
Presentaton On LBW Baby
Presentaton On LBW Baby
You might also like
- Practice Exam 2 OB NursingDocument21 pagesPractice Exam 2 OB NursingSpurgis Rickard91% (22)
- High Risk NewbornDocument76 pagesHigh Risk NewbornVijith.V.kumar92% (24)
- NIDCAPDocument38 pagesNIDCAPShahpb100% (3)
- Obst 8 - All Obstetrics 4 2021Document28 pagesObst 8 - All Obstetrics 4 2021Menna KamalNo ratings yet
- Low Birth WeightDocument22 pagesLow Birth Weightエド パジャロン100% (5)
- Nursing Education Assignment (UNIT PLAN) 1Document4 pagesNursing Education Assignment (UNIT PLAN) 1charanjit kaurNo ratings yet
- Medical Surgical Lesson Plan 1Document7 pagesMedical Surgical Lesson Plan 1charanjit kaur100% (2)
- Second Year B.SC Nursing Master PlanDocument3 pagesSecond Year B.SC Nursing Master Plancharanjit kaur100% (1)
- Garbha VruddhiDocument50 pagesGarbha VruddhiKumarNo ratings yet
- Care of Low Birth WeightDocument21 pagesCare of Low Birth WeightPrernaSharmaNo ratings yet
- NICU PPT Hypo and HyperthermiaDocument23 pagesNICU PPT Hypo and HyperthermiaelsawzgoodNo ratings yet
- Rama College of Nursing: Health Education OnDocument24 pagesRama College of Nursing: Health Education OnBrijesh Yadav100% (1)
- Management of Newborn HypothermiaDocument3 pagesManagement of Newborn HypothermiaYwagar YwagarNo ratings yet
- NUTRITIONAL AssessmentDocument46 pagesNUTRITIONAL AssessmentSonali Hazra50% (2)
- Seminar ON: Baby Friendly Hospital InitiativeDocument7 pagesSeminar ON: Baby Friendly Hospital InitiativeUmairah BashirNo ratings yet
- Prolactin Reflex (Milk Secretion Reflex)Document16 pagesProlactin Reflex (Milk Secretion Reflex)Juhi Johnson JadhavNo ratings yet
- Hirsch Sprung Disease NewDocument10 pagesHirsch Sprung Disease NewUday KumarNo ratings yet
- Introduction To Pediatric NursingDocument36 pagesIntroduction To Pediatric Nursingcharan poonia100% (2)
- IUGRDocument11 pagesIUGRAnastasiafynnNo ratings yet
- Small For Gestational AgeDocument36 pagesSmall For Gestational AgeBRYAN JOSEPH TIONGSONNo ratings yet
- Seminar ImnciDocument15 pagesSeminar Imnciseema devassy100% (1)
- Baby Friendly Hospital Initiative (Bfhi)Document9 pagesBaby Friendly Hospital Initiative (Bfhi)Ankita BramheNo ratings yet
- A Study To Evaluate The Effectiveness of Structured Teaching Program On Knowledge and Practice Regarding Kangaroo Mother Care Among Post Natal Mothers Having Low Birth Weight Babies 1Document9 pagesA Study To Evaluate The Effectiveness of Structured Teaching Program On Knowledge and Practice Regarding Kangaroo Mother Care Among Post Natal Mothers Having Low Birth Weight Babies 1Manisa ParidaNo ratings yet
- Management of Low Birth Weight BabiesDocument59 pagesManagement of Low Birth Weight BabiesKiran Khasa100% (2)
- Nbu Careplan WK 1Document4 pagesNbu Careplan WK 1MuhammadNo ratings yet
- National Health AgenciesDocument16 pagesNational Health AgenciesMadhuri JadhavNo ratings yet
- Anatomy &physiology JaundiceDocument2 pagesAnatomy &physiology JaundiceHCX dghhqNo ratings yet
- Newborn AssessmentDocument9 pagesNewborn Assessmentapi-237668254No ratings yet
- Community Health Nursing-II DiarrheaDocument4 pagesCommunity Health Nursing-II DiarrheaPriya bhattiNo ratings yet
- PerperiumDocument14 pagesPerperiumXo YemNo ratings yet
