Download as pptx, pdf, or txt
You might also like
- 5-Neuro MCQs Final UnsolvedDocument29 pages5-Neuro MCQs Final UnsolvedOsman Somi25% (4)
- Aortic Dissection PP PresentationDocument64 pagesAortic Dissection PP PresentationKonstantin DimitrovNo ratings yet
- CNS Congenital AnomaliesDocument74 pagesCNS Congenital AnomaliesMoh DrhusseinyNo ratings yet
- Radiologi DR Budi - Pediatric Congenital Neurological DiseasesDocument30 pagesRadiologi DR Budi - Pediatric Congenital Neurological DiseasesPusparasmi Mas Ayu SuprabhaNo ratings yet
- Micro and MacrocephalyDocument27 pagesMicro and MacrocephalyAbdullah GadNo ratings yet
- Chiari MalformationDocument3 pagesChiari MalformationAloysius RodriguesNo ratings yet
- Neck Dissections: DR P Lalityaswarna II ND Yr ResidentDocument79 pagesNeck Dissections: DR P Lalityaswarna II ND Yr ResidentSee GooMeNo ratings yet
- Surgical Endocrinology: University of Virginia Clinical Clerkship in Surgery Peter I. Ellman M.DDocument78 pagesSurgical Endocrinology: University of Virginia Clinical Clerkship in Surgery Peter I. Ellman M.DoctoindradjajaNo ratings yet
- Congenital Malformations of The BrainDocument57 pagesCongenital Malformations of The Brainmanisha paikarayNo ratings yet
- Congenital Aural AtresiaDocument34 pagesCongenital Aural Atresia李丞永No ratings yet
- Legg Calve PerthesDocument93 pagesLegg Calve PerthesAkshay LakraNo ratings yet
- Branchial Anomalies: David Gleinser, MD Harold Pine, MDDocument51 pagesBranchial Anomalies: David Gleinser, MD Harold Pine, MDDrsreeram ValluriNo ratings yet
- Head Neck-Pharynx Larynx Thyroid GlandDocument8 pagesHead Neck-Pharynx Larynx Thyroid GlandMe MyselfNo ratings yet
- Mandibulofacial Dysostosis, Also Known As Treacher CollinsDocument19 pagesMandibulofacial Dysostosis, Also Known As Treacher CollinsMoe KebabNo ratings yet
- Zitelli Picture Review - GeneticsDocument101 pagesZitelli Picture Review - GeneticsEllagEszNo ratings yet
- Hydro Cep Hal UsDocument11 pagesHydro Cep Hal UsEmmanuel MukukaNo ratings yet
- Neck LumpsDocument27 pagesNeck Lumpsfrabzi100% (1)
- Syringomyelia, Arachnoiditis and SpasticityDocument53 pagesSyringomyelia, Arachnoiditis and SpasticitySam OlukaNo ratings yet
- Congenital Brain Anomalies: Dr. Dev LakheraDocument61 pagesCongenital Brain Anomalies: Dr. Dev LakheraNinaNo ratings yet
- 06 Pediatrics CNS MCQDocument46 pages06 Pediatrics CNS MCQMalinda KarunaratneNo ratings yet
- RADIOLOGI - NEURORADIOLOGI 2 - Dr. Farah - Kelas ADocument106 pagesRADIOLOGI - NEURORADIOLOGI 2 - Dr. Farah - Kelas ASeno TanubrataNo ratings yet
- Arnold Chiari MalformationDocument9 pagesArnold Chiari MalformationRahul Teja GNo ratings yet
- Hydrocephalus by MacDocument44 pagesHydrocephalus by MacMacktevin FraterinNo ratings yet
- SurgeryspecimensDocument81 pagesSurgeryspecimensHimanshu BadjatyaNo ratings yet
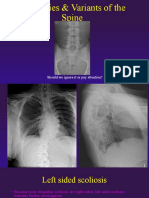
- Anomalies Variants of The SpineDocument41 pagesAnomalies Variants of The SpinekinexNo ratings yet
- Neurosurgery Congenital Anomalies: Types & DefinitionsDocument41 pagesNeurosurgery Congenital Anomalies: Types & DefinitionsMAY100% (1)
- Anaesthesia For BurnsDocument51 pagesAnaesthesia For BurnsAnulatkNo ratings yet
