr - Maryam MalekiAamir EjazNo ratings yet
- Downloadfile 28Document31 pagesDownloadfile 28Chowdhury Mohammed Tawhid TasneefNo ratings yet
- Cardiovascular Physiology Lecture 1Document95 pagesCardiovascular Physiology Lecture 1Freelance LeagueNo ratings yet
- Circulation WorksheetDocument3 pagesCirculation Worksheetholagato100% (1)
- CH 18 Cholesterol Metabolism: Biochem Block 3 NotesDocument38 pagesCH 18 Cholesterol Metabolism: Biochem Block 3 NotesJoseph KimNo ratings yet
- Respiratory System: Lab Interactive SessionDocument20 pagesRespiratory System: Lab Interactive SessionJoseph KimNo ratings yet
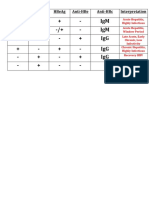
- HBV Antibody InterpretationDocument1 pageHBV Antibody InterpretationJoseph KimNo ratings yet
- Physio-DES-6 (Cardiac)Document56 pagesPhysio-DES-6 (Cardiac)Joseph Kim100% (1)
- Clinical Integration: Lymphatic & Respiratory SystemsDocument13 pagesClinical Integration: Lymphatic & Respiratory SystemsJoseph KimNo ratings yet
- Physio Lab CasesDocument4 pagesPhysio Lab CasesJoseph KimNo ratings yet
- Lymphatic System: Lab Interactive SessionDocument24 pagesLymphatic System: Lab Interactive SessionJoseph KimNo ratings yet
- Virus ClassificationDocument1 pageVirus ClassificationJoseph KimNo ratings yet
- Bernard Barber's Social System Theory: The American Sociologist June 2002Document20 pagesBernard Barber's Social System Theory: The American Sociologist June 2002Rainman1618No ratings yet
- DRUG NAME: Octreotide: Synonym (S) : Common Trade Name (S) : ClassificationDocument9 pagesDRUG NAME: Octreotide: Synonym (S) : Common Trade Name (S) : ClassificationChandanaSanjeeNo ratings yet
- Grade 6 - e A Tire Tracks Lesson 4Document3 pagesGrade 6 - e A Tire Tracks Lesson 4api-283081427No ratings yet
- Surveying For Highways: Eng. Suneth Thushara Highwy Design Division RDADocument31 pagesSurveying For Highways: Eng. Suneth Thushara Highwy Design Division RDAzeshan habibNo ratings yet
- NotingDocument160 pagesNotingdpkonnetNo ratings yet
- Verbal Communic-WPS OfficeDocument4 pagesVerbal Communic-WPS Officechandy RendajeNo ratings yet
- Sport Management Review: Evald Bundgaard Iversen, Graham CuskellyDocument13 pagesSport Management Review: Evald Bundgaard Iversen, Graham CuskellyGabriela Ioana IonitaNo ratings yet
- Cookie Business PlanDocument27 pagesCookie Business PlanLiza Mhey AcedoNo ratings yet
- Reading in Philippines HistoryDocument7 pagesReading in Philippines Historyrafaelalmazar416No ratings yet
- Nagunni 1Document2 pagesNagunni 1mayank.sharmaNo ratings yet
- FINAL TERM P.E.H. 12 Demonstrate Proper Etiquette and Safety in The Use of Facilities and Equipment For Dance ActivitiesDocument3 pagesFINAL TERM P.E.H. 12 Demonstrate Proper Etiquette and Safety in The Use of Facilities and Equipment For Dance Activitiesrandolf wassigNo ratings yet
- Give The Lord Glory and Honor (Psalm 96)Document1 pageGive The Lord Glory and Honor (Psalm 96)Lionel Valdellon100% (1)
- Dhan Allyn Romero 11 Saturn ABM EAPPDocument7 pagesDhan Allyn Romero 11 Saturn ABM EAPPJhevie RanileNo ratings yet