- Kangaroo Mother CareDocument9 pagesKangaroo Mother CareSREEDEVI T SURESHNo ratings yet
- Normal PuerperiumDocument3 pagesNormal PuerperiumarunshreerajendranNo ratings yet
- Maternal and Perinatal Outcome in Jaundice Complicating PregnancyDocument10 pagesMaternal and Perinatal Outcome in Jaundice Complicating PregnancymanognaaaaNo ratings yet
- Assessment of A New Born PPT LPDocument35 pagesAssessment of A New Born PPT LPBaldwin Hamzcorp Hamoonga100% (1)
- Nutritional ProgrammesDocument15 pagesNutritional ProgrammesRaman SamraoNo ratings yet
- Fetal DistressDocument37 pagesFetal DistressRp NdaNo ratings yet
- Assess The Effectiveness of Structured Teaching Programmed Regarding Collection of Cord Blood For Stem Cell Therapy at Bram Hospital of RaipurDocument7 pagesAssess The Effectiveness of Structured Teaching Programmed Regarding Collection of Cord Blood For Stem Cell Therapy at Bram Hospital of RaipurIJAR JOURNALNo ratings yet
- CPD Book and Patient PictureDocument6 pagesCPD Book and Patient PicturePriyaNo ratings yet
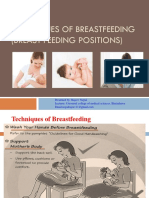
- Technique of Breast Feeding (Position of Breast Feeding)Document17 pagesTechnique of Breast Feeding (Position of Breast Feeding)Rajeev NepalNo ratings yet
- Newborn Assessment: IntroductionDocument16 pagesNewborn Assessment: Introductionsandeepv080% (1)
- CURRENT STATUS-WPS OfficeDocument35 pagesCURRENT STATUS-WPS OfficeVinnyNo ratings yet
- Breast FeedingDocument43 pagesBreast FeedingsindhujojoNo ratings yet
- IMNCIDocument47 pagesIMNCIRenuga SureshNo ratings yet
- Low Birth WeightDocument20 pagesLow Birth Weightsandhyaa7srinivassanNo ratings yet
- c14 p51 Nutritional Programmes in IndiaDocument13 pagesc14 p51 Nutritional Programmes in IndiaSrinivas Kasi0% (1)
- KMC FinalDocument36 pagesKMC FinalGandimarei100% (3)
- MCH ProgrammeDocument14 pagesMCH ProgrammepriyankaNo ratings yet
- New Born Assessment Format History CollectionDocument5 pagesNew Born Assessment Format History CollectionSherly MathewNo ratings yet
- Nursing Care of The High Risk NewbornDocument7 pagesNursing Care of The High Risk NewbornAbigail MangaoangNo ratings yet
- National Family Welfare ProgramDocument27 pagesNational Family Welfare ProgramBhawna JoshiNo ratings yet
- Border District Cluster StrategyDocument2 pagesBorder District Cluster StrategyRAJU100% (1)
- National Policy and Legislation in Relation To Child Health and WelfareDocument24 pagesNational Policy and Legislation in Relation To Child Health and Welfarerubinarashmi16100% (1)
- Care of Preterm Babies: Chinchu.MDocument59 pagesCare of Preterm Babies: Chinchu.MChinchu MohanNo ratings yet
- Presentation Abnormal PuerperiumDocument52 pagesPresentation Abnormal PuerperiumTesfaye AbebeNo ratings yet
- Food Adulteration $ Sbustance AbuseDocument22 pagesFood Adulteration $ Sbustance AbuseBabita Dhruw100% (1)
- Baby Friendly Hospital InitiativeDocument2 pagesBaby Friendly Hospital InitiativeChandu Raj100% (2)
- New Born AssessmentDocument42 pagesNew Born AssessmentBhawna Joshi100% (3)
- Case Presentation RVFDocument15 pagesCase Presentation RVFMeena Koushal100% (1)
- Assignment On Drugs Used For NewbornDocument11 pagesAssignment On Drugs Used For Newbornvarshasharma05100% (1)
- Antenatal AssessmentDocument7 pagesAntenatal Assessmentjayashreeselvaraj100% (1)