- NS 2 - Developmental Diseases of The Nervous System v2023.02Document49 pagesNS 2 - Developmental Diseases of The Nervous System v2023.02t4gjzhpfjcNo ratings yet
- JainamDocument20 pagesJainamSpandan KadamNo ratings yet
- Chiari MalformationsDocument23 pagesChiari MalformationsRoxana BociocNo ratings yet
- Dezvoltare A Creierului Care Poate Fi: HidrocefalieiDocument35 pagesDezvoltare A Creierului Care Poate Fi: HidrocefalieitatianarusuNo ratings yet
- Pharyngeal ApparatusDocument146 pagesPharyngeal ApparatusNastronamia HDNo ratings yet
- Hydrocephalus AND Spina Bifida: MR - Sachin T.Gadade M.SC (N) PediatricsDocument61 pagesHydrocephalus AND Spina Bifida: MR - Sachin T.Gadade M.SC (N) PediatricsAbdirahman Abdillahi FarahNo ratings yet
- NeckdissectionsDocument130 pagesNeckdissectionsAlvaro RivCalleNo ratings yet
- SYRINGOMYELIADocument31 pagesSYRINGOMYELIAPreeti SharmaNo ratings yet
- Spinal Deformities NewDocument79 pagesSpinal Deformities Newapi-26159412100% (3)
- Neck LumpDocument18 pagesNeck LumpJosh BurkeNo ratings yet
- Iskandar Chiari Syringomyelia ASAP 2010Document25 pagesIskandar Chiari Syringomyelia ASAP 2010Hitesh RohitNo ratings yet
- Neural Tube DefectsDocument51 pagesNeural Tube DefectsSaddat kyajjaNo ratings yet
- Cervical SpineDocument51 pagesCervical SpineEvandiar IzwardyNo ratings yet
- Brainstem Evoked ResponseDocument57 pagesBrainstem Evoked ResponseGerald PagalingNo ratings yet
- Cognition in Chiari Malformation Type IDocument22 pagesCognition in Chiari Malformation Type IMarlene LírioNo ratings yet
- NECK AnatomyzkkDocument38 pagesNECK AnatomyzkkzahidNo ratings yet
- Cranio Syn Ostos IsDocument18 pagesCranio Syn Ostos IsEzekiel ArtetaNo ratings yet
- Ortho Zusammenfassung 2020Document258 pagesOrtho Zusammenfassung 2020Aastha SethNo ratings yet
- The Head and Neck AnatomyDocument39 pagesThe Head and Neck AnatomySwati LataNo ratings yet
- HYDROCEPHALUSDocument63 pagesHYDROCEPHALUSJohnsatish Rudrapogu50% (2)
- Neck Trauma LecDocument49 pagesNeck Trauma Lecapi-3743483100% (2)
- Pediatric - Hearing - Loss Lau 3-17-10Document45 pagesPediatric - Hearing - Loss Lau 3-17-10Arief FakhrizalNo ratings yet
- Thyroid UltrasoundDocument62 pagesThyroid UltrasoundYoungFanjiens100% (1)
- Pathogenesis and TCM Treatment of Cervical Herniated Disc: East West Healing Center by Dr. Leon ChenDocument68 pagesPathogenesis and TCM Treatment of Cervical Herniated Disc: East West Healing Center by Dr. Leon ChenArtha PutuNo ratings yet
- SurgeryspecimensDocument81 pagesSurgeryspecimensHimanshu BadjatyaNo ratings yet
- DDH Lecture PDFDocument126 pagesDDH Lecture PDFSameh AbdelaalNo ratings yet
- Arnold Chiari Malformation: With SyringomyeliaDocument17 pagesArnold Chiari Malformation: With SyringomyeliaLeslie ManleyNo ratings yet
- ThyroidDocument51 pagesThyroid3rd yrsNo ratings yet
- Pediatric IssuesDocument21 pagesPediatric Issuesapi-3700579No ratings yet
- Neck MassesDocument52 pagesNeck MassesRaman Prasad SharmaNo ratings yet
- Embryology of The Neck & Neck MassesDocument52 pagesEmbryology of The Neck & Neck MassesArfian Deny PNo ratings yet
- Justin PT NanguneriDocument53 pagesJustin PT NanguneriJustin Xaviour dhasNo ratings yet