- Megillah 3Document70 pagesMegillah 3Julian Ungar-SargonNo ratings yet
- Vijaya Bank ChanchalDocument2 pagesVijaya Bank ChanchalShubham sharmaNo ratings yet
- 2005 Nicolet National Bank Annual ReportDocument16 pages2005 Nicolet National Bank Annual ReportNicolet BankNo ratings yet
- Pokemon Fusion GeneratorDocument1 pagePokemon Fusion GeneratorFrost MourneNo ratings yet
- Anb Brochure Fietsroute Klaprozen Heuvelland enDocument4 pagesAnb Brochure Fietsroute Klaprozen Heuvelland enBella BossNo ratings yet
- Entertainment Weekly - February 19, 2016Document120 pagesEntertainment Weekly - February 19, 2016Prateek Herpersad100% (1)
- HRM BBA MBA Lec 789 Job Analysis and DesignDocument41 pagesHRM BBA MBA Lec 789 Job Analysis and Designrhmafia786No ratings yet
- DxdiagDocument35 pagesDxdiagCr DickyNo ratings yet
- Links 8400peliculasDocument385 pagesLinks 8400peliculasjulio floresNo ratings yet
- Mvno - Encik KunciDocument15 pagesMvno - Encik KunciJolliffe NicholasNo ratings yet
- IBM UML 2.0 Advanced NotationsDocument21 pagesIBM UML 2.0 Advanced NotationsKeerthana SubramanianNo ratings yet
- Book Review " THE GREAT GATSBY "Document5 pagesBook Review " THE GREAT GATSBY "sayemNo ratings yet
- Futuro (Will-Going To - P.C.)Document1 pageFuturo (Will-Going To - P.C.)carolina herreraNo ratings yet
- Accy 211 - Week 8 Tut HWDocument2 pagesAccy 211 - Week 8 Tut HWIsaac ElhageNo ratings yet
- De Los Santos II v. BarbosaDocument8 pagesDe Los Santos II v. BarbosaApril IsidroNo ratings yet
- Nervous System Worksheet1Document3 pagesNervous System Worksheet1fe jandugan0% (1)

































































































Download as pptx, pdf, or txt
You might also like
- Examine Com Stack Guide Libido and Sexual EnhancementDocument16 pagesExamine Com Stack Guide Libido and Sexual Enhancementrichard100% (1)
- Abdomen (Inguinal Hernia) : Anatomy II Block 3 NotesDocument39 pagesAbdomen (Inguinal Hernia) : Anatomy II Block 3 NotesJoseph KimNo ratings yet
- DiGeorge Case Fall 2016 PDFDocument2 pagesDiGeorge Case Fall 2016 PDFJoseph KimNo ratings yet
- DiGeorge Case Fall 2016 PDFDocument2 pagesDiGeorge Case Fall 2016 PDFJoseph KimNo ratings yet
- HeartDocument50 pagesHeartmmm479cb4kNo ratings yet
- Physiology of HeartDocument74 pagesPhysiology of Heartmadeha goharNo ratings yet
- CardiovascularDocument40 pagesCardiovascularÁñèsh Kåøs100% (1)
- CVS Physiology FinalDocument21 pagesCVS Physiology FinalVondNo ratings yet
- Physiology of Heart in DetailDocument101 pagesPhysiology of Heart in Detailakanksha sharmaNo ratings yet
- Cardiovascular System Study SheetDocument8 pagesCardiovascular System Study SheetTkNo ratings yet
- Cardiovasular SystemDocument26 pagesCardiovasular SystemPhai KoemhienNo ratings yet
- 11 - CardiophysiologyDocument68 pages11 - CardiophysiologyRohit K YNo ratings yet
- Cardiovascular System: (Review)Document42 pagesCardiovascular System: (Review)Leichel AlbertoNo ratings yet
- Lecture - 3 Properties of Cardiac MuscleDocument35 pagesLecture - 3 Properties of Cardiac MuscleMRM7MDNo ratings yet