- Terminology CHNDocument4 pagesTerminology CHNKailash NagarNo ratings yet
- Reproductive and Child Health ProgrammeDocument14 pagesReproductive and Child Health ProgrammeDr Siddharth DarjiNo ratings yet
- Cpms College of Nursing Assignment ON Oral Medication: DATED: 18 MAY, 2021 Subject: Child Health NursingDocument4 pagesCpms College of Nursing Assignment ON Oral Medication: DATED: 18 MAY, 2021 Subject: Child Health NursingAmy LalringhluaniNo ratings yet
- Nursing Care PlansDocument6 pagesNursing Care PlansJhessa Curie PitaganNo ratings yet
- Care of Baby Under PhototherapyDocument4 pagesCare of Baby Under PhototherapyMary Menu100% (1)
- Icds Visit ReportDocument6 pagesIcds Visit ReportPunam Kar100% (1)
- High Risk New BornDocument12 pagesHigh Risk New BornM. jehovah Nissie YeshalomeNo ratings yet
- PrematurityDocument66 pagesPrematurityJolmajas JoharNo ratings yet
- S.G.R.D College of Nursing: AssignmentDocument3 pagesS.G.R.D College of Nursing: Assignmentcharanjit kaurNo ratings yet
- 2ND-Model DETAILDocument1 page2ND-Model DETAILcharanjit kaurNo ratings yet
- Demographic Data of The PatientDocument19 pagesDemographic Data of The Patientcharanjit kaurNo ratings yet
- CovaAppForRecruitmentsTests PDFDocument1 pageCovaAppForRecruitmentsTests PDFcharanjit kaurNo ratings yet
- Case-Presentation-on-Pem AdvanceDocument21 pagesCase-Presentation-on-Pem Advancecharanjit kaur100% (1)
- Assignment (Course Plan) 2Document3 pagesAssignment (Course Plan) 2charanjit kaurNo ratings yet
- 2ND-Model 2Document1 page2ND-Model 2charanjit kaurNo ratings yet
- Medical Surgical Seminar 2Document87 pagesMedical Surgical Seminar 2charanjit kaurNo ratings yet
- Medical Surgical Assignment 5Document2 pagesMedical Surgical Assignment 5charanjit kaurNo ratings yet
- Resume of RajaDocument2 pagesResume of Rajacharanjit kaurNo ratings yet
- M.S Drug StudyDocument9 pagesM.S Drug Studycharanjit kaurNo ratings yet
- Advance Assignmnet 4Document4 pagesAdvance Assignmnet 4charanjit kaurNo ratings yet
- Lesson Plan of Education (MS (Document9 pagesLesson Plan of Education (MS (charanjit kaurNo ratings yet
- Pediatric Nutritional AssessmentDocument51 pagesPediatric Nutritional Assessmentcharanjit kaur100% (1)
- Assignment On IMNCIDocument3 pagesAssignment On IMNCIcharanjit kaurNo ratings yet
- Health Talk On AnemiaDocument12 pagesHealth Talk On Anemiacharanjit kaurNo ratings yet
- 2.3. Mental Health Nursing: Course DescriptionDocument5 pages2.3. Mental Health Nursing: Course Descriptioncharanjit kaurNo ratings yet
- Seminar On Women EmpowermentDocument14 pagesSeminar On Women Empowermentcharanjit kaur0% (1)
- Problem Statement 1 (Autosaved) Real DimpyDocument8 pagesProblem Statement 1 (Autosaved) Real Dimpycharanjit kaurNo ratings yet
- Presentation Nursing EducationDocument22 pagesPresentation Nursing Educationcharanjit kaurNo ratings yet
- A QUASI SynopsisDocument9 pagesA QUASI Synopsischaranjit kaurNo ratings yet
- Master Plan For First Year. B.Sc. Nursing 2011-2012 X Batch: Lisie College of Nursing, Lisie Hospital, ErnakulamDocument1 pageMaster Plan For First Year. B.Sc. Nursing 2011-2012 X Batch: Lisie College of Nursing, Lisie Hospital, Ernakulamcharanjit kaurNo ratings yet