- Spinal ImagingDocument311 pagesSpinal ImagingguillaumarNo ratings yet
- Alternating Horner Syndrome: Case Report and Review of The LiteratureDocument4 pagesAlternating Horner Syndrome: Case Report and Review of The LiteratureDanielle SangalangNo ratings yet
- Internal Medicine II - NEUROLOGY CASESDocument33 pagesInternal Medicine II - NEUROLOGY CASESAhmad SobihNo ratings yet
- 5.nervous System PDFDocument88 pages5.nervous System PDFMelancholy MedicineNo ratings yet
- SCI Acute Care and Rehabilitation PT 2009Document265 pagesSCI Acute Care and Rehabilitation PT 2009api-3822828No ratings yet
- Pathology of CNS: Eric M. Mirandilla MD, DPSPDocument71 pagesPathology of CNS: Eric M. Mirandilla MD, DPSPDhruva PatelNo ratings yet
- Causes of Weakness of Lower Limbs by DR Bashir Ahmed Dar Chinkipora Sopore KashmirDocument23 pagesCauses of Weakness of Lower Limbs by DR Bashir Ahmed Dar Chinkipora Sopore KashmirProf Dr Bashir Ahmed Dar Chinki Pora Sopore Kashmir100% (1)
- Pain Pada SyringomyeliaDocument6 pagesPain Pada Syringomyeliavico julendiNo ratings yet
- Neuro Tract Lesions Ps230114Document16 pagesNeuro Tract Lesions Ps230114সোমনাথ মহাপাত্রNo ratings yet
- Pediatric RehabDocument32 pagesPediatric RehabRainy DaysNo ratings yet
- Pathophysiology of SyringomyeliaDocument14 pagesPathophysiology of SyringomyeliaGerardo100% (2)
- Syringomyelia in Neuromyelitis Optica Seropositive For Aquaporin-4 Antibody: A Case ReportDocument4 pagesSyringomyelia in Neuromyelitis Optica Seropositive For Aquaporin-4 Antibody: A Case ReportIJAR JOURNALNo ratings yet
- Dias 2013Document12 pagesDias 2013Santiago Diaz PinillosNo ratings yet
- SYRINGOMYELIADocument16 pagesSYRINGOMYELIAkyki ab100% (2)
- Case Study Intramedullary Spinal Cord TumorDocument13 pagesCase Study Intramedullary Spinal Cord TumorCitra KristiNo ratings yet
- Arnold Chiari Malformation & SyringomyeliaDocument38 pagesArnold Chiari Malformation & SyringomyeliaBojan PavlovicNo ratings yet
- Bmjopen 2020 January 10 1 Inline Supplementary Material 1Document31 pagesBmjopen 2020 January 10 1 Inline Supplementary Material 1mazen alkarras100% (1)
- Boli Vertebro MedulareDocument12 pagesBoli Vertebro MedulareHalit DianaNo ratings yet
- Qstream-1 2Document55 pagesQstream-1 2Vijay100% (1)
- Motor neurone disease د.رشاد عبدالغنيDocument18 pagesMotor neurone disease د.رشاد عبدالغنيMohammad BelbahaithNo ratings yet
- Medscape Spina BifidaDocument25 pagesMedscape Spina Bifidarica dhamayantiNo ratings yet
- Spinal Cord Disease by GadisaDocument128 pagesSpinal Cord Disease by GadisaGadisa DejeneNo ratings yet
- Term 2 Fall 2018Document90 pagesTerm 2 Fall 2018Artemio ZavalaNo ratings yet
- CNS M1 Lecture Slides Compiled, DR OsaiDocument185 pagesCNS M1 Lecture Slides Compiled, DR OsaiMusaNo ratings yet
- SpinaBifida ManagementDocument4 pagesSpinaBifida ManagementDimple GoyalNo ratings yet
- Spina Biphida. N Engl J Med 2022Document7 pagesSpina Biphida. N Engl J Med 2022JUAN GUAPO MENDOZANo ratings yet
- MeningomyeloceleDocument42 pagesMeningomyeloceleSundaraBharathiNo ratings yet
- Scoliosis A Case Study in An Adolescent BoyDocument9 pagesScoliosis A Case Study in An Adolescent BoyJAZMYNN ANNE ALCANTARANo ratings yet