- CVS PhysiologyDocument43 pagesCVS Physiologyapi-3705050100% (1)
- Cardiology Ebook Notes PDFDocument26 pagesCardiology Ebook Notes PDFsugisweNo ratings yet
- 02 AntiarrhythmicAgentsDocument83 pages02 AntiarrhythmicAgentsSiddhant BanwatNo ratings yet
- Or Cardiac Physiology, Pathophysiology, and Some PharmacologyDocument58 pagesOr Cardiac Physiology, Pathophysiology, and Some PharmacologyJacob StoneNo ratings yet
- Hemodynamics: Ncmb418 - Critical Care Nursing Rle Midterm LectureDocument7 pagesHemodynamics: Ncmb418 - Critical Care Nursing Rle Midterm LectureKyle Saberon100% (1)
- Physio CardioDocument36 pagesPhysio Cardiopooh7No ratings yet
- What Is ArrhythmiaDocument14 pagesWhat Is ArrhythmiaSharan MurugaboopathyNo ratings yet
- Heart Muscle: The Heart As A Pump and FunctionDocument4 pagesHeart Muscle: The Heart As A Pump and Functionmcwnotes100% (1)
- Cardiovascular SystemDocument50 pagesCardiovascular Systemkintan kamila100% (1)
- Cardiovascular Physiology & Urine Formation: Biology 25 A. SantiagoDocument39 pagesCardiovascular Physiology & Urine Formation: Biology 25 A. Santiagoapi-3826751No ratings yet
- Electrical Conduction in The HeartDocument35 pagesElectrical Conduction in The HeartNormasnizam Mohd NoorNo ratings yet
- Functional Human Physiology: For The Exercise and Sport Sciences The Cardiovascular System: Cardiac FunctionDocument186 pagesFunctional Human Physiology: For The Exercise and Sport Sciences The Cardiovascular System: Cardiac FunctionBery Agana F. PurbaNo ratings yet
- Fast Ap PhysioDocument3 pagesFast Ap PhysioAndrea de GuzmanNo ratings yet
- 11 Ant HEART MUSCLEDocument57 pages11 Ant HEART MUSCLEZuhaib AhmedNo ratings yet
- Introduction To Cardiovascular PhysiologyDocument29 pagesIntroduction To Cardiovascular PhysiologyMariuca MaryNo ratings yet
- The Cardiovascular SystemDocument4 pagesThe Cardiovascular SystemSharie Mae MataumNo ratings yet
- BLG111 Week2 Blood Heart 2Document74 pagesBLG111 Week2 Blood Heart 2phuongphuonganhanh171203No ratings yet
- C9Document15 pagesC9SLKNo ratings yet
- Conducting System of The HeartDocument68 pagesConducting System of The HeartNilay PatelNo ratings yet
- Physiology - Rhythmical Excitation of Heart by Dr. Mudassar Ali RoomiDocument18 pagesPhysiology - Rhythmical Excitation of Heart by Dr. Mudassar Ali RoomiMudassar Roomi100% (2)
- Conducting System of The HeartDocument27 pagesConducting System of The HeartMuhammadNo ratings yet
- Physiology of CardiovascularDocument74 pagesPhysiology of CardiovascularStevan SalosaNo ratings yet
- Cardiac PhysioDocument9 pagesCardiac Physiosakuragi jakeNo ratings yet
- Cardiovascular IntroductionDocument27 pagesCardiovascular Introductiontehillahkabwe100No ratings yet
- Cardiac Cycle Electrical Mechanical EventsDocument49 pagesCardiac Cycle Electrical Mechanical EventsJardee Datsima100% (1)
- Physio Mod 16-17Document7 pagesPhysio Mod 16-17mjdangca0111No ratings yet
- Prof DR Najneen AkhterDocument62 pagesProf DR Najneen Akhterislamamirul0487No ratings yet
- Cardiovascular PhysiologyDocument7 pagesCardiovascular PhysiologyHabib UllahNo ratings yet