- NeoPREP 2011Document342 pagesNeoPREP 2011johnbarrow641No ratings yet
- Preeclampsia - Management and Prognosis - UpToDateDocument22 pagesPreeclampsia - Management and Prognosis - UpToDateNunung firda IstiqomahNo ratings yet
- OSCE On 14/3/2008: Describe Gynaecoid PelvisDocument82 pagesOSCE On 14/3/2008: Describe Gynaecoid PelvisKahing LiNo ratings yet
- Metabolic Syndrome in Pregnancy - Causes Dan Consequences - Muhammad Adrianes Bachnas, DR., SP - OG (K) - FM PDFDocument29 pagesMetabolic Syndrome in Pregnancy - Causes Dan Consequences - Muhammad Adrianes Bachnas, DR., SP - OG (K) - FM PDFcarissa rhezaNo ratings yet
- NZMFMN Obstetric Doppler Guideline 2015Document16 pagesNZMFMN Obstetric Doppler Guideline 2015Nat NivlaNo ratings yet
- اختصارات المندوه ObstetricsDocument11 pagesاختصارات المندوه ObstetricssamyNo ratings yet
- Problems Related To Prematurity, Post Maturity, Problems Related To Gestational WeightDocument88 pagesProblems Related To Prematurity, Post Maturity, Problems Related To Gestational WeightNikky SilvestreNo ratings yet
- Falla Respiratoria & Embarazo - Lapinsky 2015Document7 pagesFalla Respiratoria & Embarazo - Lapinsky 2015Fabiola Buelna GaxiolaNo ratings yet
- Level 1 Q& A Og - KoncptDocument14 pagesLevel 1 Q& A Og - KoncptadiNo ratings yet
- Nucleated Red Blood Cells in The Fetus and PDFDocument5 pagesNucleated Red Blood Cells in The Fetus and PDFYenny YuliantiNo ratings yet
- Intrauterine Growth Restriction IUGRDocument8 pagesIntrauterine Growth Restriction IUGRJyoti Prem UttamNo ratings yet
- Nursing Care of The High - Risk Newborn To 2018Document325 pagesNursing Care of The High - Risk Newborn To 2018Keane Andal67% (3)
- Chapter 28 PROMDocument24 pagesChapter 28 PROMTansya PurnaningrumNo ratings yet
- What Is RH IncompatibilityDocument22 pagesWhat Is RH IncompatibilityKimsha ConcepcionNo ratings yet
- Selective IUGRDocument6 pagesSelective IUGRMeycha Da FhonsaNo ratings yet
- Failure To Thrive - AAPDocument11 pagesFailure To Thrive - AAPAlexNo ratings yet
- Pediatrics Case: Demographic DataDocument9 pagesPediatrics Case: Demographic DataAnurag SuryawanshiNo ratings yet
- Fetal Growth Restriction: Presenter - DR Mitali and DR Vani Moderator-Dr - Rashmi and DR ShafaqDocument53 pagesFetal Growth Restriction: Presenter - DR Mitali and DR Vani Moderator-Dr - Rashmi and DR ShafaqVani BallaNo ratings yet
- M. Preterm and Postterm - NewDocument92 pagesM. Preterm and Postterm - NewTry Ariditya UtomoNo ratings yet
- Jurnal Kesehatan Masyarakat: Health, Food Consumption, Social Economy, and Stunting Inci-Dency in Timor LesteDocument9 pagesJurnal Kesehatan Masyarakat: Health, Food Consumption, Social Economy, and Stunting Inci-Dency in Timor LesteYubeth LedohNo ratings yet
- Malnutrition e BD 12Document51 pagesMalnutrition e BD 12dr.vichiayorinaNo ratings yet
- Cme (Tdhi)Document64 pagesCme (Tdhi)OB-Gyne TDHINo ratings yet
- Isuog Guideline IugrDocument15 pagesIsuog Guideline Iugreric100% (1)
- Caton e Hess 2010 - Maternal Plane of Nutrition and Impact On The OffspringDocument16 pagesCaton e Hess 2010 - Maternal Plane of Nutrition and Impact On The OffspringsousamapNo ratings yet
- APM201 04 Olaya UmbilicalDocument6 pagesAPM201 04 Olaya UmbilicalYoshua Ulido SimangunsongNo ratings yet
















































































































Download as pptx, pdf, or txt
You might also like
- Practice Exam 2 OB NursingDocument21 pagesPractice Exam 2 OB NursingSpurgis Rickard91% (22)
- High Risk NewbornDocument76 pagesHigh Risk NewbornVijith.V.kumar92% (24)
- NIDCAPDocument38 pagesNIDCAPShahpb100% (3)
- Obst 8 - All Obstetrics 4 2021Document28 pagesObst 8 - All Obstetrics 4 2021Menna KamalNo ratings yet
- Low Birth WeightDocument22 pagesLow Birth Weightエド パジャロン100% (5)
- Nursing Education Assignment (UNIT PLAN) 1Document4 pagesNursing Education Assignment (UNIT PLAN) 1charanjit kaurNo ratings yet
- Medical Surgical Lesson Plan 1Document7 pagesMedical Surgical Lesson Plan 1charanjit kaur100% (2)
- Second Year B.SC Nursing Master PlanDocument3 pagesSecond Year B.SC Nursing Master Plancharanjit kaur100% (1)
- Garbha VruddhiDocument50 pagesGarbha VruddhiKumarNo ratings yet
- Care of Low Birth WeightDocument21 pagesCare of Low Birth WeightPrernaSharmaNo ratings yet
- NICU PPT Hypo and HyperthermiaDocument23 pagesNICU PPT Hypo and HyperthermiaelsawzgoodNo ratings yet
- Rama College of Nursing: Health Education OnDocument24 pagesRama College of Nursing: Health Education OnBrijesh Yadav100% (1)
- Management of Newborn HypothermiaDocument3 pagesManagement of Newborn HypothermiaYwagar YwagarNo ratings yet
- NUTRITIONAL AssessmentDocument46 pagesNUTRITIONAL AssessmentSonali Hazra50% (2)
- Seminar ON: Baby Friendly Hospital InitiativeDocument7 pagesSeminar ON: Baby Friendly Hospital InitiativeUmairah BashirNo ratings yet
- Prolactin Reflex (Milk Secretion Reflex)Document16 pagesProlactin Reflex (Milk Secretion Reflex)Juhi Johnson JadhavNo ratings yet
- Hirsch Sprung Disease NewDocument10 pagesHirsch Sprung Disease NewUday KumarNo ratings yet
- Introduction To Pediatric NursingDocument36 pagesIntroduction To Pediatric Nursingcharan poonia100% (2)
- IUGRDocument11 pagesIUGRAnastasiafynnNo ratings yet
- Small For Gestational AgeDocument36 pagesSmall For Gestational AgeBRYAN JOSEPH TIONGSONNo ratings yet
- Seminar ImnciDocument15 pagesSeminar Imnciseema devassy100% (1)
- Baby Friendly Hospital Initiative (Bfhi)Document9 pagesBaby Friendly Hospital Initiative (Bfhi)Ankita BramheNo ratings yet
- A Study To Evaluate The Effectiveness of Structured Teaching Program On Knowledge and Practice Regarding Kangaroo Mother Care Among Post Natal Mothers Having Low Birth Weight Babies 1Document9 pagesA Study To Evaluate The Effectiveness of Structured Teaching Program On Knowledge and Practice Regarding Kangaroo Mother Care Among Post Natal Mothers Having Low Birth Weight Babies 1Manisa ParidaNo ratings yet
- Management of Low Birth Weight BabiesDocument59 pagesManagement of Low Birth Weight BabiesKiran Khasa100% (2)
- Nbu Careplan WK 1Document4 pagesNbu Careplan WK 1MuhammadNo ratings yet
- National Health AgenciesDocument16 pagesNational Health AgenciesMadhuri JadhavNo ratings yet
- Anatomy &physiology JaundiceDocument2 pagesAnatomy &physiology JaundiceHCX dghhqNo ratings yet
- Newborn AssessmentDocument9 pagesNewborn Assessmentapi-237668254No ratings yet
- Community Health Nursing-II DiarrheaDocument4 pagesCommunity Health Nursing-II DiarrheaPriya bhattiNo ratings yet