- Lecture 2: The Heart: Prof. Magidah Alaudi, M.SCDocument62 pagesLecture 2: The Heart: Prof. Magidah Alaudi, M.SCMonicaNo ratings yet
- Cardiac PacemakersDocument49 pagesCardiac PacemakersMohammad AliNo ratings yet
- MCB136 SP 22 MT2 Study GuideDocument4 pagesMCB136 SP 22 MT2 Study GuideJeffrey JèwNo ratings yet
- Cardiology Summary PDFDocument62 pagesCardiology Summary PDFSyamsuriWahyuNo ratings yet
- Cardiovascular SystemDocument35 pagesCardiovascular Systemdelacruzchristinejoie.kldNo ratings yet
- 03 Cardiopulmonary PhysiologyDocument17 pages03 Cardiopulmonary Physiologyice cream1000791100% (1)
- CVS 1 Cardiac CycleDocument29 pagesCVS 1 Cardiac CycleDedani MakakaNo ratings yet
- Electrical Activity of Heart CellsDocument37 pagesElectrical Activity of Heart Cellsspdharanimaran001No ratings yet
- Cardio-Physiology Exam QuestionsDocument17 pagesCardio-Physiology Exam Questionsjimmy100% (2)
- Pharmacotherapy of ArrythmiasDocument68 pagesPharmacotherapy of ArrythmiasABREHAM BUKULONo ratings yet
- Cardiac PhysiologDocument30 pagesCardiac PhysiologKannan GNo ratings yet
- MD-7 HearttDocument28 pagesMD-7 HearttvincenzoNo ratings yet
- Cardiac Arrhythmia: Prepared By: Charina Gail O. Baloy, RPH, Msc. (C.)Document44 pagesCardiac Arrhythmia: Prepared By: Charina Gail O. Baloy, RPH, Msc. (C.)Chinenye Akwue100% (1)
- Cardiac AssessmentDocument54 pagesCardiac AssessmentAthira PSNo ratings yet
- Cvs Physiology 1Document18 pagesCvs Physiology 1Thayalan AllanNo ratings yet
- First Session-Dr - Maryam MalekiDocument49 pagesFirst Session-Dr - Maryam MalekiAamir EjazNo ratings yet
- Downloadfile 28Document31 pagesDownloadfile 28Chowdhury Mohammed Tawhid TasneefNo ratings yet
- Cardiovascular Physiology Lecture 1Document95 pagesCardiovascular Physiology Lecture 1Freelance LeagueNo ratings yet
- Circulation WorksheetDocument3 pagesCirculation Worksheetholagato100% (1)
- CH 18 Cholesterol Metabolism: Biochem Block 3 NotesDocument38 pagesCH 18 Cholesterol Metabolism: Biochem Block 3 NotesJoseph KimNo ratings yet
- Respiratory System: Lab Interactive SessionDocument20 pagesRespiratory System: Lab Interactive SessionJoseph KimNo ratings yet
- HBV Antibody InterpretationDocument1 pageHBV Antibody InterpretationJoseph KimNo ratings yet
- Physio-DES-6 (Cardiac)Document56 pagesPhysio-DES-6 (Cardiac)Joseph Kim100% (1)
- Clinical Integration: Lymphatic & Respiratory SystemsDocument13 pagesClinical Integration: Lymphatic & Respiratory SystemsJoseph KimNo ratings yet
- Physio Lab CasesDocument4 pagesPhysio Lab CasesJoseph KimNo ratings yet
- Lymphatic System: Lab Interactive SessionDocument24 pagesLymphatic System: Lab Interactive SessionJoseph KimNo ratings yet
- Virus ClassificationDocument1 pageVirus ClassificationJoseph KimNo ratings yet
- Bernard Barber's Social System Theory: The American Sociologist June 2002Document20 pagesBernard Barber's Social System Theory: The American Sociologist June 2002Rainman1618No ratings yet
- DRUG NAME: Octreotide: Synonym (S) : Common Trade Name (S) : ClassificationDocument9 pagesDRUG NAME: Octreotide: Synonym (S) : Common Trade Name (S) : ClassificationChandanaSanjeeNo ratings yet