- PerperiumDocument14 pagesPerperiumXo YemNo ratings yet
- Kangaroo Mother CareDocument9 pagesKangaroo Mother CareSREEDEVI T SURESHNo ratings yet
- Normal PuerperiumDocument3 pagesNormal PuerperiumarunshreerajendranNo ratings yet
- Maternal and Perinatal Outcome in Jaundice Complicating PregnancyDocument10 pagesMaternal and Perinatal Outcome in Jaundice Complicating PregnancymanognaaaaNo ratings yet
- Assessment of A New Born PPT LPDocument35 pagesAssessment of A New Born PPT LPBaldwin Hamzcorp Hamoonga100% (1)
- Nutritional ProgrammesDocument15 pagesNutritional ProgrammesRaman SamraoNo ratings yet
- Fetal DistressDocument37 pagesFetal DistressRp NdaNo ratings yet
- Assess The Effectiveness of Structured Teaching Programmed Regarding Collection of Cord Blood For Stem Cell Therapy at Bram Hospital of RaipurDocument7 pagesAssess The Effectiveness of Structured Teaching Programmed Regarding Collection of Cord Blood For Stem Cell Therapy at Bram Hospital of RaipurIJAR JOURNALNo ratings yet
- CPD Book and Patient PictureDocument6 pagesCPD Book and Patient PicturePriyaNo ratings yet
- Technique of Breast Feeding (Position of Breast Feeding)Document17 pagesTechnique of Breast Feeding (Position of Breast Feeding)Rajeev NepalNo ratings yet
- Newborn Assessment: IntroductionDocument16 pagesNewborn Assessment: Introductionsandeepv080% (1)
- CURRENT STATUS-WPS OfficeDocument35 pagesCURRENT STATUS-WPS OfficeVinnyNo ratings yet
- Breast FeedingDocument43 pagesBreast FeedingsindhujojoNo ratings yet
- IMNCIDocument47 pagesIMNCIRenuga SureshNo ratings yet
- Low Birth WeightDocument20 pagesLow Birth Weightsandhyaa7srinivassanNo ratings yet
- c14 p51 Nutritional Programmes in IndiaDocument13 pagesc14 p51 Nutritional Programmes in IndiaSrinivas Kasi0% (1)
- KMC FinalDocument36 pagesKMC FinalGandimarei100% (3)
- MCH ProgrammeDocument14 pagesMCH ProgrammepriyankaNo ratings yet
- New Born Assessment Format History CollectionDocument5 pagesNew Born Assessment Format History CollectionSherly MathewNo ratings yet
- Nursing Care of The High Risk NewbornDocument7 pagesNursing Care of The High Risk NewbornAbigail MangaoangNo ratings yet
- National Family Welfare ProgramDocument27 pagesNational Family Welfare ProgramBhawna JoshiNo ratings yet
- Border District Cluster StrategyDocument2 pagesBorder District Cluster StrategyRAJU100% (1)
- National Policy and Legislation in Relation To Child Health and WelfareDocument24 pagesNational Policy and Legislation in Relation To Child Health and Welfarerubinarashmi16100% (1)
- Care of Preterm Babies: Chinchu.MDocument59 pagesCare of Preterm Babies: Chinchu.MChinchu MohanNo ratings yet
- Presentation Abnormal PuerperiumDocument52 pagesPresentation Abnormal PuerperiumTesfaye AbebeNo ratings yet
- Food Adulteration $ Sbustance AbuseDocument22 pagesFood Adulteration $ Sbustance AbuseBabita Dhruw100% (1)
- Baby Friendly Hospital InitiativeDocument2 pagesBaby Friendly Hospital InitiativeChandu Raj100% (2)
- New Born AssessmentDocument42 pagesNew Born AssessmentBhawna Joshi100% (3)
- Case Presentation RVFDocument15 pagesCase Presentation RVFMeena Koushal100% (1)
- Assignment On Drugs Used For NewbornDocument11 pagesAssignment On Drugs Used For Newbornvarshasharma05100% (1)
- Antenatal AssessmentDocument7 pagesAntenatal Assessmentjayashreeselvaraj100% (1)
- Terminology CHNDocument4 pagesTerminology CHNKailash NagarNo ratings yet
- Reproductive and Child Health ProgrammeDocument14 pagesReproductive and Child Health ProgrammeDr Siddharth DarjiNo ratings yet
- Cpms College of Nursing Assignment ON Oral Medication: DATED: 18 MAY, 2021 Subject: Child Health NursingDocument4 pagesCpms College of Nursing Assignment ON Oral Medication: DATED: 18 MAY, 2021 Subject: Child Health NursingAmy LalringhluaniNo ratings yet
- Nursing Care PlansDocument6 pagesNursing Care PlansJhessa Curie PitaganNo ratings yet
- Care of Baby Under PhototherapyDocument4 pagesCare of Baby Under PhototherapyMary Menu100% (1)
- Icds Visit ReportDocument6 pagesIcds Visit ReportPunam Kar100% (1)
- High Risk New BornDocument12 pagesHigh Risk New BornM. jehovah Nissie YeshalomeNo ratings yet
- PrematurityDocument66 pagesPrematurityJolmajas JoharNo ratings yet
- S.G.R.D College of Nursing: AssignmentDocument3 pagesS.G.R.D College of Nursing: Assignmentcharanjit kaurNo ratings yet
- 2ND-Model DETAILDocument1 page2ND-Model DETAILcharanjit kaurNo ratings yet
- Demographic Data of The PatientDocument19 pagesDemographic Data of The Patientcharanjit kaurNo ratings yet
- CovaAppForRecruitmentsTests PDFDocument1 pageCovaAppForRecruitmentsTests PDFcharanjit kaurNo ratings yet
- Case-Presentation-on-Pem AdvanceDocument21 pagesCase-Presentation-on-Pem Advancecharanjit kaur100% (1)
- Assignment (Course Plan) 2Document3 pagesAssignment (Course Plan) 2charanjit kaurNo ratings yet
- 2ND-Model 2Document1 page2ND-Model 2charanjit kaurNo ratings yet
- Medical Surgical Seminar 2Document87 pagesMedical Surgical Seminar 2charanjit kaurNo ratings yet
- Medical Surgical Assignment 5Document2 pagesMedical Surgical Assignment 5charanjit kaurNo ratings yet
- Resume of RajaDocument2 pagesResume of Rajacharanjit kaurNo ratings yet
- M.S Drug StudyDocument9 pagesM.S Drug Studycharanjit kaurNo ratings yet
- Advance Assignmnet 4Document4 pagesAdvance Assignmnet 4charanjit kaurNo ratings yet
- Lesson Plan of Education (MS (Document9 pagesLesson Plan of Education (MS (charanjit kaurNo ratings yet
- Pediatric Nutritional AssessmentDocument51 pagesPediatric Nutritional Assessmentcharanjit kaur100% (1)
- Assignment On IMNCIDocument3 pagesAssignment On IMNCIcharanjit kaurNo ratings yet
- Health Talk On AnemiaDocument12 pagesHealth Talk On Anemiacharanjit kaurNo ratings yet
- 2.3. Mental Health Nursing: Course DescriptionDocument5 pages2.3. Mental Health Nursing: Course Descriptioncharanjit kaurNo ratings yet
- Seminar On Women EmpowermentDocument14 pagesSeminar On Women Empowermentcharanjit kaur0% (1)
- Problem Statement 1 (Autosaved) Real DimpyDocument8 pagesProblem Statement 1 (Autosaved) Real Dimpycharanjit kaurNo ratings yet
- Presentation Nursing EducationDocument22 pagesPresentation Nursing Educationcharanjit kaurNo ratings yet
- A QUASI SynopsisDocument9 pagesA QUASI Synopsischaranjit kaurNo ratings yet
- Master Plan For First Year. B.Sc. Nursing 2011-2012 X Batch: Lisie College of Nursing, Lisie Hospital, ErnakulamDocument1 pageMaster Plan For First Year. B.Sc. Nursing 2011-2012 X Batch: Lisie College of Nursing, Lisie Hospital, Ernakulamcharanjit kaurNo ratings yet