- Grade 6 - e A Tire Tracks Lesson 4Document3 pagesGrade 6 - e A Tire Tracks Lesson 4api-283081427No ratings yet
- Surveying For Highways: Eng. Suneth Thushara Highwy Design Division RDADocument31 pagesSurveying For Highways: Eng. Suneth Thushara Highwy Design Division RDAzeshan habibNo ratings yet
- NotingDocument160 pagesNotingdpkonnetNo ratings yet
- Verbal Communic-WPS OfficeDocument4 pagesVerbal Communic-WPS Officechandy RendajeNo ratings yet
- Sport Management Review: Evald Bundgaard Iversen, Graham CuskellyDocument13 pagesSport Management Review: Evald Bundgaard Iversen, Graham CuskellyGabriela Ioana IonitaNo ratings yet
- Cookie Business PlanDocument27 pagesCookie Business PlanLiza Mhey AcedoNo ratings yet
- Reading in Philippines HistoryDocument7 pagesReading in Philippines Historyrafaelalmazar416No ratings yet
- Nagunni 1Document2 pagesNagunni 1mayank.sharmaNo ratings yet
- FINAL TERM P.E.H. 12 Demonstrate Proper Etiquette and Safety in The Use of Facilities and Equipment For Dance ActivitiesDocument3 pagesFINAL TERM P.E.H. 12 Demonstrate Proper Etiquette and Safety in The Use of Facilities and Equipment For Dance Activitiesrandolf wassigNo ratings yet
- Give The Lord Glory and Honor (Psalm 96)Document1 pageGive The Lord Glory and Honor (Psalm 96)Lionel Valdellon100% (1)
- Dhan Allyn Romero 11 Saturn ABM EAPPDocument7 pagesDhan Allyn Romero 11 Saturn ABM EAPPJhevie RanileNo ratings yet
- Megillah 3Document70 pagesMegillah 3Julian Ungar-SargonNo ratings yet
- Vijaya Bank ChanchalDocument2 pagesVijaya Bank ChanchalShubham sharmaNo ratings yet
- 2005 Nicolet National Bank Annual ReportDocument16 pages2005 Nicolet National Bank Annual ReportNicolet BankNo ratings yet
- Pokemon Fusion GeneratorDocument1 pagePokemon Fusion GeneratorFrost MourneNo ratings yet
- Anb Brochure Fietsroute Klaprozen Heuvelland enDocument4 pagesAnb Brochure Fietsroute Klaprozen Heuvelland enBella BossNo ratings yet
- Entertainment Weekly - February 19, 2016Document120 pagesEntertainment Weekly - February 19, 2016Prateek Herpersad100% (1)
- HRM BBA MBA Lec 789 Job Analysis and DesignDocument41 pagesHRM BBA MBA Lec 789 Job Analysis and Designrhmafia786No ratings yet
- DxdiagDocument35 pagesDxdiagCr DickyNo ratings yet
- Links 8400peliculasDocument385 pagesLinks 8400peliculasjulio floresNo ratings yet
- Mvno - Encik KunciDocument15 pagesMvno - Encik KunciJolliffe NicholasNo ratings yet
- IBM UML 2.0 Advanced NotationsDocument21 pagesIBM UML 2.0 Advanced NotationsKeerthana SubramanianNo ratings yet
- Book Review " THE GREAT GATSBY "Document5 pagesBook Review " THE GREAT GATSBY "sayemNo ratings yet
- Futuro (Will-Going To - P.C.)Document1 pageFuturo (Will-Going To - P.C.)carolina herreraNo ratings yet
- Accy 211 - Week 8 Tut HWDocument2 pagesAccy 211 - Week 8 Tut HWIsaac ElhageNo ratings yet
- De Los Santos II v. BarbosaDocument8 pagesDe Los Santos II v. BarbosaApril IsidroNo ratings yet
- Nervous System Worksheet1Document3 pagesNervous System Worksheet1fe jandugan0% (1)