- NeoPREP 2011Document342 pagesNeoPREP 2011johnbarrow641No ratings yet
- Preeclampsia - Management and Prognosis - UpToDateDocument22 pagesPreeclampsia - Management and Prognosis - UpToDateNunung firda IstiqomahNo ratings yet
- OSCE On 14/3/2008: Describe Gynaecoid PelvisDocument82 pagesOSCE On 14/3/2008: Describe Gynaecoid PelvisKahing LiNo ratings yet
- Metabolic Syndrome in Pregnancy - Causes Dan Consequences - Muhammad Adrianes Bachnas, DR., SP - OG (K) - FM PDFDocument29 pagesMetabolic Syndrome in Pregnancy - Causes Dan Consequences - Muhammad Adrianes Bachnas, DR., SP - OG (K) - FM PDFcarissa rhezaNo ratings yet
- NZMFMN Obstetric Doppler Guideline 2015Document16 pagesNZMFMN Obstetric Doppler Guideline 2015Nat NivlaNo ratings yet
- اختصارات المندوه ObstetricsDocument11 pagesاختصارات المندوه ObstetricssamyNo ratings yet
- Problems Related To Prematurity, Post Maturity, Problems Related To Gestational WeightDocument88 pagesProblems Related To Prematurity, Post Maturity, Problems Related To Gestational WeightNikky SilvestreNo ratings yet
- Falla Respiratoria & Embarazo - Lapinsky 2015Document7 pagesFalla Respiratoria & Embarazo - Lapinsky 2015Fabiola Buelna GaxiolaNo ratings yet
- Level 1 Q& A Og - KoncptDocument14 pagesLevel 1 Q& A Og - KoncptadiNo ratings yet
- Nucleated Red Blood Cells in The Fetus and PDFDocument5 pagesNucleated Red Blood Cells in The Fetus and PDFYenny YuliantiNo ratings yet
- Intrauterine Growth Restriction IUGRDocument8 pagesIntrauterine Growth Restriction IUGRJyoti Prem UttamNo ratings yet
- Nursing Care of The High - Risk Newborn To 2018Document325 pagesNursing Care of The High - Risk Newborn To 2018Keane Andal67% (3)
- Chapter 28 PROMDocument24 pagesChapter 28 PROMTansya PurnaningrumNo ratings yet
- What Is RH IncompatibilityDocument22 pagesWhat Is RH IncompatibilityKimsha ConcepcionNo ratings yet
- Selective IUGRDocument6 pagesSelective IUGRMeycha Da FhonsaNo ratings yet
- Failure To Thrive - AAPDocument11 pagesFailure To Thrive - AAPAlexNo ratings yet
- Pediatrics Case: Demographic DataDocument9 pagesPediatrics Case: Demographic DataAnurag SuryawanshiNo ratings yet
- Fetal Growth Restriction: Presenter - DR Mitali and DR Vani Moderator-Dr - Rashmi and DR ShafaqDocument53 pagesFetal Growth Restriction: Presenter - DR Mitali and DR Vani Moderator-Dr - Rashmi and DR ShafaqVani BallaNo ratings yet
- M. Preterm and Postterm - NewDocument92 pagesM. Preterm and Postterm - NewTry Ariditya UtomoNo ratings yet
- Jurnal Kesehatan Masyarakat: Health, Food Consumption, Social Economy, and Stunting Inci-Dency in Timor LesteDocument9 pagesJurnal Kesehatan Masyarakat: Health, Food Consumption, Social Economy, and Stunting Inci-Dency in Timor LesteYubeth LedohNo ratings yet
- Malnutrition e BD 12Document51 pagesMalnutrition e BD 12dr.vichiayorinaNo ratings yet
- Cme (Tdhi)Document64 pagesCme (Tdhi)OB-Gyne TDHINo ratings yet
- Isuog Guideline IugrDocument15 pagesIsuog Guideline Iugreric100% (1)
- Caton e Hess 2010 - Maternal Plane of Nutrition and Impact On The OffspringDocument16 pagesCaton e Hess 2010 - Maternal Plane of Nutrition and Impact On The OffspringsousamapNo ratings yet
- APM201 04 Olaya UmbilicalDocument6 pagesAPM201 04 Olaya UmbilicalYoshua Ulido SimangunsongNo ratings yet